
Abstract
Background:
EZSCAN® (Impeto Medical, Paris, France), a noninvasive device that assesses sweat gland dysfunction using reverse iontophoresis, also detects early dysglycemia. Given the interrelationships among dysglycemia, vasculopathy, and neuropathy, EZSCAN may detect kidney disease in diabetes (DKD).
Methods:
An EZSCAN score (0–100) was calculated using a proprietary algorithm based on the chronoamperometry analysis. We measured the score in 50 Chinese type 2 diabetes patients without DKD (urinary albumin–creatinine ratio [ACR] <2.5 mg/mmol in men or ACR <3.5 mg/mmol in women and estimated glomerular filtration rate [eGFR] >90 mL/min/1.73 m2) and 50 with DKD (ACR ≥25 mg/mmol and eGFR <60 mL/min/1.73 m2). We used spline analysis to determine the threshold value of the score in detecting DKD and its sensitivity and specificity.
Results:
EZSCAN scores were highly correlated with log values of eGFR (r=0.67, P<0.0001) and ACR (r=−0.66, P<0.0001). Using a cutoff value of 55, the score had 94% sensitivity, 78% specificity, and a likelihood ratio of 4.2 to detect DKD with a positive predictive value of 81% and a negative predictive value of 93%. On multivariable analysis, DKD was independently associated with EZSCAN score (β=−0.72, P=0.02), smoking status (1=never, 0=current/former) (β=−2.37, P=0.02), retinopathy (1=yes, 0=no) (β=3.019, P=0.01), triglycerides (β=2.56, P=0.013), and blood hemoglobin (β=−0.613, P=0.04). Patients without DKD but low EZSCAN score (n=10) had longer duration of disease (median [interquartile range], 13 [9–17] vs. 8 [4–16] years; P=0.017) and were more likely to have retinopathy (36.7% vs. 5.1%, P=0.02), lower eGFR (98 [95.00–103] vs. 106 [98.5–115], P=0.036), and treatment with renin–angiotensin system blockers (81.8% vs. 25.6%, P=0.002) than those with a normal score.
Conclusion:
EZSCAN may detect high-risk subjects for DKD in Chinese populations.
Introduction
EZSCAN® (Impeto Medical, Paris, France) is a new, patented technology that measures electrochemical skin conductance through reverse iontophoresis and chronoamperometry. In brief, iontophoresis is the physical process that enables electrically charged particles to pass through a membrane after an electrical stimulus. Reverse iontophoresis extracts ions from the sweat glands with sympathetic innervation. Measurements are performed where sweat glands are most numerous on the palms of the hands, soles of the feet, and forehead. Large-area nickel electrodes are used alternatively as an anode or a cathode. A low-voltage direct current (DC) is applied on the anode to generate a voltage through reverse iontophoresis on the cathode. A current between the anode and cathode with intensity of about 0.2 mA, proportional to the sweat chloride concentration, is then measured by chronoamperometry. 8,9
EZSCAN is a noninvasive and rapid test that does not require special subject preparation or medical supervision. This technology was first validated in patients with cystic fibrosis who had high sweat chloride concentration and subsequently confirmed to have 75% sensitivity and 100% specificity in measuring sudomotor dysfunction in type 2 diabetes patients. 8 This technology can also detect diabetes with 70–84% sensitivity and specificity, probably because of reduced distribution of sweat glands and subepidermal nerve fibers. 9 Given the close associations among dysglycemia, neuropathy, and vasculopathy, 10 we hypothesize that this technology may be used to detect high-risk subjects for DKD for intensive treatment.
Patients and Methods
As part of a quality improvement program, we enroll 30–40 patients with diabetes weekly into the Hong Kong Diabetes Registry, established since 1995. All patients underwent a 4-h clinical assessment on an outpatient basis, after at least 8 h of an overnight fast. Standard procedures, modified from the European DiabCare protocol, were used to document medical history, anthropometric indices, BP, retinopathy (retinal photography), sensory neuropathy (graduated tuning fork and monofilament), and peripheral vascular disease (Doppler scan) (Table 1). A blood sample was collected for hematology and biochemical tests. A sterile, random spot urine sample was collected to measure ACR. 11
Data are mean±SD or median (interquartile range) values or number of patients (%).
Kidney disease in diabetes (DKD) was defined as a urinary albumin-creatinine ratio (ACR) of ≥25 mg/mmol and an estimated glomerular filtrate rate (eGFR) of <60 mL/min/1.73 m2 on two occasions within 4–6 weeks.
