
Abstract
Aim:
Insulin therapy induces remission in subjects with newly diagnosed type 2 diabetes mellitus (T2DM). This study assessed the insulin and C-peptide levels in newly diagnosed T2DM subjects during low-dose insulin therapy.
Subjects and Methods:
Twenty newly diagnosed, drug-naive, T2DM patients without acute or chronic complications were the subjects for this study. Premixed insulin (70/30), 16 units, as two divided doses, was started for all subjects after preliminary investigations. The same dose of insulin was continued until normoglycemia was achieved. Subsequently the insulin dose was down-titrated. Plasma insulin, C-peptide, and blood glucose (both fasting and after breakfast) were measured at baseline and monthly for 6 months. Body weight and glycosylated hemoglobin (HbA1c) were measured every 3 months and the lipid profile was obtained at baseline and at 6 months.
Results:
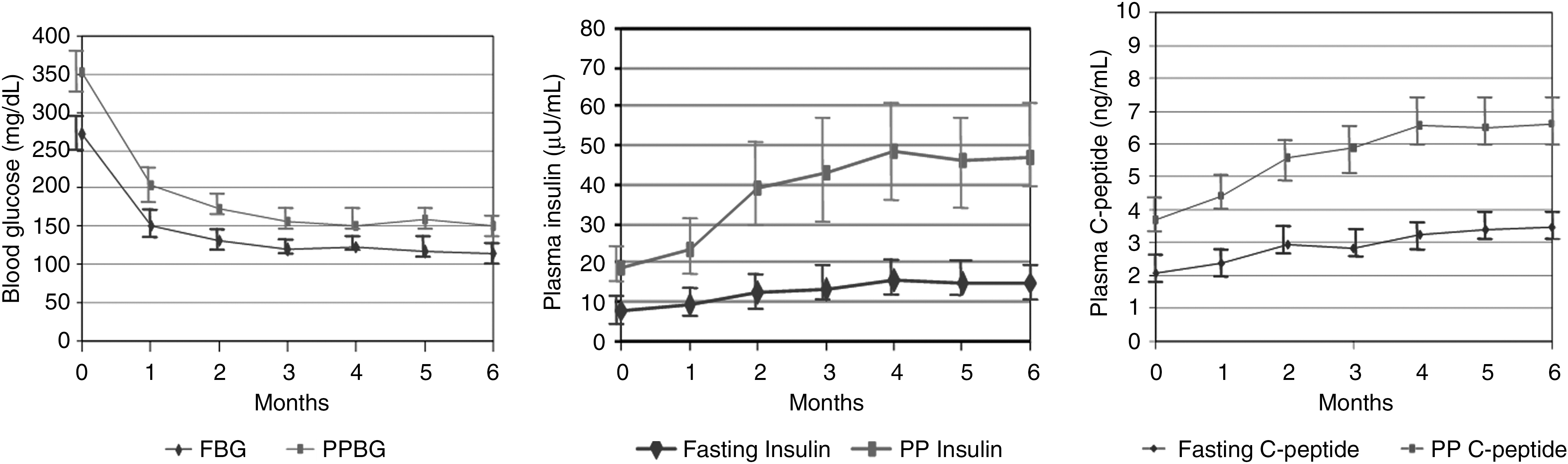
Blood glucose levels showed a rapid decreasing trend and reached the near-normoglycemic range by 3 months, whereas plasma insulin and C-peptide showed a slow and steady increase until the fourth month and remained the same during the next 2 months of follow-up. HbA1c was 11.3 ± 1.4% (range, 8.6–13.5%) and 7.05 ± 0.54% (range, 6.3–8.1%) at the time of diagnosis and at the end of 6 months, respectively. The mean weights of the study subjects at baseline and 3 and 6 months were 70 ± 16 kg (range, 44–95 kg), 68 ± 13 kg, and 68 ± 13 kg (P = 0.083), respectively. Total cholesterol, low-density lipoprotein-cholesterol, and triglycerides decreased, whereas high-density lipoprotein-cholesterol was higher at 6 months.
Conclusion:
Low-dose insulin therapy in newly diagnosed T2DM leads to β-cell recovery (as documented by plasma insulin and C-peptide levels) by 3–4 months.
Introduction
Subjects and Methods
This study was conducted at the Department of Endocrinology and Metabolism, All India Institute of Medical Sciences, New Delhi, India. Recently diagnosed, treatment-naive T2DM patients presenting to the Endocrinology Outpatient Department from July 1, 2008 to June 30, 2009 were the subjects for the study.
The study protocol was approved by the institutional ethics committee. Written informed consent was obtained prior to study participation. As this was an exploratory study, sample size was calculated taking into account the number of patients who could be studied during a 1-year period. Based on our previous experience we planned to enroll 20 patients for this study.
