
Abstract
Aims:
This study performed a systematic review and meta-analysis on glycemic control and pregnancy outcomes in women with type 1 diabetes mellitus (T1DM) treated with lispro (LP) versus regular insulin (RI) since before pregnancy.
Methods:
We performed a MEDLINE and EMBASE search. Abstracts (and full articles when appropriate) were reviewed by two independent researchers. Inclusion criteria were patients with T1DM, data on women treated with RI and LP since before pregnancy until delivery in the same article, at least five pregnancies in each group, and information on at least one pregnancy outcome. Quality assessment was performed using the Newcastle–Ottawa Quality Assessment Scale for cohort studies.
Results:
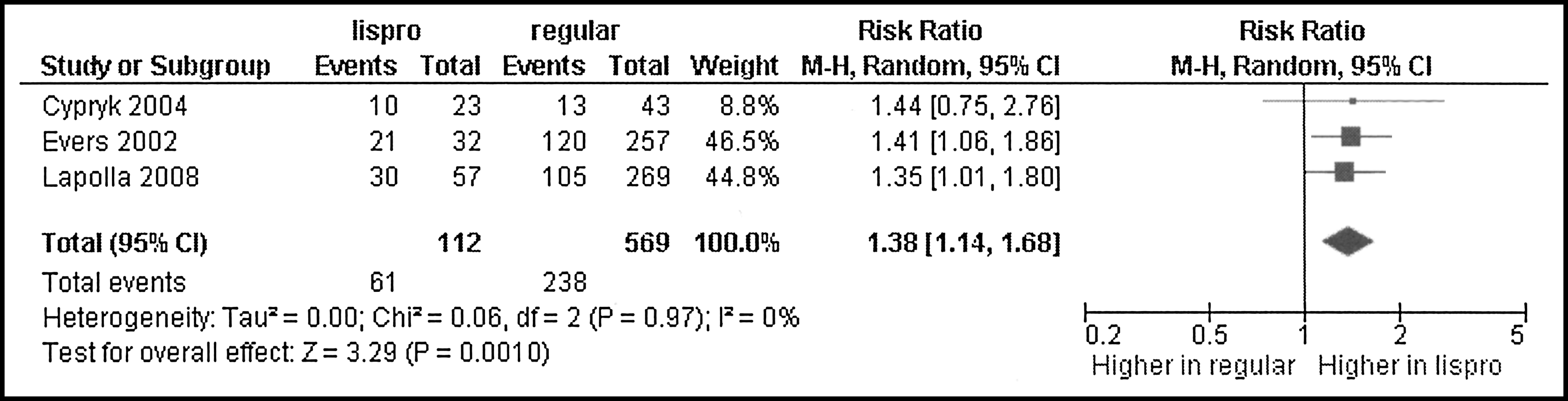
Outcome data were summarized with Revman version 5.0 (ims.cochrane.org/revman/download [The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark]), applying a random effects model. Two hundred sixty-seven abstracts were identified, and four full articles fulfilled inclusion criteria, all of them corresponding to observational studies. Baseline characteristics were similar in women treated with LP or RI. Regarding outcome data, no differences between LP and RI groups were observed in hemoglobin A1c, gestational age at birth, birth weight, and rate of diabetic ketoacidosis, pregnancy-induced hypertension, pre-eclampsia, spontaneous miscarriages, interruptions, total abortions, cesarean section, preterm birth, macrosomia, small-for gestational-age newborns, stillbirth, neonatal and perinatal mortality, neonatal hypoglycemia, and major malformations. The rate of large-for-gestational age newborns was higher in the LP group (relative risk 1.38; 95% confidence interval 1.14–1.68).
Conclusions:
In relation to women with T1DM treated with RI, those treated with LP display similar baseline characteristics and no differences in metabolic control or perinatal outcome with the exception of a higher rate of large-for-gestational-age newborns.
Introduction
Insulin lispro (LP) has been a treatment option for diabetes mellitus since its Food and Drug Administration approval in 1996. Compared with regular insulin (RI), LP seems helps to reduce postprandial and interprandial glycemia and also nocturnal hypoglycemia; 4 owing to this, LP may help to improve both glycemic control and outcomes in pregnancy with diabetes.
