
Abstract
Background:
The purpose of this study was to examine future acceptance of an artificial pancreas (AP) and its perceived usefulness, ease of use, and trust in the device.
Methods:
A questionnaire, based on the Technology Acceptance Model, was developed to examine future acceptance with its determinants and intention to use the AP. One hundred thirty-two patients with diabetes type 1 treated with insulin pump therapy completed the questionnaire. Using factor analysis and reliability analysis, the number of items was reduced from 34 to 15.
Results:
The response rate was 66%. The subjects had a mean age of 43 years, and 34% were male. Almost 75% had the intention to use an AP. There were high scores on perceived usefulness (expected improvement of glucose control: 35.6% moderately agreed and 53% strongly agreed), perceived ease of use (expectation that the AP can be easily handled: 33.3% moderately agreed and 53.8% strongly agreed), and trust (administration of correct insulin dose and reliability of glucose measurement: 40.9% and 38.9% moderately agreed, whereas 32.6% and 28.2% strongly agreed, respectively).
Conclusions:
A newly developed questionnaire examining the acceptance of an AP indicated that most patients with continuous subcutaneous insulin infusion–treated type 1 diabetes have the intention to use an AP system and have a positive attitude toward perceived usefulness, ease of use, and trust.
Introduction
Looking at the attitudes toward the likely components of the AP, continuous subcutaneous insulin infusion (CSII) and subcutaneous continuous glucose monitoring (CGM), concerns about the acceptance and future use of the AP could be raised. Recently Seereiner et al. 6 showed that in adolescents who stopped pump use, reluctance to CSII was due to catheter insertion-related issues, altered body shape, and decrease in well-being. CSII in adults was associated with concerns about perceived body image and social acceptance. 7 Furthermore, CGM use diminishes over time: 8 over a period of 6 months the frequency of use in the Juvenile Diabetes Research Foundation trial diminished from 7 days/week to 6.5 days/week in adults, from 6.3 days/week to 3.3 days/week in adolescents, and from 6.8 days/week to 3.7 days/week in children. In children, reasons for not wearing CGM included skin irritations, inaccurate readings, and excessive alarms. 9
Parental attitudes towards a closed-loop system were examined by Elleri et al.: 10 all parents with a child with type 1 diabetes welcomed the AP, and 90% of the parents trusted the automatic insulin delivery. In an earlier study, we used interviews to assess the overall attitude toward the AP in 22 adults with type 1 diabetes: 11 overall, there was a positive attitude, with the intention to use the closed-loop system dependent on trust in the AP, which was related to the quality of glucose control that would be provided. These interviews formed the starting point for developing a questionnaire to examine the perceived acceptance and intention to use the AP in a larger patient group. The aim of this study was to develop a questionnaire to examine future acceptance of an AP and its determinants in adults with CSII-treated type 1 diabetes.
Subjects and Methods
Patients
All patients had type 1 diabetes and were treated with CSII. They were followed in the outpatient clinic of a university hospital, the Academic Medical Center in Amsterdam, The Netherlands, or in an affiliated teaching hospital, the Onze Lieve Vrouwe Gasthuis in Amsterdam.
Design
Theoretical framework and questionnaire development
The concept of the questionnaire was based on the Technology Acceptance Model (TAM). The original model studied acceptance or intention to use new computer systems in order to improve job performance. 12 Initially, the TAM was based on two concepts: perceived usefulness and perceived ease of use. Perceived usefulness was defined as the degree to which a person believes that using the new system would enhance job performance. Perceived ease of use was defined as to what degree a person believes that using a particular system would be free of effort. To increase the predictive value of the TAM, both variables were extended with determinants of perceived usefulness and perceived ease of use. 13 –15 Eventually, trust in the new system was added to the model by Pavlou. 16
Figure 1 gives a visual representation of the model.
