
Abstract
Background and Methods:
The accuracy and precision of three blood glucose meters (BGMs) were evaluated in 600 hospitalized patients with type 1 (n = 200) or type 2 (n = 400) diabetes. Capillary blood glucose values were analyzed with Accu-Chek® Aviva [Roche (Hellas) S.A., Maroussi, Greece], Precision-Xceed® [Abbott Laboratories (Hellas) S.A., Alimos, Greece], and Glucocard X-Sensor® (Menarini Diagnostics S.A., Argyroupolis, Greece). At the same time plasma glucose was analyzed using the World Health Organization's glucose oxidase method.
Results:
Median plasma glucose values (141.2 [range, 13–553] mg/dL) were significantly different from that produced by the BGMs (P < 0.001). The Accu-Chek Aviva underestimated hypoglycemia (plasma glucose ≤55 mg/dL) by a mean difference of 4.1 mg/dL (95% confidence interval [CI] 0–28 mg/dL), and the Precision-Xceed did so by a mean difference of 6.2 mg/dL (95% CI 0–29 mg/dL); the same was true for the Glucocard X-Sensor by a mean difference of 9.1 mg/dL (CI 0–57 mg/dL) (P < 0.001 for all BGMs). Hyperglycemia (plasma glucose ≥250 mg/dL) was overestimated with the Accu-Chek Aviva and the Precision-Xceed by a mean difference of 4.8 mg/dL (95% CI 0–41 mg/dL) and 10.4 mg/dL (CI 0–92 mg/dL), respectively; the same was true for the Glucocard X-Sensor by a mean difference of 20.3 mg/dL (95% CI 0–100 mg/dL) (P < 0.001 for all BGMs). Asymptomatic hypoglycemia was detected in 28% of type 1 and in 18% of type 2 diabetes patients. In all cases, the BGMs were unreliable in sensing hypoglycemia. Multivariate linear regression analysis demonstrated that low blood pressure and hematocrit significantly affected glucose measurements obtained with all three BGMs (P < 0.05).
Conclusions:
In hospitalized diabetes patients, all three frequently used BGMs undersensed hypoglycemia and oversensed hyperglycemia to some extent. Patients and caregivers should be aware of these restrictions of the BGMs.
Introduction
Study Design and Patients
Approval was obtained from the institution's investigational review board before any data were collected, and written informed consent was signed by each patient after explanation of the study's purposes. A method-comparison study design was used to compare glucose values obtained with the three BGMs and the clinical laboratory analysis method. The dependent variables were the differences between glucose values obtained with the BGMs (fingerstick specimens) and the values obtained with the clinical laboratory method.
From December 2008 up to September 2010, hospitalized patients treated in our clinic for infections, as well as episodes of hyper- or hypoglycemia due to inadequate glycemic treatment and control, were screened during daily bedside glucose monitoring. In total, 600 patients (median age, 53 [range, 14–78] years) with type 1 (n = 200) or type 2 diabetes (n = 400) were recruited. Detailed medical history was obtained from all participants, and we excluded patients on medication that could interfere with blood glucose levels (i.e., galactose, glutathione, ascorbic acid, and xylose), as well as patients undergoing peritoneal dialysis with solutions containing icodextrin or patients receiving intravenous immunoglobulin therapy containing maltose. None of the patients studied received intravenous solutions containing maltose as a substitute for glucose or as a mean of hydration.