In 1999 initial reports of LP use during pregnancy suggested an association with congenital anomalies 5 and a high prevalence of proliferative retinopathy. 6 However, this has not been confirmed in subsequent publications. 7 –10
LP is approved for pregnancy use since August 2001, but there is limited evidence of its influence on glycemic control and pregnancy outcomes in pregnancy with diabetes in general and in women with T1DM in particular. With this background, the aim of this study is to perform a systematic review and meta-analysis on the impact of LP (vs. RI) on glycemic control and pregnancy outcomes in women with T1DM.
Subjects and Methods
The review protocol has not been published, and this systematic review does not have a registration number. The MOOSE Group 11 and the PRISMA Statement 12 guidelines for systematic reviews and meta-analyses have been followed.
The chosen inclusion criteria were: (1) women with T1DM; (2) data on women treated with RI and LP since before pregnancy until delivery in the same article; (3) at least five pregnancies in each group; and (4) information on at least one pregnancy outcome.
Medline and EMBASE searches were performed using the search detailed in the Appendix; the last update was performed on January 11, 2010. Abstracts (and full articles when appropriate) were reviewed by two independent researchers and if required because of differences set by consensus with a third one.
In order to asses the quality of individual studies, we decided to use the Newcastle–Ottawa Quality Assessment Scale 13 for cohort studies and CONSORT Statement 14 for randomized controlled trials.
We decided to collect information on the following maternal descriptive characteristics and outcomes: ethnic origin, age, body mass index, chronic hypertension, duration of diabetes, presence of diabetes complications, gestational age at first pregnancy visit, glycosylated hemoglobin (HbA1c) at conception, in the first, second, and third trimesters, and at the end of pregnancy, ketoacidosis, rate of severe hypoglycemia, insulin requirements in the three trimesters of pregnancy, pregnancy-induced hypertension, pre-eclampsia, and cesarean section.
As to fetal outcomes, we chose to collect information on spontaneous and induced abortions, preterm birth, gestational age at delivery, birth weight, macrosomia (defined as birth weight ≥4,000 g), babies small for gestational age (SGA) (birth weight <10th percentile), babies large for gestational age (LGA) (birth weight >90th percentile), stillbirth (babies born dead beyond 180 days of pregnancy), perinatal mortality (rate of deaths from 180 days of pregnancy to 28 days of life), neonatal mortality (rate of neonatal deaths before the 28th day of life), major and minor congenital malformations, and neonatal hypoglycemia.
Baseline characteristics, metabolic control, and outcome data were extracted using predefined templates. Publications were reviewed by two independent researchers, and if required, differences were set by consensus with a third one.
Background characteristics were summarized, weighting by SE. Formal statistical comparison was not deemed necessary for descriptive purposes.
Outcome data were summarized with Revman version 5.0 (ims.cochrane.org/revman/download [The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark]). When the heterogeneity was ≥50% or the number of studies was three or fewer, a random effects model was applied.
Results
Two hundred sixty-seven abstracts were identified, and four full articles fulfilled the inclusion criteria (Fig. 1).

Flow chart of articles through the review process.
In the publication of Lapolla et al., 15 18% of the women using LP stopped it after the first trimester. This article would not have qualified for inclusion, but the authors were requested to provide the data corresponding to women under LP treatment throughout pregnancy; this is the information included in the meta-analysis.
The four articles corresponded to observational studies, and all of them have qualified as well by the Newcastle–Ottawa Quality Assessment Scale.
The articles included in this review 9,15 –17 are summarized in Table 1.
See text.
LP, lispro; RI, regular insulin.
The baseline characteristics are similar in pregnant women treated with LP relative to those treated with RI in terms of age, body mass index, duration of diabetes, pregestational care, and presence of chronic hypertension (Table 2).
LP, lispro; RI, regular insulin.
In terms of the metabolic outcomes—HbA1c (first measurement and in the three trimesters) and ketoacidosis episodes—no differences have been observed between groups (Table 3).
CI, confidence interval; HbA1c, glycosylated hemoglobin; MD, mean difference; NS, not significant; RR, risk ratio, SGA, small for gestational age newborns.
In terms of maternal outcomes, no differences between the groups were observed in prepregnancy-induced hypertension, pre-eclampsia, and cesarean section. As to fetal outcomes, no difference was observed in miscarriages, terminations, total abortions, gestational age at delivery, preterm birth, birth weight, rate of SGA newborns, major malformations, neonatal hypoglycemia, and stillbirth or perinatal mortality (Table 3). The only difference was seen in the rate of LGA newborns, which was higher in the LP group with relative risk of 1.38 and 95% confidence interval of 1.14, 1.68 (Fig. 2).