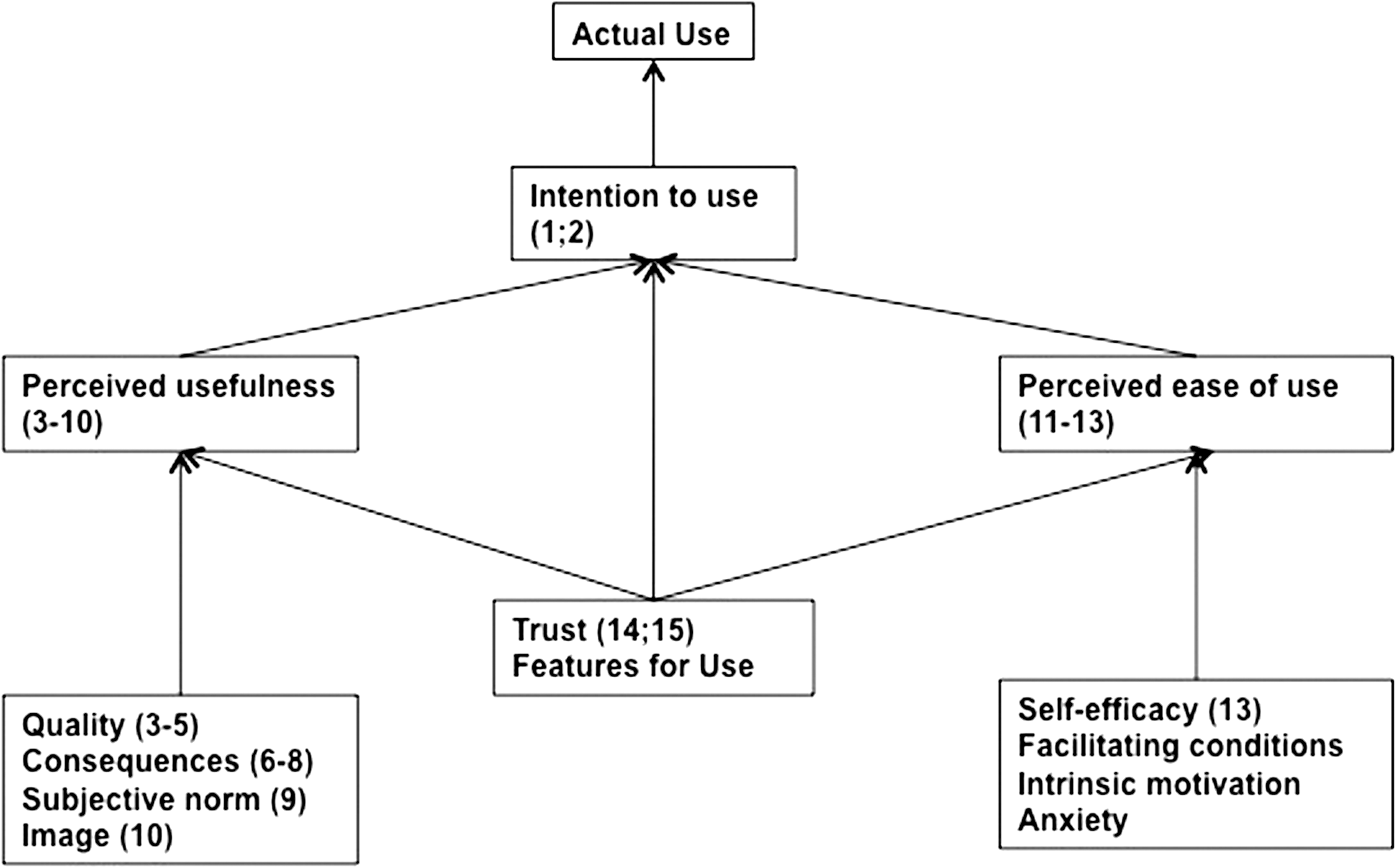
Visual representation of the adapted Technology Acceptance Model. Items (question numbers) of the questionnaire relating to each concept (intention to use, perceived usefulness, perceived ease of use, and trust) are added.
In the context of the AP, the intention to use the AP is the subjective probability that one will use the AP. Perceived usefulness is the degree to which the patient thinks that the AP would facilitate glucose control. Its determinants are quality of care (the degree of glucose control), consequences of the AP (healthcare cost and required time investment, quality of life), the importance of the AP towards glucose control, influence of relatives (subjective norm), and perceived image in a peer group if using the AP.