After explanation of the testing procedure, patient demographic and clinical data were documented. Blood samples were collected from the antecubital vein after an overnight fast of 12–16 h. A tourniquet was applied for less than 1 min, and the site to be punctured was cleaned with 70% methylated spirit. Duplicate venipuncture and fingerstick glucose measurements were taken at the same time from all subjects by two physicians. Blood samples from the same subject were used for each set of tests. Fingertip capillary blood samples were divided and randomly assayed on all three BGMs, whereas the venipuncture blood sample of each patient was dispensed into fluoride oxalate–containing tubes, centrifuged at 500 g for 5 min, and analyzed in a central laboratory with an RA-XT Technicon analyzer (Technicon Ltd., Dublin, Ireland) using the World Health Organization's glucose oxidase method (coefficient of variation <5%). The mean time from blood sampling to glucose laboratory analysis was 30 ± 5 min. All three BGMs studied use amperometry technology to analyze blood glucose values and were plasma-calibrated. As specified in the manufacturer's directions, glucose testing was performed by placing a drop (∼5 μL) of capillary blood obtained by lancing a fingertip on the reagent strip and then placing the strip into the BGM for reading. The minimum amount of blood discarded before glucose sampling was 3 mL, and none of the patients had to contribute more than one sample. After each glucose therapeutic determination, hematocrit and blood pressure were hand-logged onto a data sheet for each patient.
Hematocrit levels were analyzed by the hospital clinical laboratory with a Beckman Coulter (Brea, CA) model LH 750 hematology analyzer. Hemoglobin A1c was measured with a latex immunoagglutination inhibition method (Bayer HealthCare LLC, Elkhart, IN) with a range for subjects without diabetes of 4.0–6.0%. Blood pressure was measured three consecutive times 5 min apart, with the subject sitting, using an appropriate cuff size. The mean value of the last two measurements was used in the statistical analysis.
Test strips for BGMs with identical lot numbers, after their expiration date was checked, were used for the study. The median shelf life of the test strips once they were opened was 25 (range, 5–35) days. Before data collection, all physicians performing the BGM sampling and analysis were familiarized in the proper use of the BGMs and lancet devices.
Statistical analysis
Statistical analysis was performed using the SPSS program (version 15.0, SPSS Inc., Chicago, IL). Data are shown as mean ± SD values, unless otherwise indicated. Descriptive statistics were used for summarizing data. Difference scores between capillary and plasma glucose values were calculated for each patient. Mean difference scores and limits of agreement between the BGM values and the central laboratory glucose values were estimated by regression analysis, and a comparison of alternative models based on the highest r 2 value was made in order to find the best fitted. Paired Student's t test was used to compare differences between the parameters studied determined by different methods. Accuracy of BGMs was assessed after adjustment for low hematocrit and blood pressure values. Multivariate linear regression analysis was performed to look for factors associated with the difference scores between the laboratory value and the BGM glucose values. Values of P < 0.05 were considered as statistically significant.
Results
Paired comparison of plasma–capillary glucose values obtained with the different methods studied and limits of agreement in the presence of hypo- and hyperglycemia
The demographic and clinical characteristics of the studied population are presented in Table 1. Glucose values were normally distributed. Paired-sample t test indicated that the median value generated by the World Health Organization reference method was significantly different from that produced by the BGMs (P < 0.001). Figure 1 demonstrates the results of simple regression analysis between glucose levels (in mg/dL) measured with the BGMs and the central laboratory method. When hypoglycemia was defined as a plasma glucose level of ≤55 mg/dL, the mean difference for the Accu-Chek Aviva was 4.1 mg/dL (95% confidence interval [CI] 0–28 mg/dL), for the Precision-Xceed was 6.2 mg/dL (95% CI 0–29 mg/dL), and for the Glucocard X-Sensor was 9.1 mg/dL (95% CI 0–57 mg/dL) (P < 0.001 for all BGMs). Definition of hyperglycemia as a plasma glucose level of ≥250 mg/dL verified that the mean difference for the Accu-Chek Aviva was 4.8 mg/dL (95% CI 0–41 mg/dL), for the Precision-Xceed was 10.4 mg/dL (95% CI 0–92 mg/dL), and for the Glucocard X-Sensor was 20.3 mg/dL (95% CI 0–100 mg/dL) (P < 0.001 for all BGMs).
