
Abstract
Self-monitoring of blood glucose (SMBG) in type 2 diabetes has increasingly been shown to display beneficial effects on glycemic control. SMBG is not only associated with a reduction of hemoglobin A1c but has also been demonstrated to increase patients' awareness of the disease. SMBG has also the potential to visualize and predict hypoglycemic episodes. International guidelines by the International Diabetes Federation, the European Society of Cardiology, and the European Association for the Study of Diabetes and also the International Society for Pediatric and Adolescent Diabetes emphasize that SMBG is an integral part of self-management. More recently, two European consensus documents have been published to give recommendations for frequency and timing of SMBG also for various clinical scenarios. Recently, a European expert panel was held to further facilitate and enhance standardized approaches to SMBG. The aim was to present simple, clinically meaningful, and standardized SMBG strategies for type 2 diabetes. The panel recommended a less intensive and an intensive scheme for SMBG across the type 2 diabetes continuum. The length and frequency of SMBG performance depend on the clinical circumstances and the quality of glycemic control. The expert panel also recommended further evaluation of various schemes for SMBG in type 2 diabetes in clinical studies.
Introduction
Studies
There is strong evidence that SMBG is highly beneficial in people treated with and without insulin. A systematic review, which included 15 trials with more than 3,200 patients, analyzed the effect of SMBG on glycemic control in non–insulin-treated patients with type 2 diabetes. 1 SMBG was associated with a significant reduction of hemoglobin A1c (HbA1c), compared with non-SMBG. This effect tended to be greatest in patients with poor glycemic control and did not drop over longer follow-up periods. Furthermore, SMBG was associated with a more frequent detection of hypoglycemia, generally in the mild to moderate range. However, no references on optimal frequency of SMBG testing could be deduced. 1
Another meta-analysis on the effects of SMBG, 2 which included 13 randomized controlled trials, found that interventions with SMBG showed a reduction in HbA1c of 0.40% compared with interventions without SMBG. The meta-analysis also pointed out that when regular medical feedback was provided to people, the HbA1c reduction more than doubled. 2
A meta-analysis of 1,307 non–insulin-treated patients with type 2 diabetes demonstrated a 0.42% lower HbA1c level in those patients who performed SMBG compared with those who did not apply SMBG. 3 A meta-analysis of five randomized, controlled trials of people with type 2 diabetes without insulin reported an overall decrease of 0.39% in HbA1c in favor of SMBG 4 compared with the control group. Benefits of SMBG in the management of patients with type 2 diabetes who are not receiving insulin have also been observed in the Kaiser Permanente Northern California Medical Care Program. 5
The Diabetes Glycemic Education and Monitoring (DiGEM) study failed to demonstrate a positive impact on HbA1c levels in patients with type 2 diabetes. 6 Multiple limitations of the study, however, need to be considered. For example, the mean HbA1c values of patients ranged from 7.41% to 7.53% at enrollment (a value close to the treatment goal in many patients), and therefore there was a low potential to improve blood glucose control in the patients. Furthermore, a clear differentiation of the groups (with and without blood glucose monitoring) was not achieved. 6
The potential of SMBG in patients with newly diagnosed type 2 diabetes was demonstrated in a recent, 1-year study conducted in Spain. 7 An SMBG-based structured educational and pharmacological program (n=99) was compared with an HbA1c-based control group (n=66). In the HbA1c group treatment regimens were changed on the basis of HbA1c values every 3–6 months. The SMBG group started with six-point profiles every 3 days. After glycemic stabilization they performed one profile every 1–2 weeks. 7 The SMBG patients achieved higher rates of diabetes regression (HbA1c <6% on metformin alone) and remission (HbA1c 6.0–6.4%) compared with the control group (39% vs. 5% and 37% vs. 30%, respectively). In addition, within 1 year the median HbA1c (from 6.6% to 6.1%) and body mass index (from 29.6 to 27.9 kg/m2) were significantly reduced in the SMBG group, but not in the control group. 7
In another recent study, conducted in Japan in 71 patients with type 2 diabetes, SMBG at low frequencies also resulted in an improved glycemic control. 8 The participants, who were all treated without insulin, were enrolled and randomized into an SMBG group (n=37) and a control group. The patients in the SMBG group performed no more than 10 blood glucose tests per month in the postprandial phase. The control group performed SMBG in a random fashion. HbA1c reduction was significantly higher in the SMBG group, which performed postprandial monitoring, compared with the control group (−0.4% vs. −0.1%). 8