Non-DKD defined as a random spot ACR of <2.5 mg/mmol in men or of <3.5 mg/mmol in women and an eGFR of >90 mL/min/1.73 m2 on two occasions within 4–6 weeks.
Complications were defined as follows: retinopathy, diabetes-related changes (hemorrhage and exudates on fundus photograph or history of advanced eye disease such as retinal detachment or vitreous hemorrhage); peripheral neuropathy, two of three signs and/or symptoms of abnormal sensation in distal extremities and reduced sensation on graduated tuning fork (<4/8 for age ≥60 years and <6/8 for age <60 years) at the ankle or monofilament to the sole and forefoot; stroke, transient or permanent neurological damage due to cerebrovascular accident; coronary heart disease, history of myocardial infarction, acute coronary syndrome, chest pain with positive coronary imaging or stress test, or history of coronary artery intervention; and peripheral vascular disease, history of lower extremity amputation or absent foot pulses confirmed by ankle:brachial ratio of <0.9 on Doppler scan.
ACEI, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BP, blood pressure; HbA1c, glycosylated hemoglobin; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; OAD, oral antidiabetes drugs.
Inclusion and exclusion criteria
The Chinese-calibrated abbreviated Modification of Diet in Renal Disease Study was used to calculate the eGFR, expressed in mL/min/1.73 m2:
where SCR is serum creatinine expressed in μmol/L and 1.233 is the adjusting coefficient. 12
In this study, DKD was defined as ACR ≥25 mg/mmol and eGFR <60 mL/min/1.72 m2 on two separate occasions within 4–6 weeks. Patients with eGFR <15 mL/min/1.732 or on dialysis were excluded. Patients with normoalbuminuria (ACR <3.5 mg/mmol in women and <2.5 mg/mmol in men) and eGFR >60 mL/min/1.72 m2 on two occasions were used as control subjects. Patients with two consistent sets of values fulfilling these criteria were invited to undergo EZSCAN testing in accordance to the manufacturer's instruction. The study was approved by the Chinese University of Hong Kong Clinical Research Ethics Committee. All patients gave written informed consent.
Laboratory assays
Plasma glucose was measured by a hexokinase method (Hitachi 911 automated analyzer, Boehringer Mannheim, Mannheim, Germany). Glycosylated hemoglobin (HbA1c) was measured by an automated ion-exchange chromatographic method (Bio-Rad Laboratories, Hercules, CA) (reference range, 5.1–6.4%). Inter-assay and intra-assay coefficients of variation for HbA1c were both ≤3.1% at values below 6.5%. Total cholesterol, triglycerides, and high-density lipoprotein-cholesterol were measured by enzymatic methods on the Hitachi 911 automated analyzer using reagent kits supplied by Boehringer Mannheim. Low-density lipoprotein-cholesterol was calculated by the equation of Friedewald et al. 13 Urinary creatinine (by the Jaffe kinetic method) and albumin (immunoturbidimetry method) were also measured on the Hitachi 911 automated analyzer using reagent kits supplied Boehringer Mannheim. The inter-assay precision coefficients of variation were 12.0% and 2.3% for urinary albumin concentrations of 8.0 mg/L and 68.8 mg/L, respectively. The lowest detection limit was 3.0 mg/L. Serum creatinine was measured (by the Jaffe kinetic method) on a Dimension AR system (Dade Behring, Deerfield, IL). The precision performance of all assays was within the manufacturer's specifications.
Measurement of EZSCAN scores
The EZSCAN device was designed to perform a precise evaluation of sweat gland function based on sweat chloride concentrations using reverse iontophoresis and chronoamperometry. Six electrodes were placed on skin areas rich in sweat glands—namely, the forehead, palmar side of the hands, and plantar side of the feet. A continuous current lower than 4 V among these six electrodes was induced, and the conductance (in mSi), expressed as a ratio of the current generated and the constant DC stimulus, was calculated for the face (left and right part), hands (left and right), feet (left and right), and whole body (global conductance). A time/ampere curve was recorded for each derivation, and the mean value was estimated for each region. The conductance is characteristic of different parts of the body depending on the topographical distributions of sympathetic ganglions and nerve fiber lengths. A specific zone generates the same electrochemical measures in a subject, except when a pathological process modifies the function due to small fiber neuropathy. 8
During the test, the patient placed his or her hands and feet on the electrodes and headband electrodes on the forehead. All electrodes were connected to a computer for recording and data management (Fig. 1). The patient was asked to stand still for 2 min. During the test, six combinations of 15 different low DC voltages were applied. According to the conductance measured on hands and feet, an EZSCAN score ranging from 0 to 100 was calculated using a proprietary algorithm. All patients' details were de-identified, and the corresponding EZSCAN results were displayed on the screen, which could not altered by users or readers.

