
Abstract
Background:
Proper healing of ulcers and wounds on the feet of diabetes patients is important in order to prevent amputation. If the wound area reduction during the first 4 weeks of the treatment is not 40% or more, reevaluation of the treatment is necessary. The wound area evaluation is not complicated when the patient stays at a hospital, but when he or she goes home the physician does not have a tool allowing monitoring of the wound area.
Methods and Results:
The aim of the present article is to present a new device able to take a wound picture and send it automatically to the database. This device, called the Patient's Module (PM), is also able to download data from the memories of blood pressure and blood glucose meters and send the data to the database. The PM is able to operate within the TeleDiaFoS system (developed earlier in collaboration with the Department and Clinic of Gastroenterology and Metabolic Diseases, Medical University of Warsaw, Warsaw, Poland) aimed at monitoring of treatment of patients with diabetic foot syndrome. The PM was tested on 10 type 2 diabetes patients during a 3-month period.
Conclusions:
The study revealed that the PM can be used as a home telemonitoring device, and the analysis of the data sent from patient's home enables the assessment of wound healing progress, giving the physician the possibility for earlier change of the treatment if the wound area reduction is not satisfactory.
Introduction
When a DFS patient receives standard outpatient clinic care, the time between visits is longer than 4 weeks. The wound state is not monitored during this time. In order to monitor progress of healing when the patient stays at home, a device allowing taking a wound picture and sending it together with other information related to the patient state to the physician is needed. Based on that information the physician would be able to determine the progress of wound healing and, in the case of insufficient progress, to prepare for change of the wound therapy.
One can conclude that a reliable tool for wound area measurement is necessary and that this tool should be common in clinical practice. It is a simple way to evaluate the wound area when the maximal length of wound is known and the width is perpendicular to the length. The area of an ellipse of chords equal to the length and the width of the wound is a good estimator of the wound area when the wound is not large. The estimation of wound area should not be used when the therapeutic decisions depend on the wound area change. In such a case, to determine the wound area a more reliable method called planimetrics should be used. There are some devices and systems based on this method. A Visitrak from Smith & Nephew (London, UK) 6 needs a transparent foil on which wound boundaries are traced when, in the first step, the foil is placed onto the wound and, in the second step, the traced wound is redrawn onto the digitizing tablet, which calculates automatically the wound area. In other systems the wound area is calculated from digital pictures of the wound. Examples of such systems are PictZar™ (BioVisual Technologies, LLC, Westwood, NJ) 7 and VERG. 8 Some of the systems are portable, such as the Silhouette 9 from Aranz Medical Ltd. (Christchurch, New Zealand) or the Wound Measurement Device from the Georgia Institute of Technology (Atlanta, GA). 10 More advanced systems are able to produce a three-dimensional image of the wound and can measure the wound volume. Examples of such a systems are MAVIS 11 and DigiSkin. 12
None of the above-mentioned systems of wound area measurement can be used by the patient at home as they can be used only by trained operators and are not designed to be operated by the patient.
The main objective of this article is to present a new device designed and developed at the Institute of Biocybernetics and Biomedical Engineering, Polish Academy of Sciences (Warsaw, Poland) for telemonitoring of patients with DFS treated at home. The device is operated by the patient without the assistance of other trained person.
Materials and Methods
The imaging device developed, which is also able to download blood glucose and blood pressure data and send the data to the Central Clinical Server (CCS), is called the Patient's Module (PM). The PM is able to work within the TeleDiaFoS system (developed earlier in collaboration with the Department and Clinic of Gastroenterology and Metabolic Diseases, Medical University of Warsaw, Warsaw) designed for monitoring DFS patients.
PM of the TeleDiaFoS system
The PM was designed with some major assumptions: • the patient's safety in the sphere of elimination of possibility of the wound infection • good quality of the wound picture (with minimal file size and minimal time of scanning) • data transmission (blood glucose and blood pressure) • easy to use
Before the development of the PM, a digital camera, a multimedia GSM phone, and an optical scanner were preselected as imaging devices. The digital camera and telephone were excluded because of the need to develop a customized foot support, a stand for the device, and a light source with a support. The optical scanner requires a PC to work, but it assures good lighting, and there is no problem with the foot support because the foot lies on the scanner glass window. An optical scanner was selected in order to develop an imaging device.