Perceived ease of use is the degree to which the patient believes that using the AP would be free of effort. The determinants are self-efficacy to operate with the AP, need for training (external control), using features of the currently used insulin pump (proxy for intrinsic motivation), and anxiety at the time of starting the new treatment. As a proxy for the latter, we inquired about anxiety at the time of starting insulin pump treatment. Trust in the AP manufacturer and features of the AP system are additional factors.
Development of the questionnaire
Step 1: in-depth interviews. First, in-depth interviews were performed to evaluate these concepts. The results of these interviews have been reported elsewhere. 11 During the interviews, none of the open questions was experienced as ambiguous. Therefore, the open questions were rephrased to closed questions, and some questions derived from information obtained from those interviews was added, like the widespread patient wish of having a display on the CGM device to increase trust. Initially, 34 items were drafted, as well as some questions on demographic characteristics. Answers were given on a 7-point Likert scale, where 0 = strongly disagree, 1 = moderately disagree, 2 = somewhat disagree, 3 = neutral, 4 = somewhat agree, 5 = moderately agree, and 6 = strongly agree.
Step 2: the introduction. In the written introduction to the questionnaire, the AP was described in detail to the participant. The AP was presented as controlling glucose concentrations in an automated way. Insulin administration would be by CSII, dependent on glucose values measured by a subcutaneous continuous glucose sensor (CGM device). An algorithm would calculate the exact amount of insulin required. This algorithm would be integrated in the insulin pump, without materially increasing its size. The CGM device would need to be replaced every 3–7 days. CGM would perhaps be inaccurate in the range of low and high glucose levels, so in case of an alarm the patient would have to perform self-monitoring of blood glucose (SMBG). Apart from checking the alarms, patients also would have to perform SMBG for calibration at a frequency of twice a day.
Step 3: evaluation by pilot patients (“three-step-interview”). In order to prevent unclearly formulated questions, the questionnaire was presented to 10 pilot patients. Each of them was asked to read out loud the introduction and the questions, and they were asked to give their thoughts on them. After all questions were filled in, 10 questions were picked at random to verify the correct interpretation of the answer to that question. In the end, patients were asked if they thought items were missing. After four pilot patients, we concluded the item of wearing a CGM device as a second device in addition to the pump was not clearly formulated and was rephrased. Furthermore, the introduction of the algorithm was shortened. No items were missing according to the pilot patients.
Step 4: administration of the questionnaire. The questionnaire was sent to all patients with type 1 diabetes using CSII under treatment in the two centers. Two hundred questionnaires were sent out: 80 questionnaires from the affiliated teaching hospital and 120 questionnaires from the university hospital. The patients were asked to answer all questions and were requested to return the questionnaire in a prestamped and preaddressed envelope.
Step 5: translation into English. The Dutch version of the questionnaire was translated backwards in English by two independent translators: one native Dutch speaker with a high level of fluency in English and a native English speaker (Table 1).
AP, artificial pancreas; CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; HbA1c, hemoglobin A1c; SMBG, self-monitoring of blood glucose; TAM, Technology Assessment Model.
Statistical analysis of reliability of the items and item reduction
To reduce the number of items, factor analysis was performed using SPSS version 18.0 (SPSS, Inc., Chicago, IL). The 34 items were subjected to principal components analysis, where the original items are transformed into a smaller set of linear combinations, with all of the variance in the scores being used. To assess data suitability for analysis, the strength of the intercorrelations among the items, individual Kaiser–Meyer Oklin (KMO) value per item, and Bartlett's test of sphericity were used. The strength of the item intercorrelations was reflected in a correlation coefficient of ≥0.3. The threshold for KMO values was set at 0.7. Values above this cutoff value are coherent with good patterns of correlations, and the analysis should yield reliable factors. 17 Bartlett's test of sphericity had to be statistically significant (P < 0.05) for the factor analysis to be considered appropriate. The individual KMO value was below 0.7 in 16 items. Therefore these items were removed and excluded from further analysis.