EZSCAN apparatus and connection to a computer for recording and data management.
Statistical analyses
Statistical Analysis System release 9.10 (SAS Institute Inc., Cary, NC) and Statistics Package for the Social Sciences version 10.0.7 for Windows (2000, SPSS, Inc., Chicago, IL) were used to perform analysis unless otherwise specified. All data are expressed as mean (SD) or median (interquartile range) as appropriate. Comparison between groups was made by Student's t test or Mann–Whitney test as appropriate. Urinary ACR and eGFR were logarithmically transformed for correlation analysis with EZSCAN scores. Two statisticians not involved in the conduct of the clinical study, independent of the sponsor, performed the analysis. Restricted cubic spline with three knots was used within logistic regression analysis 14,15 to generate the odds ratio curve that showed the full-range association between EZSCAN and DKD. We examined the shape of the curve and selected the threshold value where the odds ratio for DKD started to rise sharply. We used this cutoff point to regroup the EZSCAN score into a binary variable and used C-statistics to determine the model fit and its ability to detect DKD, as indicated by sensitivity, specificity, positive predictive value, negative predictive value, and likelihood ratios. A value of P<0.05 was considered significant.
Results
Between January and October 2009, 163 patients fulfilling the ACR and eGFR values were invited to undergo repeat blood and urine testing within 4–6 weeks followed by EZSCAN testing. Among the 123 subjects who returned for repeat testing, 50 were selected as cases and 50 as controls with two sets of consistent ACR/eGFR results. Patients with DKD had longer duration of disease, higher triglycerides and ACR, and lower EZSCAN score, eGFR, and blood hemoglobin than those without. They were also more likely to be smokers and had stroke, retinopathy, and treatment with insulin, statins, and/or RAS blockers (Table 1).
There were high correlations between EZSCAN score and log values of eGFR (r=0.67, P<0.0001) and ACR (r=−0.66, P<0.0001). Figure 2 shows the spline curve analysis and identified two cutoff values of EZSCAN score with C-statistics of 0.86 for the cutoff point of 55 and 0.81 for the cutoff point of 59. These values had over 90% sensitivity and 66–78% specificity to detect DKD with a likelihood ratio of 2–4. They also had over 90% sensitivity to detect retinopathy and sensory neuropathy (Table 2). We used significantly different variables on univariable analysis (age, sex, duration of disease, triglycerides, blood hemoglobin, systolic BP, smoking, alcohol intake, retinopathy, and neuropathy) as independent variables in the multivariate analysis. The category of DKD (1=yes, 0=no) was independently associated with EZSCAN score (β=−0.72, P=0.02), smoking (1=never smoker, 0=current/former smoker) (β=−2.37, P=0.02), retinopathy (β=3.019, P=0.01), triglycerides (β=2.56, P=0.013), and blood hemoglobin (β=−0.613, P=0.04). In a separate model adjusting for drug usage (insulin, oral antidiabetes drugs, statins, RAS blockers, other BP-lowering drugs), age, sex, and duration of disease, EZSCAN (β=−0.65, P=0.028) remained independently associated with DKD along with BP-lowering drugs (β=2.94, P=0.008).

A restricted cubic spline Cox model analysis (univariable) showing the odds ratios of EZSCAN score for kidney disease in diabetes in Chinese type 2 diabetes patients with a threshold value of 55–59 in a declining manner.
DKD, kidney disease in diabetes.
Figure 3 shows the scatter plot between eGFR and EZSCAN scores with high concordance at low values. Among the 50 subjects without DKD (eGFR >60 mL/min/1.73 m2), 10 had EZSCAN score lower than 55. Compared with those with a normal EZSCAN score (n=40), these subjects had lower score (47.55±5.66 vs. 65.82±8.33, P<0.001), longer duration of disease (median [interquartile range], 13 [9–17] vs. 8 [4–16] years; P=0.017) and were more likely to have retinopathy (36.7% vs. 5.1%, P=0.02), lower eGFR (98 [95.00–103] vs. 106 [98.5–115], P=0.036), and treatment with RAS blockers (81.8% vs. 25.6%, P=0.002).