The patient's safety is assured by developing a two-stage procedure of the PM disinfection. Microzid AF Liquid® (Schulke & Mayr, Norderstedt, Germany) and Softasept®N (B. Braun, Melsungen, Germany) are used in the first and the second steps of disinfection, respectively. The efficacy of this procedure was evaluated by microbiological tests in which the PM surface was covered by a solution containing wound bacteria, and then, after the disinfection procedure, samples to test microbiological growth were taken. The test gave negative results in eight samples, what was enough to assume the procedure was a safe one. The upper side of the PM is made of tempered glass in order to reduce the risk of injuries when accidentally broken.
The PM case is made of a composite solid surface material that is non-porous and resistant to bacteria. It is also transparent to electromagnetic waves, which is important when a GSM modem is operating inside a box made of this material.
The wound image quality was verified in function of the image resolution, file size, and jpeg compression coefficient. The optimal result was reached when the image resolution was 200 dpi and the compression coefficient was equal to 70. The file size was 150–250 kB, which was not too big to send it with the slowest (GPRS) internet connection used in the PM. The time of foot scanning is about 15 s. The patient is in the sitting position, having one foot onto the floor while the other is scanned (Fig. 1).

Patient's Module while taking a picture of the foot sole.
The Accu-Chek® Active and Accu-Chek Go glucometers (Roche, Mannheim, Germany) and 3BU1-4PC blood pressure meter (Microlife, Widnau, Switzerland) were used in the TeleDiaFoS system. The PM software is able to communicate with the meters and to download the measurement data and send the data to the CCS. The procedure of data sending uses an ftp connection to send the data files to the server. There is a process running at the server that analyzes the files and saves the data in the database tables. Physicians can access the patients' data using local workstations with local databases. The data in the local workstations are synchronized with the data in the CCS in order to enable the physicians to look into the newest patients' data.
When developing the PM it was assumed that the patient will get no support in the device management, so the PM should be easy to use as much as possible. Therefore it was equipped with a two-button remote control.
The PM consists of an optical scanner, PC motherboard with processor and RAM memory, hard disk drive, RS232-IR converter, AD converter with IO ports, wireless GSM modem, wireless controller board for remote control, and custom-made case. There is a scanner window 110 mm wide and 297 mm tall in the upper surface of the PM. The dimensions of the scanner window assure scanning of one foot at a time.
The PM is an autonomic device in the sphere of connection to the internet, and therefore there are no requirements regarding the internet infrastructure at the patient's home. The PM is connected to the internet by a wireless modem, which needs a valid telecom SIM card. When there are problems with the internet connection due to the GSM network coverage, another GSM network can be used after the SIM card is changed.
When the PM starts, it downloads the configuration parameters (patient's ID, conversion coefficient, and automatic switch-off time) from the CCS. If the connection to the CCS is not available, it uses stored values of those parameters. When the PM is ready to use, the patient selects the desired option of the PM operation: (1) scanning, (2) data downloading, or (3) switching the PM off. After scanning and data downloading the PM software automatically sends the data to the CCS and switches the PM off. There is a data backup folder at the hard drive of the PM, and every file ready to send to the CCS is copied to this folder to assure data recovery in case of data transmission failure.
The procedure of the foot wound picture taking requires the few following steps: 1. Putting the PM onto the floor. 2. Disinfecting of the PM. 3. Switching the PM on. 4. Taking off the wound dressing. 5. Putting a foot onto the scanner window in order to take a foot picture (while the patient is sitting). 6. Cleaning the PM and storing it in a safe place.
After the wound picture is taken, the PM sends it to the CCS. The physicians can evaluate the foot sole skin and the wound—its appearance and area.