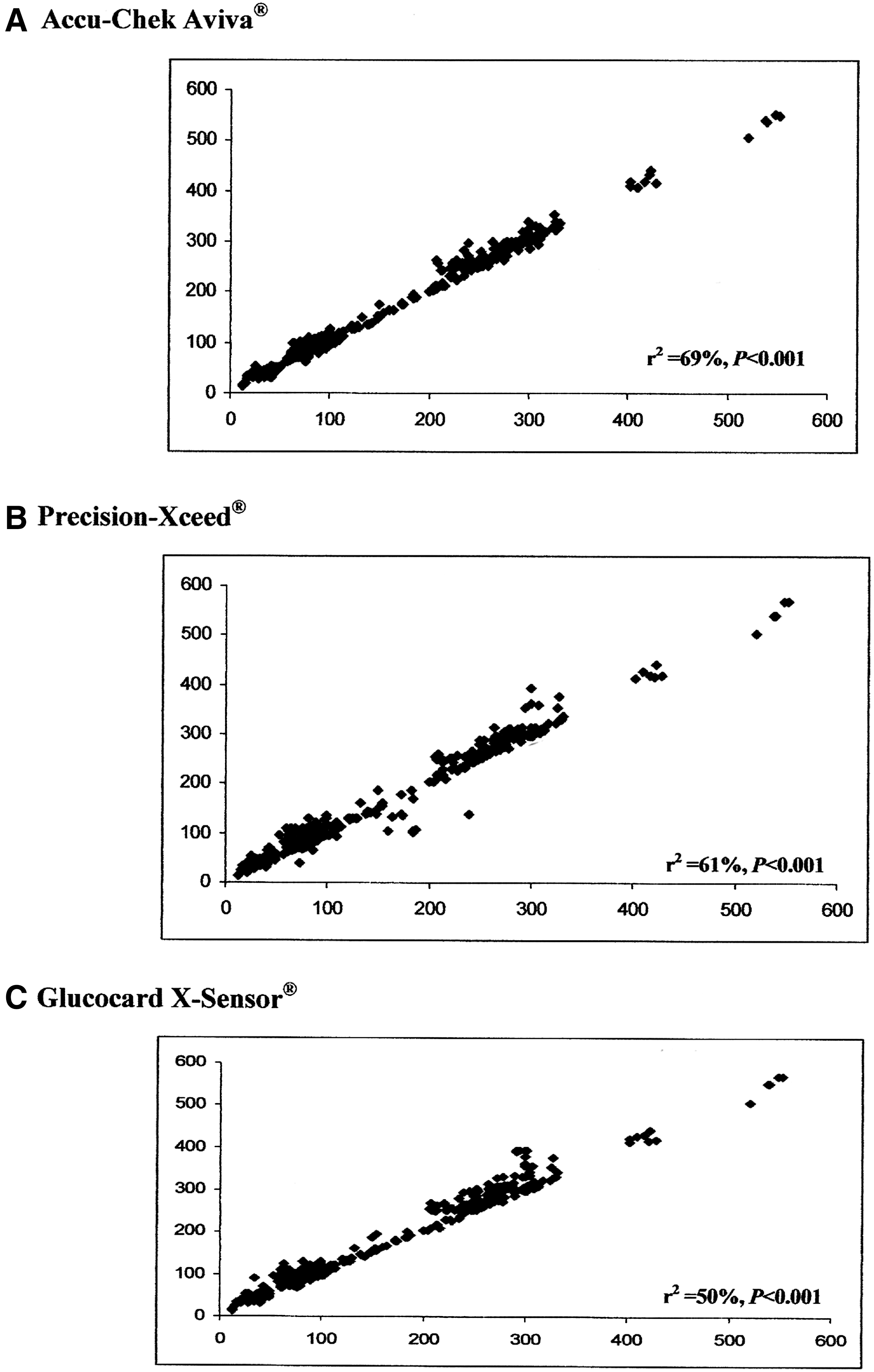
Simple regression analysis of glucose levels (in mg/dL) measured with (
Median (range) values.