A principal component analysis of the remaining 18 items was performed to determine the smallest number of factors that can be used to best represent the interrelations among the set of items. Inspection of the matrix revealed most coefficients were above the recommended value of 0.3. The overall KMO value was 0.878, exceeding the recommended value of 0.7, and all individual KMO values were >0.767, which is above the acceptable limit of 0.7. Bartlett's test of sphericity reached statistical significance, indicating the appropriateness of the analysis. To retain the numbers of items, the eigenvalue was set at 1. An eigenvalue of 1 indicates that a substantial amount of the statistical variation is explained by a factor. Also, Catell's scree test was used. This test entails plotting the eigenvalues of the items and inspecting the plot to find a point of inflexion. At such a point of inflexion, that number of items contributes the most to the explanation of the variance in the data set. The principal components analysis revealed the presence of four components with eigenvalues exceeding 1, explaining 39.8%, 9.2%, 7.7%, and 6.3% of the variance. An inspection of the scree plot revealed a clear point of inflexion (change in slope of the line) after the second component. Using direct Oblimin rotation, no separate scales could be found (data not shown).
Reliability analysis was performed using Cronbach's α. The questionnaire had a Cronbach's α of 0.899, reflecting a good internal consistency. Deletion of three of the remaining 18 items increased Cronbach's α to 0.906, and deletion of any of the remaining items would not further increase the α value. In conclusion, the original 34 items of the questionnaire could be reduced to 15 items (Table 1).
Demographic features are given as mean with range of minimum and maximum. Comparisons between gender and the responses from patients under treatment at the university hospital and the teaching hospital were made using the χ 2 test.
Percentages are given if the number of respondents was 132; otherwise, both percentage and absolute number of responses/respondents are given.
Results
One hundred thirty-three patients returned the questionnaire: 86 of 120 patients (71.7%) in the university hospital and 47 of 80 patients (58.8%) in the affiliated teaching hospital. The overall response rate was 66%. One person did not fill out the questionnaire, so 132 questionnaires could be analyzed. The patient characteristics are given in Table 2, and the results of the questionnaire are given in Table 3.
Data are given as mean with range of minimum and maximum (n = 127).
CSII, continuous subcutaneous insulin infusion; SMBG, self-monitoring of blood glucose.
The answers were given on a 7-point Likert scale, where 0 = strongly disagree, 1 = moderately disagree, 2 = somewhat disagree, 3 = neutral, 4 = somewhat agree, 5 = moderately agree, and 6 = strongly agree.
AP, artificial pancreas; CGM, continuous glucose monitoring; HbA1c, hemoglobin A1c.
Mean age was 43 years (range, 18–70 years), and 34% (45 of 127) were male. Diabetes type 1 was diagnosed at a mean age of 17.9 years (range, 1.5–47 years), and the mean duration of CSII treatment was 7.2 years (range, 0.2–29 years). The mean number of SMBG per day was 4.9 (range, 0–12.5), and nine (7%) patients reported not having any difficulty in controlling their glucose during the day. The other patients experienced difficulties during one or more parts of the day. Regarding education, 59% (75 of 127) had high school education or held a university degree, two persons did not have any education, two persons had finished primary school, and 37.8% (48 of 127) did have some form of secondary education. Regarding occupation, 72.4% (92 of 127) had a paid job, two patients did voluntary work, three were unemployed, two persons were retired, six were students, 8.3% (11 of 127) were disabled, and 7.8% (10 of 127) were housewives.
Intention to use
The majority would like to change at this time their current treatment to the AP (10.6% somewhat agreed, 19.7% moderately agreed, and 55.3% strongly agreed), whereas 7.6% were neutral and 6% responded negatively.
Perceived usefulness
Most patients believed that the AP will improve their glucose control (35.6% moderately agreed, and 53% strongly agreed). Most subjects anticipated that the AP will reduce the frequency of hypoglycemia: 37.9% moderately agreed, and 42.4% strongly agreed. Similarly, a reduction in hyperglycemia was expected by 83.4%: 37.9% moderately agreed, and 45.5% strongly agreed.
Determinants of perceived usefulness
The responses to the statements that by using the AP life will be easier and that wearing the AP will decrease the worries about diabetes were almost similar: 7.6% of the patients strongly disagreed, 15.9% and 12.2% (16 of 131) of the subjects were neutral, 20.5% and 19.0% (25 of 131) somewhat agreed, 20.5% and 25.2% (33 of 131) moderately agreed, and 28.0% and 35.9% (47 of 131) strongly agreed. Furthermore, 11.4% disagreed on the item that AP will reduce the daily time spent on diabetes, 22% were neutral, and 66.7% agreed (15.2% somewhat, 27.3% moderately, and 24.2% strongly). Most of the subjects felt influenced by the opinion on AP of people who are important to them (12.1% somewhat agreed, 21.2% moderately agreed, and 33.3% strongly agreed). Twelve percent of the subjects disagreed that others would influence them to wear the AP. Almost the same distribution was found on the item “Wearing an AP will make me an example to other people with diabetes.”