The use of SMBG enables the patient to monitor glycemic excursions and identify any effect of behavior or treatment on glycemic variability and control. Therefore, SMBG supports minimization of glycemic variability and reduces the risk for diabetes complications. 9 Glycemic variability is reported to be associated with impairment of endothelial function 10 and cognitive performance. 11
The Retrolective Study Self-Monitoring of Blood Glucose and Outcome in Patients with Type 2 Diabetes (ROSSO) Study is a retrospective, epidemiological cohort study that reported that nonfatal micro- and macrovascular event rates are lower in people with type 2 diabetes who performed SMBG compared with those who did not perform SMBG (7.2% vs. 10.4%). 12 Also, fatal event rates were lower in the SMBG group compared with the non-SMBG group (2.7% vs. 4.6%). 12 In summary, the study reported a reduction in morbidity and mortality in diabetes patients who performed SMBG compared with those who did not perform SMBG. 12
Recently published results from the STeP Study, which enrolled 483 poorly controlled (HbA1c ≥7.5%), insulin-naive people with type 2 diabetes, showed significantly greater reductions in mean HbA1c in the structured testing group compared with the active control group. 13 The data confirmed that appropriate use of structured SMBG significantly improves glycemic control and facilitates more timely/aggressive treatment changes in non–insulin-treated type 2 diabetes. 13
SMBG has been shown to be able to predict severe hypoglycemia, providing a potential tool to trigger self-regulatory prevention of significant hypoglycemia. 14 Furthermore, in patients with type 2 diabetes, SMBG can heighten patients' awareness of the disease and of the impact of lifestyle on blood glucose. 15 SMBG is also accompanied by challenges for the patients. 15 Consistently high blood glucose readings could potentially cause anxiety and self-blame. 15 As a consequence, the purpose of monitoring and interpretation of measurements should be reinforced in educational sessions. 15 Performing structured and standardized SMBG is required to successfully face the challenges. As demonstrated by the United Kingdom Prospective Diabetes Study Group (UKPDS), intensive blood glucose control in patients with type 2 diabetes is able to reduce both micro- and macrovascular complications. 16
Recommendations on SMBG in Guidelines
European Society of Cardiology and European Association for the Study of Diabetes
The “Guidelines on Diabetes, Pre-Diabetes, and Cardiovascular Diseases” of the European Society of Cardiology (ESC) and the European Association for the Study of Diabetes (EASD) emphasize the importance of SMBG in diabetes patients with cardiovascular disease. 17 In the ESC/EASD Guidelines, SMBG is acknowledged as a major part of comprehensive management to reduce cardiovascular risk in patients. The guidelines point out that SMBG is an indispensable prerequisite for a successful management and therapy. It is outlined that a mutual reviewing of the SMBG protocols at each patient visit allows physicians and patients to become partners in treatment.
International Diabetes Federation
The “Guideline for Management of Postmeal Glucose” of the International Diabetes Federation (IDF) gives recommendations for the targets of postmeal glucose and how they should be assessed. 18 The guidelines emphasize that 2-h postmeal plasma glucose should not exceed 7.8 mmol/L (140 mg/dL) as long as hypoglycemia is avoided. They recommend considering self-monitoring of postmeal blood glucose with SMBG because it is currently the most practical method for monitoring postmeal glycemia. The 2-h timeframe for measurement of plasma glucose concentrations is recommended because it conforms to guidelines published by most of the leading diabetes organizations and medical associations.
The IDF “Guideline for Management of Postmeal Glucose” also addresses the topic of the frequency and timing of SMBG. They generally recommend that people treated with insulin perform SMBG at least three times per day. In non–insulin-treated diabetes, SMBG should be individualized to each person's treatment regimen and level of glycemic control, despite a lack of evidence regarding timing and frequency of SMBG.
The IDF “Guideline on Self-Monitoring of Blood Glucose in Non-Insulin Treated Type 2 Diabetes” 19 is considered to be the first guideline that gives global recommendations for SMBG. According to these guidelines currently there is no clear evidence regarding optimal SMBG regimens in non–insulin-treated type 2 diabetes. It is mentioned, however, that in these patients it is often not necessary to perform SMGB on a daily basis. 19
The guidelines differentiate three levels of diabetes care depending on the regions where they are applied: minimal care, standard care, and comprehensive care. In standard care, the global IDF guidelines recommend SMBG for all newly diagnosed people with type 2 diabetes as an integral part of self-management education. Furthermore, SMBG should be available on an ongoing basis in those on insulin treatment.