Calculation of wound area in the TeleDiaFoS system
The wound area measurement in the TeleDiaFoS system is based on counting of pixels within the area or areas traced by operator. Tracing of a wound may be done precisely when the wound boundaries are well-defined as shown in Figure 2; however, a debridement is necessary in case of dead tissue presence around the wound (Fig. 3). The area of the traced wound is a product of the pixel number and the area of a single pixel. The resolution of the foot pictures is 200 dpi, and therefore every image pixel represents a square with sides of length 0.127 mm. The area of a single pixel is 0.016129 mm2. The software calculates also the relative wound area change from the beginning of treatment. It is assumed by default that the day when the first picture was taken is the beginning of treatment.

Example of a foot wound with well-defined wound boundaries.
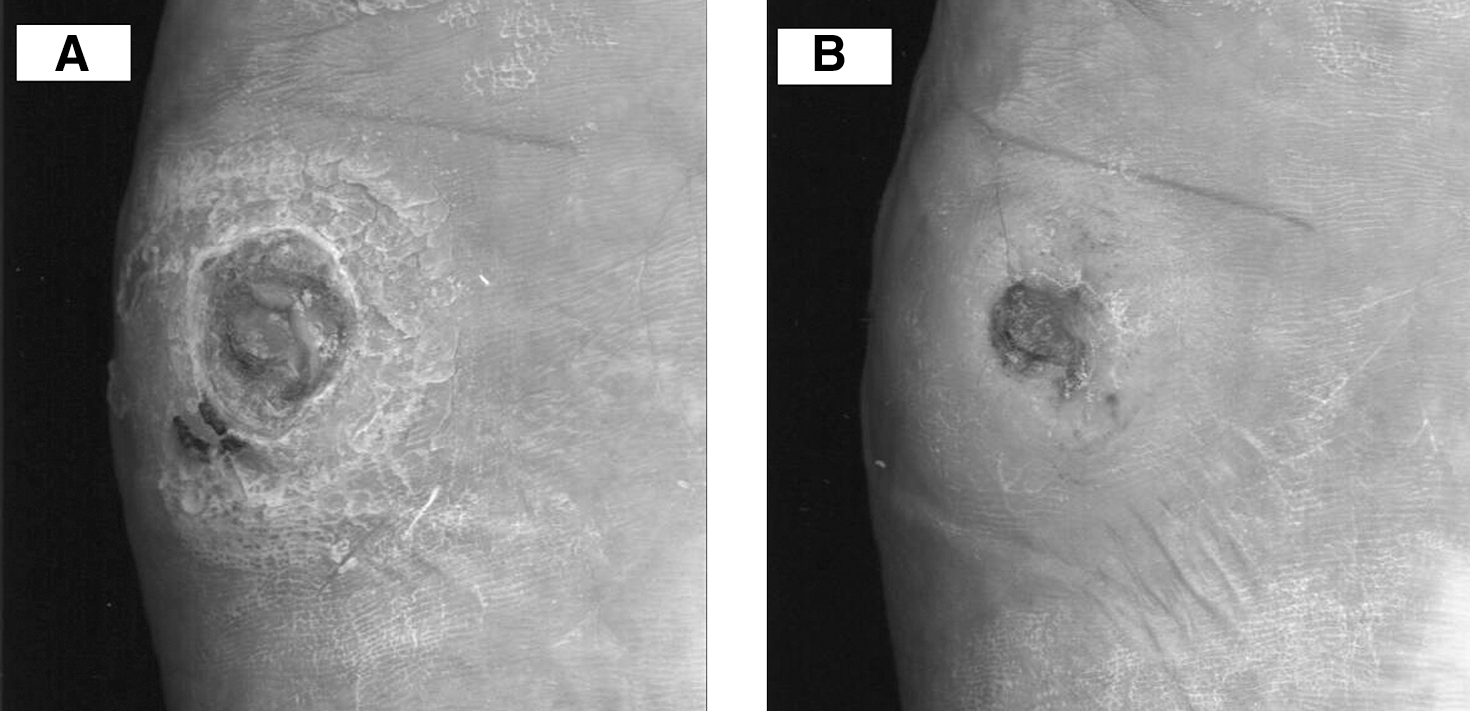
(
The study protocol
The inclusion criteria of patient selection were as follows: diabetes type 2, diagnosis of foot neuropathy, and ulcer present on one foot only. The exclusion criteria were as follows: diabetes type 1, secondary diabetes, retinopathy, nephropathy, heart disease, and mental retardation. The patients were selected in order to verify the technical feasibility of the monitoring system, and therefore we decided to choose those with type 2 diabetes with neuropathy. We wanted to have a homogeneous group. In patients with type 1 diabetes we could have younger persons, but we wanted to show that even older patients have no problem with managing the PM. We assumed that the patient will be the only person for the PM management, so it was necessary to exclude those with retinopathy and as well those with mental retardation. All patients had foot wounds due to neuropathy, but all types of foot wounds are supposed to be monitored using the PM.