Information on some of the predefined variables of interest (maternal severe hypoglycemia or neonatal mortality) was not provided in the publications.
Discussion
In this systematic review and meta-analysis comparing LP versus RI in pregnant women with T1DM using these insulins since before pregnancy, maternal baseline characteristics and maternal and fetal outcomes were similar with the exception of the rate of LGA newborns.
This had already been observed in a multicentric Italian study, one of the individual articles included in this meta-analysis, 15 but not in a recent article where in fact the rate of SGA was higher in the LP group. 18 The higher rate of LGA in this meta-analysis cannot be attributed to a worse metabolic control in the LP group; differences in HbA1c were not significant, and, in either case, the trend was to a lower HbA1c in the LP group. In the aforementioned Italian study, 15 the higher rate of LGA was observed despite a lower HbA1c in the first trimester in the LP group. Overall, this suggests that the higher rate of LGA in the LP group would not be mediated through glycemic control. It could be mediated by other factors known to influence fetal growth (i.e., smoking habit or weight gain during pregnancy 16 ), of which we do not have information for the studies included in the meta-analysis. However, the homogeneity across the studies is remarkable: I 2 was 0%, and for an overall relative risk of 1.38, the relative risk of individual studies went from 1.35 to 1.44. Another possibility would be an effect of LP itself. LP has been reported not to cross the placenta in studies performed in the third trimester, with no report addressing first trimester transfer. 19,20 However, LP could have an indirect effect through a placental action.
The insulin/insulin-like growth factor (IGF) system—insulin, IGF type 1 (IGFI), IGF type 2, and various IGF-binding proteins—is implicated not only in the regulation of fetal growth and development but also in that of the placenta. 21 LP insulin homology to IGFI is higher than that of RI. 22 Placenta expresses both IGFI and insulin receptors on both the maternal and fetal sides. Insulin receptors display a temporal pattern, decreasing their concentration in the maternal side and increasing that on the fetal side as pregnancy progresses. 23 As for IGFI receptors, they are mainly expressed in the maternal side and do not experience significant variations across pregnancy. Thus, the presence of IGFI receptors in the maternal side of the placenta throughout pregnancy opens the possibility of an indirect effect of maternal insulin on the fetus, and maternal insulin being LP or RI could have a differential effect.
The most important limitation of this study is that it includes a small number of studies, and all of them are retrospective/cohort studies. There are very few randomized controlled trials addressing use of LP during pregnancy, but they have not fulfilled inclusion criteria of this meta-analysis because they either initiated LP after the first trimester 24 or addressed women with gestational diabetes. 25,26 The strength of this study is that it constitutes the summary of the best available information of LP versus RI use in women in T1DM. We did our best to aim at the information being as unequivocal as possible; the inclusion criteria asked for separate information on T1DM, use of the same type of insulin throughout pregnancy, and availability of a comparison group.
The use of LP insulin during pregnancy has been the subject of a recent narrative review that did not use exclusion criteria. Findings were similar to those reported here, but the authors emphasized the trend toward lower HbA1c in the LP group, whereas the increase in LGA was minimized. 27
In conclusion, in pregnant women with T1DM treated with LP versus RI since before pregnancy, we observed no difference in baseline characteristics, metabolic control, and maternal and fetal outcomes with the exception of a higher rate of LGA newborns in the LP group. It is important that this issue be studied by other authors (ideally in a randomized controlled trial) and that newborn body composition also be addressed to better understand differences in LGA. Meanwhile, the conclusion should be that there is no evidence of a beneficial effect of LP use during pregnancy.
Footnotes
Acknowledgments
We thank Prof. A. Lapolla and M.G. Dalfrà for providing the information on women treated with LP insulin throughout pregnancy.
Author Disclosure Statement
C.G.B., A.C.B., and R.C.P. declare that they have received reimbursement for attending a symposium and/or a fee for speaking from Lilly and NovoNordisk Pharma. I.G.S. has no competing interests.
Appendix
| 1. exp lispro |
| 2. exp Humalog |
| 3. exp insulin analog |
| 4. 1 or 2 or 3 |
| 5. exp pregnancy |
| 6. 4 and 5 |