Inclusion criteria
Newly diagnosed T2DM patients with two fasting blood glucose (FBG) values >200 mg/dL and no past or present history of treatment with oral hypoglycemic agents or insulin who were more than 18 years of age were included in the study.
Exclusion criteria
Patients with the following diagnoses were excluded: diabetes with acute complications, gestational diabetes mellitus, secondary diabetes mellitus, presence of chronic complications related to diabetes mellitus that could interfere with study design, and intake of drugs known to affect carbohydrate metabolism.
Methodology
The baseline evaluation included detailed history, physical examination, routine investigations, glycosylated hemoglobin (HbA1c), FBG, postprandial blood glucose (PPBG), lipid profile, and serum glutamic acid decarboxylase-65 (GAD-65) antibody. The initial samples of fasting and postprandial plasma insulin and C-peptide were collected on the second or third day after starting treatment with insulin, without missing the insulin dose. This was done to allow for comparison with the plasma insulin and C-peptide values of subsequent months, samples for which were also collected without skipping the insulin dose.
The subjects were given comprehensive diabetes education, which included medical nutrition therapy, lifestyle modification, advice regarding self-monitoring of glucose at home, insulin injection technique, and management of hypoglycemia. Subjects were started on premixed insulin (30/70) at a dose of 10 units half an hour before breakfast and 6 units half an hour before dinner. 13 The subjects were encouraged to monitor capillary glucose before and after meals. If the patient developed hypoglycemia, the dose of insulin was reduced by 2 units. The subjects whose insulin dose was reduced to 4 units or less per day were changed to a single dose of long-acting insulin analog (glargine) at bedtime. The minimum dose (4 units) of insulin was continued for a period of 3 months after achieving near euglycemia.
The patients were followed up in the endocrine outpatient department on a monthly basis for 6 months. Estimation of FBG, PPBG, plasma insulin, and C peptide was done every month during the study period. HbA1c was measured at the end of 3 and 6 months. Body weight and waist circumference were recorded at the time of inclusion and at the end of the third and sixth months. Lipid profile was done at the end of 6 months. One of the study physicians was available around the clock for telephone consultation.
Statistics
Data are presented as number (%) or mean ± SD values as appropriate. Wilcoxon signed rank test was used to compare clinical and laboratory characteristics of the patients before and after initiation of insulin therapy. A P value of ≤0.05 was considered significant.
Results
In total, 20 newly diagnosed treatment-naive T2DM patients were enrolled in the study and were followed up for 6 months. The clinical profile of these 20 patients is shown in Table 1. The mean age of the study population was 41.6 ± 12.5 years (range, 26–65 years). The mean duration of osmotic symptoms before presenting to our clinic was 41.25 ± 62.41 days (range, 5–240 days). The mean body mass index (BMI) of the study group at presentation was 26.02 ± 5.34 kg/m2 (range, 17.62–35.71 kg/m2). Nine (45%) patients were overweight (BMI ≥25 kg/m2), whereas four (20%) were obese (BMI ≥30 kg/m2). Two patients had BMI <18.5 kg/m2. GAD-65 antibody was detectable in five (25%) patients. The mean weight in the GAD-65-positive group was 63.8 ± 6.3 kg, and that in the GAD-65-negative group was 72.1 ± 17.3 kg. The difference, however, was not statistically significant. Table 2 shows the laboratory parameters at initiation of therapy and at the end of 6 months of treatment. All patients had FBG >200 mg/dL (mean ± SD, 271 ± 52 mg/dL; range, 212–411 mg/dL) at baseline. The mean baseline HbA1c of the patient group was 11.3 ± 1.4% (range, 8.6–13.5%); it was 7.05 ± 0.54 % (range, 6.3–8.1%) at the end of 6 months. Five patients received statins during the study period. The total cholesterol, low-density lipoprotein-cholesterol, and triglycerides were lower, whereas high-density lipoprotein-cholesterol was higher, at 6 months compared with baseline in the 15 subjects who were not initiated on statins. The mean weights of the study subjects at baseline and 3 and 6 months were 70 ± 16 kg (range, 44–95 kg), 68 ± 13 kg, and 68 ± 13 kg (P = 0.083), respectively.
Data are mean ± SD values (range).
Data are numbers (percentages).
T2DM, type 2 diabetes mellitus.
P value is for comparison of value at 6 months with that at baseline.
Lipid profile data are for 15 patients not on statins.
BMI, body mass index; FBG, fasting blood glucose; HbA1c, glycosylated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PP, postprandial; PPBG, postprandial blood glucose.