HbA1c, glycated hemoglobin.
Coefficient correlations between the different methods studied for hypoglycemia and hyperglycemia
For hyperglycemia (defined by a plasma glucose value of ≥250 mg/dL), capillary glucose values obtained with all three BGMs were significant correlated with plasma laboratory values (r = 0.92 to r = 0.98, P < 0.001). The same was true for hypoglycemia (defined by a plasma glucose value of ≤55 mg/dL), although capillary glucose values obtained with the Accu-Chek Aviva and the Precision-Xceed were slightly more significantly correlated (r = 0.75, P < 0.001) with plasma laboratory values than those obtained with the Glucocard X-Sensor (r = 0.62, P = 0.005).
Precision of the BGMs in diagnosing hypo- and hyperglycemia
For plasma glucose levels of ≤55 mg/dL, all three BGMs demonstrated 50% sensitivity and 81–84% specificity in diagnosing hypoglycemia. For plasma glucose levels of ≥250 mg/dL, all three BGMs demonstrated 100% sensitivity and 75% specificity in diagnosing hyperglycemia. Asymptomatic hypoglycemia was present in 28% (n = 30) of the patients with type 1 diabetes and in 17.7% (n = 19) of the patients with type 2 diabetes. The Accu-Chek Aviva and the Precision-Xceed underdiagnosed hypoglycemia by 10% and 28%, respectively, whereas the Glucocard X-Sensor was off by 39% in all cases studied. Acute symptomatic hypoglycemia (plasma glucose values <45 mg/dL) was recorded in 88 (14.7%) patients. The Accu-Chek Aviva misdiagnosed acute hypoglycemia in 4.4% (n = 26), the Precision-Xceed in 6.5% (n = 39), and the Glucocard X-Sensor in 9.7% (n = 58) of the patients studied (P < 0.001 for all BGMs).
Hyperglycemia was overdiagnosed by 16% and 15% with the Accu-Chek Aviva and the Precision-Xceed, respectively, and by 25% with the Glucocard X-Sensor. Acute symptomatic hyperglycemia (plasma glucose values 270–360 mg/dL) was recorded in 96 (16.0%) of the patients. The Accu-Chek Aviva overdiagnosed acute hyperglycemia in 0.3% (n = 2, P = 0.007), the Precision-Xceed in 3.5% (n = 21, P < 0.001), and the Glucocard X-Sensor in 6.0% (n = 36, P < 0.001) of the patients studied.
Achievement of international accuracy goals with the BGMs
The accuracy goals recommended by the International Organization for Standardization's criteria [ISO 15197, 2004(E)] of ± 20 mg/dL for glucose values <100 mg/dL and ± 20% for glucose values >100 mg/dL for at least 95% of the results were achieved by the Accu-Chek Aviva and the Precision-Xceed with 73% (Fig. 2) and 69% (Fig. 3) of the patients' measurements, respectively, and with 55% by the Glucocard X-Sensor (Fig. 4).

Accuracy of measurements obtained with the Accu-Chek Aviva compared with central laboratory values according to the ISO NORM 15197, 2004(E) international standards.