Perceived ease of use
Most (75.8%) of the subjects agreed on the item “the AP seems easy to use” (25.1% [33 of 131] somewhat agreed, 24.4% [32 of 131] moderately agreed, and 26.7% [35 of 131] strongly agreed), 19.1% (25 of 131) subjects were neutral, and the remaining 4.5% (six of 131) disagreed on this item. The statement that wearing a CGM device in addition to the insulin pump will not hinder using the AP resulted in the following breakdown of answers: 1.5% (two of 131) strongly disagreed, 3.8% (five of 131) moderately disagreed, 2.3% (three of 131) somewhat disagreed, 6.8% (nine of 131) were neutral, 15.9% (21 of 131) somewhat agreed, 26.7% (35 of 131) moderately agreed, and 42.7% (56 of 131) strongly agreed.
Determinants of perceived ease of use
Almost all subjects (94.7%) thought that they could handle the AP (7.6% somewhat agreed, 33.3% moderately agreed, and 53.8% strongly agreed), whereas 4.5% of the subjects were neutral and 0.8% strongly disagreed.
Trust
The responses to the items that the AP will administer the right amount of insulin and that AP would measure correctly the glucose concentrations were almost similar: 1.5% of the subjects strongly disagreed on both items, 0.8% disagreed moderately on both items, 0.8% and three of 131 (2.3%) subjects somewhat disagreed, 8.3% subjects versus 10 of 131 (7.6%) subjects neutral, 14.4% and 27 of 131 (20.6%) somewhat agreed, 40.9% and 51 of 131 (38.9%) moderately agreed, and 32.6% and 37 of 131 (28.2%) strongly agreed.
No differences were seen between males and females and between university hospital–and affiliated teaching hospital–treated patients (data not shown).
Discussion
We developed and validated a questionnaire that examined the acceptance of an AP. The outcome was that most patients with type 1 diabetes had the intention to use this system, and they had a positive attitude toward perceived usefulness, perceived ease of use, and trust, suggesting a high need for closed-loop systems among type 1 diabetes patients.
The initial questionnaire was developed on the basis of the in-depth interviews based on the TAM. 11 It contained 34 items, and after the factor analysis and reliability analysis, were performed, more than half of the items could be excluded. The remaining 15 items reflected the concept of the TAM: two questions for intention to use, eight questions for perceived usefulness and its determinants, and three items for perceived ease of use. Only for features for use were no questions retained. Also, three determinants of perceived ease of use did not have an item in the questionnaire, probably because of removal of the last two items from CSII use and the reluctance experienced before the starting the insulin pump.
A limitation of the study was that the AP was described and was not visualized by a prototype. Therefore patients could have had an insufficient concept of the AP and could therefore be biased toward the positive or negative regarding the AP. Also, in The Netherlands, a limited number of patients are familiar with CGM because of the lack of reimbursement. This could make the subjects less critical on the performance of the AP despite the explicit remark of inaccuracy of CGM in the introduction. The estimated experience with mostly short-term CGM in the total population (n = 200) was around one-third. Furthermore, the questionnaire was only presented to subjects with type 1 diabetes who were treated with CSII. This population could be positively biased because they are used to wear a device with corresponding technical limitations like occlusions and alarms and have accepted any negative influence on body perception. However, these patients are the most likely first candidates for AP systems.
This AP acceptance questionnaire can be used in different populations and for investigating the acceptance of AP systems with different features, such as bihormonal systems requiring a dual pump. 2,3,5 Different features can be described in the introduction, and prototypes of a closed-loop system can be shown before administering the questionnaire.
To conclude, most of the patients with type 1 diabetes were willing to use an AP system and expected it to be beneficial. This supports more research and funding for the development of closed-loop systems.
Footnotes
Acknowledgments
This study was funded by the Netherlands Organization of Scientific Research.
Author Disclosure Statement
There are no conflicts of interest.