The guidelines emphasize that SMBG should be considered also on an ongoing basis for people using oral glucose-lowering agents to provide information on hypoglycemia, to assess glucose excursions due to medications and lifestyle changes, and to monitor changes during intercurrent illness. The guidelines also recommend performing annually a structured assessment of self-monitoring skills, of the quality and use made of the results obtained, and of the equipment used.
International Society for Pediatric and Adolescent Diabetes
The “Clinical Practice Consensus Guidelines” of the International Society for Pediatric and Adolescent Diabetes (ISPAD) give specific recommendations for the assessment and monitoring of glycemic control in children and adolescents with diabetes. 20,21 The guidelines highlight SMBG as an essential tool in the optimal management of childhood and adolescent diabetes. SMBG should be prescribed at a frequency to optimize each child's diabetes control because frequency of SMBG correlates with glycemic control.
The guidelines point out that early detection of lower glucose values prior to symptomatic hypoglycemia may allow correction with a decreased risk of overcorrection and resultant hyperglycemia. They emphasize that SMBG should be performed regularly. Frequency of SMBG should be individualized and comprise a combination of fasting and postprandial measurements. Once glycemic goals have been achieved, several fasting values a week and daily postprandial values, taken after the biggest meal, are adequate while the values remain within the target range. Blood glucose also should be measured to show levels of blood glucose in response to the action profiles of insulin, after food intake, and in association with vigorous sport or exercise. During acute illness or in case of symptoms of hyper- or hypoglycemia, testing should be performed more frequently, and patients should be in close contact with their diabetes care team for advice.
In the guidelines it is pointed out that a successful application of intensified diabetes management with multiple injection therapy or insulin infusion therapy requires frequent SMBG (four to six times a day) and regular, frequent review of the results to identify patterns requiring adjustment to the diabetes treatment plan.
European Consensus Statement
In 2009 a European consensus statement on SMBG was published. It intended to facilitate and enhance a structured approach to SMBG throughout Europe and presented, beyond guideline-based approaches, clinical recommendations for frequency and timing of SMBG in people with diabetes 22 as well as targets for pre- and postprandial blood glucose levels. 22
HbA1c target
An overall HbA1c target of ≤6.5% in people with diabetes is recommended. Aiming for lower HbA1c levels is suggested, if this can be achieved safely. An HbA1c in the normal range (<6.0%) is recommended for pregnant women and for those planning pregnancy. High-risk patients presenting with microvascular and/or macrovascular disease may require a modification of HbA1c targets. Patients with a high risk of hypoglycemia and patients with hypoglycemia unawareness may also be in need for an adaptation of HbA1c targets. In these patients, HbA1c targets may be increased to <7% or <7.5%.
Frequency of testing
The recommended frequency of testing depends on the type of diabetes, the treatment approach, and the educational level. For people on an intensive basal–bolus insulin regimen four to eight tests every day are recommended. SMBG should be performed primarily preprandially and at bedtime. Postprandial testing should be performed seven to 10 times per week, and nocturnal testing should be performed once weekly.
Patients on a basal or premixed insulin treatment should test two to four times every day with SMBG primarily preprandially and including postprandial testing one or two times every day. Performing nocturnal tests is recommended once every week or every 2 weeks. For type 2 diabetes patients who are on diet or oral agents, testing is recommended up to six to eight tests per week, with an equal number of preprandial and postprandial tests. For people with diabetes who are not on insulin or who do not test frequently, blood glucose should be measured in couplets (pre- and postprandial) to provide meaningful information. For the patients, a scheme of a seven-point monitoring per day once per week or once per month may also be beneficial.
SMBG may be recommended at time of diagnosis of type 2 diabetes in order to improve patients' awareness of lifestyle modification and treatment. At this stage, a few SMBG tests are recommended for all patients (three to five tests per week). A high frequency of testing (four to eight tests per day or more) is recommended during pregnancy. In pregnant women, postprandial blood glucose testing should be reduced to 1 h postmeal. Frequent blood glucose testing is recommended in high-risk patients with known coronary artery disease, neuropathy, or hypoglycemia unawareness to help recognize episodes of hypoglycemia. More frequent nocturnal blood glucose testing is suggested in patients experiencing severe hypoglycemia.