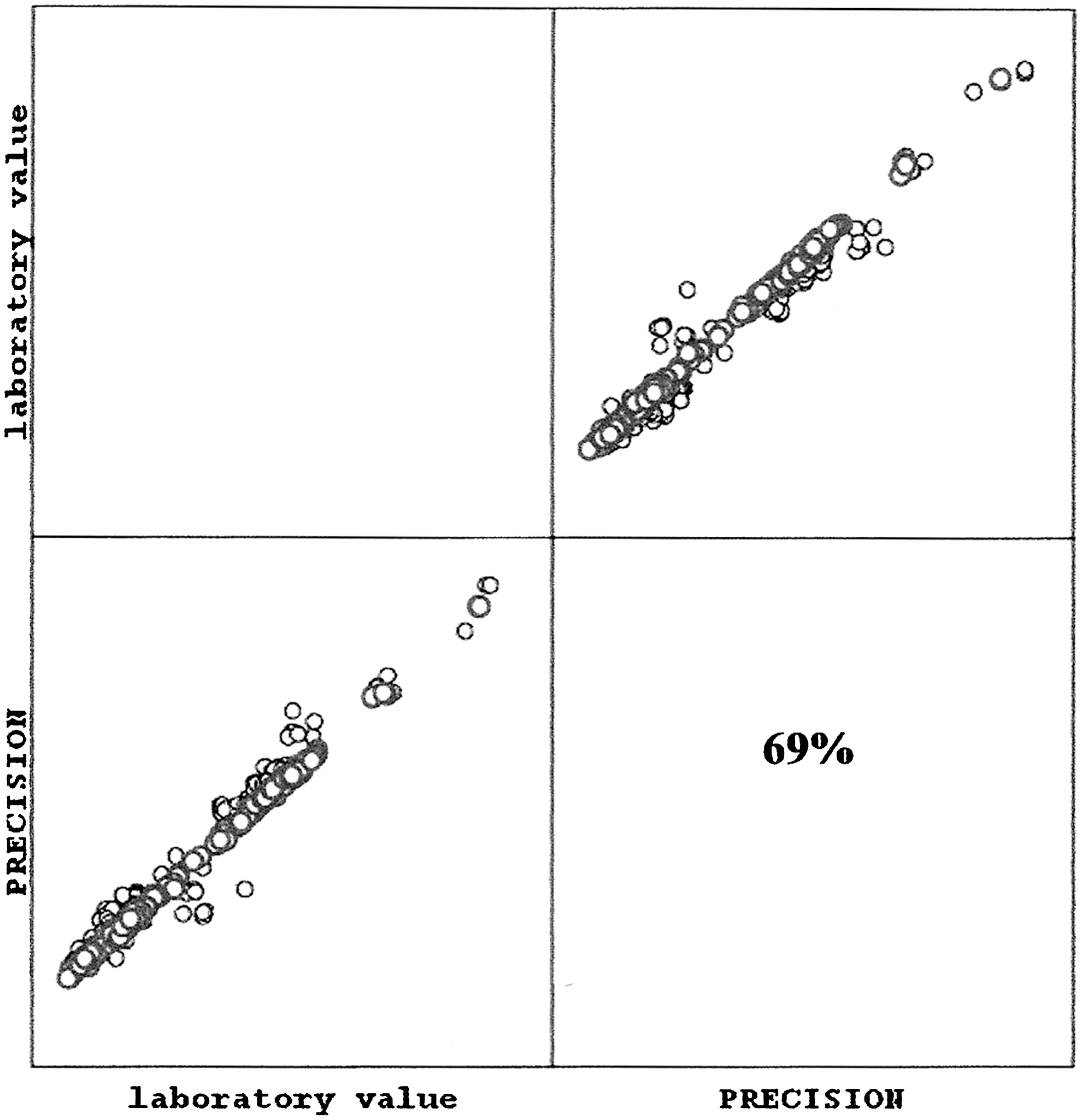
Accuracy of measurements obtained with the Precision-Xceed compared with central laboratory values according to the ISO NORM 15197, 2004(E) international standards.