The patients were using the PM at their homes, but prior to that they were trained in managing the PM in the clinic or at their homes. They were asked to take a picture of the foot wound not more frequently than wound dressing change. The measurement data (glycemia and blood pressure) were transmitted to the CCS a few times a week. Each foot wound picture was evaluated by four observers in order to calculate wound area and its change from the beginning of healing. Mean value of the foot wound area and coefficient of variation (CV) were calculated for each wound. Median, minimal, and maximal values of CV were calculated for each wound.
The study was approved by the ethics committee of the Warsaw Medical University.
Results
Two hundred fifty-six wound images were sent by 10 patients to the CCS. Table 1 shows the monitoring period, number of assessed wounds, initial wound area, and its change after 4 and 12 weeks or at the end of monitoring for all patients. Median of CVs and their range are also shown in Table 1.
CV, coefficient of variation.
Figure 4 shows the wound area change of the patient with well-defined wound boundaries shown in Figure 2. This patient achieved wound area reduction by more than 50% in 4 weeks of treatment.

Foot wound area of a patient (ID number 3) over a 75-day period of monitoring. Data are mean ± SD values.
Figure 5 shows the wound area change of a patient with not well-defined wound boundaries. As a result there are large CVs of the means. This patient achieved wound area reduction of −23.9% in 4 weeks of treatment.

Foot wound area of a patient (ID number 7) over a 114-day period of monitoring. Data are mean ± SD values.
Discussion
The estimated cost of the PM is $2,500 US on the basis of a few units that have been developed for feasibility assessment. If the production of thousands of units is considered, the cost may be lower than $1,000 US per device. Another cost is the data transmission fee. As we previously have evaluated, 13 the cost of data transmission for 3 months is about $17 US. However, those costs can be eliminated if at the patient's home there is an internet connection that can be used for the PM data transmission. The PM is already equipped with a network card (for cable connection); as well, it can be provided with a Wi-Fi adapter for wireless connection (cost about $5–10 US). Instead of equipping the patient with a PM, we can employ a nurse to do the photographic documentation of the patient's foot every week. Such a nurse should be paid at least $400 US for each patient for 3 months plus costs of travel.
The PM has certain limitations. The picture recorded by a scanner is a projection of the curved skin surface to a flat scanning surface. The smaller the angle between the plane in which the wound is lying and the scanning plane, the larger is the area reproducibility by the scanner. The DFS wounds appear mostly in the regions of the foot sole, where the foot has contact with the ground, and those regions of foot are parallel to the ground. The errors of area reproducibility from those regions are negligible. Our earlier research revealed that more than 98% of foot wounds are located on the foot sole. That part of the foot is in good approximation parallel to the scanning plane, and therefore the area reproducibility is almost 100%. If the angle is equal, for instance, to 10°, scanning gives an underestimation of 1.52% only. In the study 14 comparing wound area values recorded by the Visitrak, Silhouette, linear measurement, and the PM, strong correlations (Pearson correlation coefficient R > 0.985) had been found among the Visitrak, Silhouette, and the PM. In evaluation of the wound healing process, relative area change is more important than its absolute value. When a set of pictures of the wound is taken by the PM over time, the angle between the scanning plane and the wound plane is almost constant (from picture to picture), and as a result the percentage change of the wound area remains, in good approximation, independent of this angle.