Targets for preprandial blood glucose
A preprandial blood glucose target of <6 mmol/L (108 mg/dL) is recommended for the majority of patients. The targets for children are based on the ISPAD guidelines: preschool children (0–6 years), 5–8 mmol/L (90–144 mg/dL); older children (≥7 years), 4–8 mmol/L (72–144 mg/dL). A less stringent target of 5–7 mmol/L (90–130 mg/dL) may be suggested in patients with known coronary artery disease or risk of severe hypoglycemia. In pregnant women, a preprandial blood glucose of 3.3–5.0 mmol/L (60–90 mg/dL) is recommended.
Targets for postprandial blood glucose
The consensus pointed out that postprandial blood glucose testing is one of the key elements of SMBG. The postprandial testing target of<7.8 mmol/L (140 mg/dL) taken 2 h after a meal is the ideal target in most people with type 1 and type 2 diabetes. However, this should always be achieved within the limits of maximal safety in order to avoid hypoglycemia. In pregnant women, a 1-h postprandial blood glucose of <7.8 mmol/L (140 mg/dL) and a 2-h postprandial blood glucose of <6.6 mmol/L (120 mg/dL) is recommended.
European Consensus Document on SMBG in Clinical Cases
Recently, a consensus of European experts has presented typical clinical settings in which SMBG could be useful and recommended.
23
The consensus focused on nine clinical cases that address aspects of the daily clinical practice.
23
The cases involved intermittent or continuous SMBG and were considered to be role models for clinical situations that can be frequently detected: 1. Pediatric patients with type 1 diabetes 2. Patients with gestational diabetes 3. Patients with type 2 diabetes with elevated postprandial blood glucose levels 4. Patients with type 2 diabetes with lack of motivation and adherence 5. Patients with type 2 diabetes at risk of hypoglycemia or with hypoglycemia unawareness 6. Patients with type 2 diabetes with coronary artery disease or with type 2 diabetes with nephropathy 7. Elderly patients with type 2 diabetes (≥80 years of age)
The Expert Panel Meeting: Methodology and Findings
In July 2010, experts in diabetology and endocrinology formed an expert panel to create recommendations for patterns of SMBG in type 2 diabetes. A scientific survey was conducted to gather initial feedback from the group and identify common challenges. The expert panel convened to clarify the current situation, discuss the issues, and consider priorities for action. A series of recommendations were generated by the group, based on the local experiences of the experts, in addition to evidence in the medical literature and existing blood glucose management guidelines—in particular, the recent IDF recommendations.
Overall, the feedback identified the need to educate diabetes caregivers and patients on SMBG in type 2 diabetes in a structured approach. In summary, the main findings of the survey completed by the expert panel highlighted the following:
The level of implementation of SMBG varies among countries. In many countries, blood glucose testing strips are not reimbursed, which can act as a disincentive to patients to regularly self-monitor their blood glucose. Furthermore, not all countries target the same groups of patients for screening: some screen the whole population, whereas others offer no routine screening. Standardization of SMBG is generally poor, among specialists as well as among general practitioners and diabetes educators. Not all doctors routinely recommend SMBG in type 2 diabetes. Consensuses/guidelines for clinicians to teach patients how and when to self-test their pre- and postprandial glucose levels are lacking. There was general consensus that SMBG should be implemented in a structured way. Collaboration and interdisciplinary discussion should be encouraged and improved among specialists, such as endocrinologists, general practitioners, and diabetes educators.
Recommmendations for SMBG Schemes in Type 2 Diabetes
Summary of the current situation
Today recommendations for an individual regimen of SMBG for individual therapeutic approaches across the diabetes continuum are scarce. In general, merely potential daily frequencies for SMBG are recommended.
In the majority of recommendations, timing for SMBG or specific information on the length of SMBG approaches is not included.
In 2009, the IDF Guidelines on “Self-Monitoring of Blood Glucose in Non-Insulin Treated Type 2 Diabetes” were published. 13,19 The recommendations present several examples for a focused regimen, which included a five- and seven-point profile and a staggered SMBG regimen.
Furthermore, three examples of low-intensity SMBG regimen were given: meal-based testing, detection/assessment of fasting hyperglycemia, and detection of asymptomatic hypoglycemia.
The expert panel suggested two schemes for SMBG in type 2 diabetes: less intensive testing in type 2 diabetes (Fig. 1) and intensive testing in type 2 diabetes (Fig. 2). The group agreed that the lengths of the periods of testing depend on the individual situations and may range from an intermittent 3-day monitoring once a month to a continuous and daily SMBG (Fig. 3).