The starting dose of insulin was 16 units daily for all the patients, and the same dose was maintained until near euglycemia was achieved. The insulin dose was down-titrated based on blood glucose values. Figure 1 shows blood glucose, plasma insulin, and C-peptide values during the 6 months of treatment. Blood glucose levels reached the near-euglycemic range by month 3, whereas insulin and C-peptide levels increased until month 4 and continued in the same range during the next 2 months.
(
Six patients were diagnosed as having hypertension; they received an angiotensin converting enzyme inhibitor or an angiotensin receptor blocker, singly or in combination with other antihypertensives, depending on the blood pressure response. None of the normotensive patients became hypertensive during therapy with insulin.
Discussion
Prevalence of T2DM is increasing globally. The rate of rise is more in developing countries like India, compared with industrialized western countries. The disease starts at a younger age, and patients are therefore more prone to develop complications resulting from chronic hyperglycemia, which imposes a considerable physical and financial burden for both the individual and the society. Therefore we need to develop new theraputic agents and/or strategies that can cure and/or control progression of the disease. 14 Therapy that preserves and/or protects β-cell function will be cost-effective in the long term. 15
There is a progressive defect in insulin secretion in patients with T2DM prior to onset of hyperglycemia. 1 –5,16 –18 Endoplasmic reticulum stress is triggered by chronic hyperglycemia and activation of insulin synthetic pathway. 19,20 Even under physiological conditions the β-cells have a high rate of protein synthesis, and any additional demand for insulin secretion can have the potential to induce exhaustion of insulin biosynthesis. 21 Early insulin therapy and rapid normalization of plasma glucose may mitigate the endoplasmic reticulum stress in β-cells. Other benefits of early therapy with insulin in T2DM may be mediated through its anti-inflammatory 22 and anti-apoptotic 23,24 actions. A recent study with intensive insulin treatment reported normalization of glucose-dependent insulinotropic polypeptide responsiveness. 25 Thus, optimal glycemic control in newly diagnosed T2DM patients with insulin may help to preserve and/or regenerate β-cells. However, only a few studies 6 –13 have specifically focused on the probable role of early insulin therapy in preserving β-cell function and mass in T2DM patients. These studies have shown that a short course of intensive insulin therapy by continuous subcutaneous insulin infusion or multiple subcutaneous insulin injection induced remission in patients with newly diagnosed T2DM. 6 –12 Similar results could be observed with low-dose, twice daily subcutaneous insulin administration. 13
The present study assessed insulin and C-peptide levels during low-dose insulin therapy in newly diagnosed T2DM patients. We observed that there was a significant fall in blood glucose levels by 4 weeks, and near normoglycemia could be achieved by the end of 3 months. There was gradual and consistent increase in plasma insulin and C-peptide during the first 4 months, and the same levels were maintained during the subsequent 2 months of this study. There were no episodes of major hypoglycemia or weight gain during these 6 months.
Plasma insulin and C-peptide were measured without skipping insulin. The dose of insulin was either same or lower than the baseline dose. Therefore it was assumed that the rise in plasma insulin values was contributed by an increase in endogenous insulin secretion. This was further corroborated by a corresponding rise in plasma C-peptide levels. The insulin and C-peptide levels of these subjects were higher in comparison with lean healthy (normal glucose tolerance) subjects by the end of 3 months. 26 Unlike in the previous study, 13 insulin was continued, although in a lower dose for 6 months. However, no change was observed in blood glucose, insulin, or C-peptide beyond 4 months. There was significant improvement in the lipid parameters at the end of 6 months without any lipid-lowering therapy.
Insulin therapy is commonly accompanied with weight gain. 27 –31 The magnitude of weight gain ranged from 3.7 kg to 7.5 kg over the initial year of treatment. 28 –31 The gain in weight in an insulin-treated patient is directly proportional to total daily insulin dose. 32 It has also been suggested that the closer an insulin regimen simulates the normal endogenous insulin secretion, the less is the gain in weight with insulin. 33 Fear of hypoglycemia and weight gain are the two major reasons for the psychological resistance to insulin therapy. 34 –36 The present study, which used low-dose insulin in two divided doses in an outpatient setting, could achieve near normoglycemia without exposing patients to hypoglycemia. As in the previous study, 13 there was a trend towards weight loss.
Low-dose insulin therapy and appropriate dose reduction as normoglycemia is achieved could be a simple and effective way to reverse the disease in newly diagnosed T2DM. Failure to reduce the insulin dose as normoglycemia is achieved could cause periods of undiagnosed hypoglycemia, which will have detrimental effects on β-cell recovery.
The limitations of this study are that it had enrolled only subjects with symptomatic hyperglycemia and the duration of follow-up was only 6 months.
Footnotes
Author Disclosure Statement
No competing financial interests exist.