Larger deviations in wound area measurements come from uncertainties of positions of the wound edges, which was also pointed out by Flanagan. 15 The same wound is not traced in the same way by different operators—the positions of wound edges differ from one operator to other. This is an important source of error in wound area measurement. The best results in the wound area measurement can be achieved after wound debridement by a trained nurse. When the dead tissue is removed from the wound, the edges of the wound are clearly visible and can be precisely marked (Fig. 3). Otherwise, large uncertainties of positions of the wound edges may be an important issue in the wound area determination. In the case of hyperkeratosis presence around the wound, the patient should be called to visit the ambulatory unit in order to remove the dead tissue.
The PM is prepared to work within the TeleDiaFoS system, but it could be used as a device that sends data to any e-mail user. It can be a physician or other person interested in the wound healing progress.
Every patient was able to operate the PM and was sending successfully the foot images and measurement data. Data transmissions were lost, because of weak GSM signal, in the case of seven images from the total of 386, that is, 1.8%. Those images were retrieved from the backup folder of the PM.
There were 231 files containing the measurement data that were sent to the CCS, and there were no problems concerning transmissions of those files.
A device of similar functionality as the PM, the Vincent 50, has been developed in The Netherlands.
16
It was designed also to send foot pictures from the patient's home to the medical team in order to evaluate the state of the foot. The main differences between the PM and the Vincent 50 are: 1. The PM takes the pictures of 200 dpi resolution, which is two times higher. 2. The PM is able to send the measurement data as BG and BP (the Vincent 50 does not send any measurement data). 3. The PM requires a unique disinfection procedure; we were not informed about the Vincent 50 disinfection procedure, if any.
Our earlier research revealed that patients found the PM easy to use and gave them a sense of safeness because of awareness that the wound state has been evaluated by the medical team. 13 The patients were also glad to be released from travel to the clinic in order to evaluate the foot wound. Travel to the outpatient clinic is accompanied by stress, which was confirmed by some patients. This way the patient's comfort of living is increased.
Prevention of the occurrence of foot ulcers is even more important than monitoring the wound area. There are some reports on foot temperature monitoring in preventing foot ulceration. Lavery et al. 17 concluded that a difference in feet temperature larger than 2.2°C (4°F) is a possible symptom of oncoming ulceration. The temperature measurements are relatively uncomplicated and can be performed by the patient at home. When monitoring of patients who previously did not experience wound ulceration is considered, there is a risk of low patient compliance in such monitoring, because the patients are unaware of the seriousness of the wound development and its consequences. The patient's compliance will be higher in preventing foot ulcer recurrence, and in the case of such patients the foot temperature monitoring would be effective. 18
The cost–benefit analysis of using the PM is related to the decrease in frequency of visits of the patient to an outpatient clinic. When the process of wound healing is accepted by the physician, the patient does not need to arrive for a visit. There are time and money savings for both the patient and the doctor. Another issue concerns the assumption that as time of the wound healing becomes shorter, the physician can react faster to unacceptable progress in the wound healing. Shorter time of the wound healing gives measurable savings. The most important issue is that a healed wound means no need for foot amputation, and that is the most important cost saving. The International Diabetes Federation has stated that the economic cost of a diabetic foot ulcer is thought to be between $7,000 and $10,000 US, and where healing is complicated and amputation required, this cost may increase to as much as $65,000 US per person. 19
A certain limitation of this article is the lack of a randomized controlled trial in which patients with and without PM would be surveyed. Such a study is required to determine the device efficacy in DFS treatment. The strength of this article is the fact that we are presenting in detail a device able to provide home telemonitoring of DFS patients, which is very easy to operate and provides the medical team with useful information regarding foot status and metabolic control of the patient.
The PM revealed its usefulness in home telemonitoring because the wound pictures sent from the patient's home enable the assessment of wound healing progress and therefore give the physician a chance to change the treatment if the percentage wound area reduction is not 10% or more in the first week of treatment or 40% after 4 weeks. The use of the PM may enable reducing the number of foot amputations in DFS patients.
Footnotes
Acknowledgments
The work has been supported by research grant 3 T11E049 29 from the Polish Ministry of Science and Higher Education.
Author Disclosure Statement
No competing financial interests exist.