Scheme 1: less intensive testing in type 2 diabetes. Characteristics of the scheme are the focus on paired meal testing (pre- and postprandial) once per day to identify the dynamics of glucose levels in response to a meal. The duration of testing is one paired meal testing per month, 1 week/month, 3–7 days/week, continuous paired testing.

Scheme 2: intensive testing with seven tests per day over a minimum of 3 days up to 7 days for educational purposes, for adjustment of therapy, or for diet. Characteristics of the scheme are the focus on the dynamics of glucose levels per day to identify the variability of glucose levels. The duration of testing is a minimum of 3 days/week to 1 week/month, with continuous self-monitoring of blood glucose.
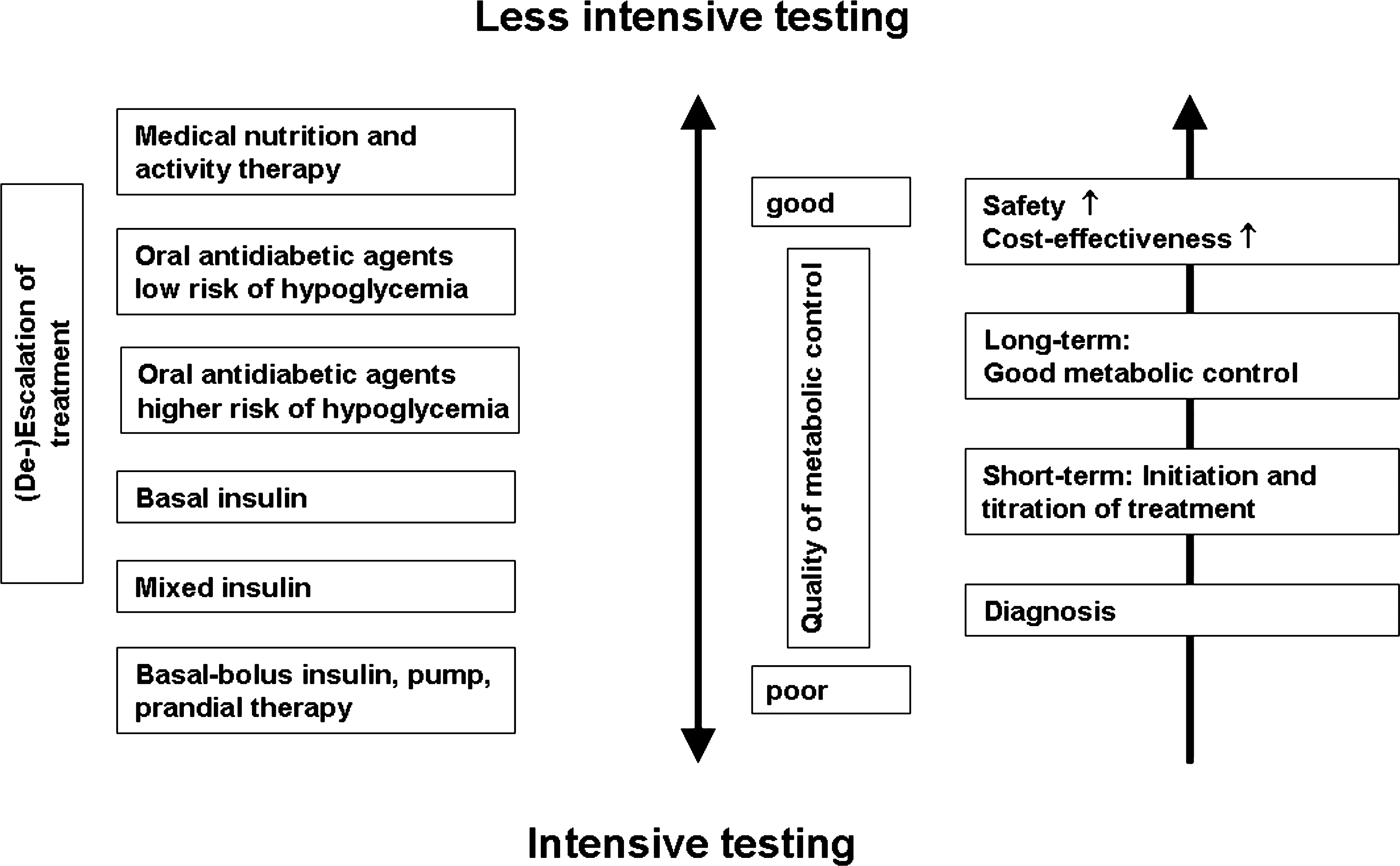
Intensity of testing should be oriented toward several variables (e.g., quality of metabolic control, treatment approaches, and the risk of hypoglycemia).