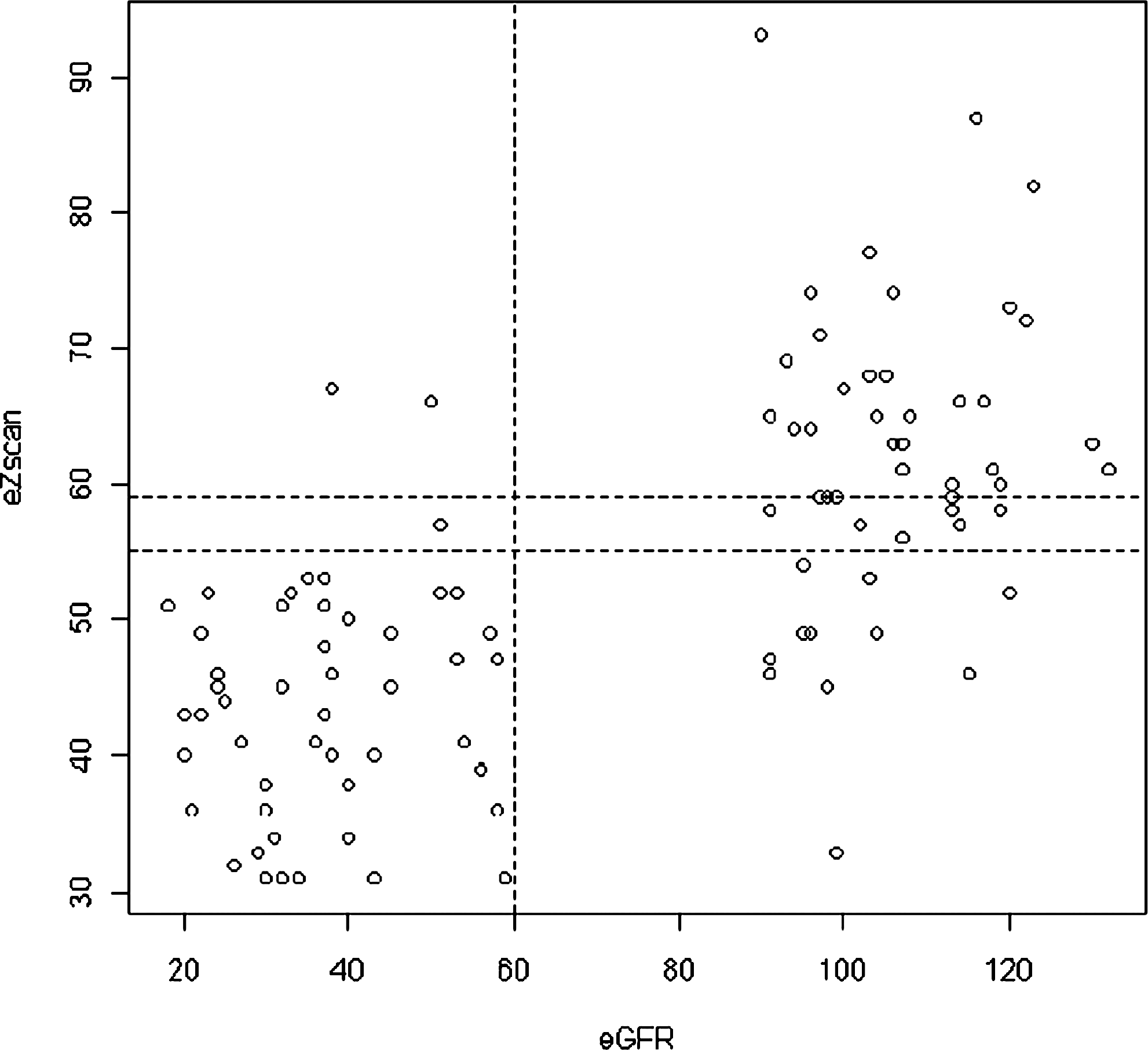
A scatter plot and grid analysis showing the correlations between estimated glomerular filtration rate (eGFR) and EZSCAN scores.
Discussion
In this proof-of-concept study, we used two validated parameters (ACR/eGFR) to select patients with or without DKD based on consistent results on two occasions. Compared with those without DKD, patients with DKD were older, had longer duration of disease, were more likely to be treated with multiple drugs, and had more risk factors and complications including low blood hemoglobin. The latter is a powerful predictor for all-cause mortality and cardiorenal complications in Chinese type 2 diabetes patients. 16 From the 5-year prospective Hong Kong Diabetes Registry involving more than 5,000 type 2 diabetes patients, we have reported the independent predictive roles of male, disease duration, age, HbA1c, retinopathy, micro-/macroalbuminuria, metabolic syndrome components, and low body mass index for new onset of DKD. 17 For end-stage renal disease, only blood hemoglobin and ACR were independent predictors. 18 Thus, results from this case-control study agree with findings from our prospective surveys.