This section is considered to present simple, clinically applicable, and individualized SMBG strategies for various clinical scenarios aiming at supporting optimized and efficacious treatment approaches. We acknowledge that the schemes are based on knowledge of the expert panel. They have not been scientifically validated in clinical studies, and they will require further evaluation in the future.
The two SMBG schemes (Figs. 1 and 2) that could be applied as an intermittent or continuous approach, respectively, are suggested.
The two schemes could be allocated to various clinical scenarios:
• Initiation of lifestyle changes only (newly diagnosed type 2 diabetes). SMBG Scheme 1 (Fig. 1) is suggested in order to facilitate diabetes education, understanding, and behavioral changes. The duration of testing is 3 days for 1–12 weeks: for stable/good metabolic control, 3 days to 1 week, compared with unstable/poor metabolic control, 3 days to 1 week per month.
• Initiation of a first oral glucose-lowering agent (newly diagnosed or longer-term type 2 diabetes). SMBG Scheme 1 (Fig. 1) is suggested in order to facilitate diabetes education, understanding, and behavioural changes. The duration of testing is 3 days for 1–12 weeks: for stable/good metabolic control, 3 days per month, compared with unstable/poor metabolic control, 3 days to 1 week per month.
• Initiation of a second or third oral glucose-lowering agent and initiation of glucagon-like peptide-1 analogs (longer-term type 2 diabetes). SMBG Scheme 1 (Fig. 1) is suggested in order to support the aim to treat to target and to facilitate diabetes education, understanding, and behavioral changes. The duration of testing is 1–12 weeks: for stable/good metabolic control, 3 days per month, compared with unstable/poor metabolic control, 3 days to one week per month.
• Initiation of a combination therapy (oral glucose-lowering agents and insulin). In view of the eventuality of hypoglycemic episodes, short-term administration of Scheme 2 (Fig. 2) is considerable. Return to Scheme 1 as soon as the patient achieves the individual metabolic goals. The duration is 3 days for 1–12 weeks: for stable/good metabolic control, 3 days to 1 week on Scheme 2, compared with unstable/poor metabolic control, 3 days to 1 week or more on Scheme 2.
• Initiation of mixed (conventional) insulin therapy also possibly in combination with oral agents. Short-term administration of Scheme 2 (Fig. 2) is considerable. Return to Scheme 1 as soon as the patient achieves the individual metabolic goals. The duration is 3 days for 1–12 weeks: for stable/good metabolic control, 3 days to 1 week on Scheme 2, compared with unstable/poor metabolic control, 3 days to 1 week or more on Scheme 2.
• Initiation of basal-bolus insulin or insulin pump therapy. For the purpose of glycemic assessment, patient safety, and optimized therapy, implementation of Scheme 2 (Fig. 2) is advisable. The duration is the continuous approach of Scheme 2.
The two schemes are considered as a starting point. Intensity and frequency should be further individualized. Temporary modifications should include, among others, acute or long-term concomitant illnesses, deterioration of HbA1c, pregnancy or planning of pregnancy, hypoglycemic episodes and risk of hypoglycemic episodes, driving a car, and temporary medication to interfere with blood glucose levels.
Conclusions
SMBG has proven to be a possible supplemental tool to verify glucose excursions in people with type 2 diabetes. It is increasingly recognized that SMBG should be implemented in type 2 diabetes in a more structured and standardized approach. A less intensive and an intensive scheme for SMBG is recommended across the type 2 diabetes continuum.
Its length and frequency of performance depend on the clinical circumstances and the level of metabolic control. In general, the level of implementation of SMBG in type 2 diabetes should be improved, combined with a wider use of structured approaches and a better interpretation of glucose levels to reach the treatment targets. SMBG in type 2 diabetes is central to the achievement of long-term glycemic control and an essential part to prevent acute and chronic complications in type 2 diabetes. SMBG needs therapeutic feedback from the care providers and the patient to generate the best benefit.
Footnotes
Acknowledgments
The expert panel was supported by an unrestricted educational grant of Bayer HealthCare.
Author Disclosure Statement
O.S. has received funds from Bayer HealthCare and Roche Diagnostics GmbH. No competing financial interests exist for H.A., T.B., A.C, P.D., A.F., W.G., K.H., P.K., I.S., and B.V.