Using spline curve analysis, we selected an EZSCAN score of 55 to detect DKD with a C-statistic of 0.86, with the latter being comparable to the area under the curve of the receiver operator curve analysis. This cutoff point had 94% sensitivity, 78% specificity, and a likelihood ratio of 4.2 in detecting DKD. It is interesting that subjects without DKD but abnormal EZSCAN score had lower eGFR and longer duration of disease and were more likely to have retinopathy and have been treated with RAS blockers than those with a normal score, suggesting that the EZSCAN score may be used as a noninvasive test to detect subjects with DKD.
EZSCAN as a validated tool to detect neuropathy
The independent association of DKD with EZSCAN score might be in part due to its frequent association with neuropathy. 19 Several observational studies have reported the presence of early somatic and autonomic neuropathy in subjects with prediabetes and metabolic syndrome. 20 In a community-based survey of 100 subjects with diabetes or prediabetes, 20% and 54%, respectively, had probable somatic (nerve conduction study) and autonomic neuropathies (heart rate variability study). Some of the implicated risk factors included hyperglycemia, renal insufficiency, and systolic blood pressure. 20,21
Eccrine glands, which mediate sweat responses, are simple tubular glands with a rich supply of blood vessels and sympathetic C nerve fibers, which are mainly cholinergic. The distribution of eccrine glands covers a density of 500–600/cm2 over the palms of the hands and soles of the feet, 180/cm2 on the forehead, 108/cm2 on the forearm, and 60/cm2 on the back. In physiological conditions, the secretory coil produces an ultrafiltrate (isotonic to plasma), with reabsorption of sodium and chloride by the sweat duct resulting in hypotonic sweat with stable ionic concentration. In people with autonomic dysfunction, an abnormal sweat response may be an early marker of small fiber neuropathy. 22 Recent advances using skin biopsy also identified abnormal structure and function of sweat glands in subjects with diabetes. 23
Potential clinical utility of EZSCAN to detect DKD
Our study was based on the premise that patients with DKD were likely to have widespread vascular and nerve dysfunction, which can be due to factors not routinely measured in clinical practice (e.g., inflammatory, metabolic, and genetic factors) in addition to disease duration, BP, and HbA1c. In our study, we used conventional methods to detect somatic neuropathy (e.g., tuning fork and monofilament) but did not document autonomic neuropathy. Because the technology of EZSCAN is highly sensitive and specific in detecting sweat gland dysfunction, 8 it is plausible that it has provided some measures of autonomic neuropathy that either coexist or precede DKD. A prospective study involving more subjects with measurements of autonomic neuropathy is needed to confirm this hypothesis.
Most professional bodies recommend regular screening for complications and risk factors in patients with diabetes, including eye, feet, blood, and urine examinations. 24 However, in part because of the complex nature of the protocol, the silent nature of these risk factors, and large clinic volume, many audits have revealed suboptimal assessment procedures in diabetes patients, resulting in delayed diagnosis and treatment. In the International Diabetes Mellitus Practice Survey, which enrolled over 9,000 type 2 diabetes patients outside North America and Europe, nearly 30% of patients never underwent screening for microvascular complications, including renal function and/or albuminuria. 7 Similarly, nephrologists have reported late presentation of DKD, often with poor control of risk factors prior to referral. 25
Conclusions
Treatment of diabetes is expensive, and with the onset of diabetes complications, especially end-stage renal disease, the treatment cost is further increased by three- to 10-fold. 26 In the Emerging Risk Factor Collaboration, consisting of 97 prospective cohorts, diabetes subjects have a threefold increased risk of renal disease compared with subjects without diabetes. 27 Despite these disease burdens, optimal control of risk factors and appropriate use of RAS blockers can prevent these organ damage by 20–50%. 3,28,29 These data will need independent replication, but our preliminary results suggest that EZSCAN may be a simple tool that can be administered by non-medical personnel in non-healthcare settings with minimal subject preparation, to raise awareness and detect high-risk subjects for DKD for definitive testing and intensified management.
Footnotes
Acknowledgments
We thank all medical and nursing staff at the Yao Chung Kit Diabetes Assessment Centre and Diabetes Clinical Trial Unit of the Chinese University of Hong Kong, the Prince of Wales Hospital, Shatin for recruiting the patients. The study was supported by an unrestricted educational grant from Impeto Medical, Paris, France.
Author Disclosure Statement
P.B., J.-H.C., and J.-P.D. are employees of Impeto Medical. R.O., K.K.T.C., E.W., A.K., X.Y., E.L., and J.C.N.C. declare no competing financial interests exist.