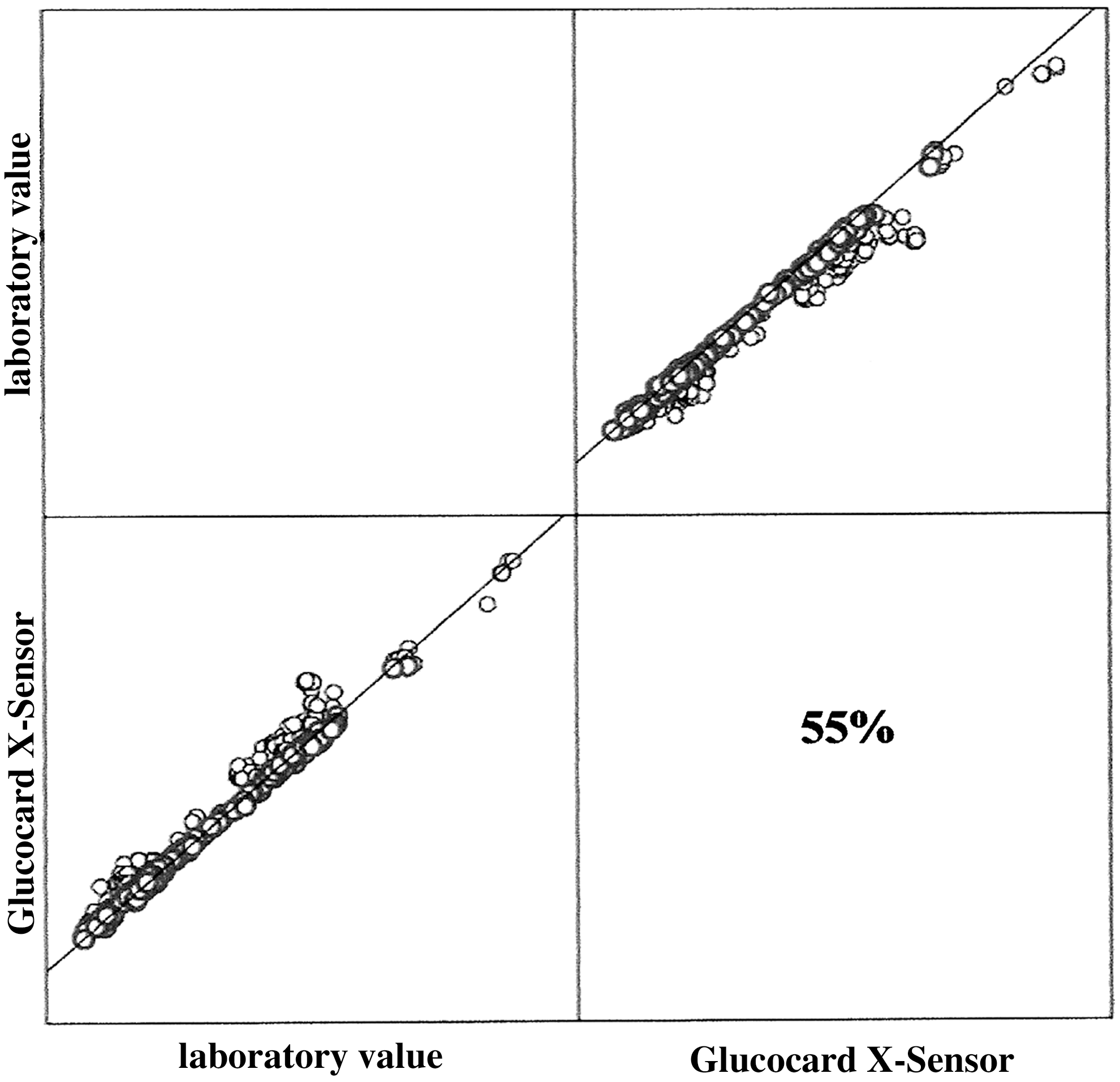
Accuracy of measurements obtained with the Glucocard X-Sensor compared with central laboratory values according to the ISO NORM 15197, 2004(E) international standards.
Clinical parameters associated with the measurement errors produced by the BGMs
In our studied patients, low hematocrit values (<30%) were recorded in 25% (n = 150) of the patients, whereas low systolic blood pressure (<110 mm Hg) in 39% (n = 234). The cut-point of systolic blood pressure <110 mm Hg corresponded to the lower 15% of systolic blood pressure distribution among the population studied. Multiple linear regression analysis showed that low hematocrit values were marginally associated with underdiagnosed hypoglycemia using the Accu-Chek Aviva measurements, whereas they were significantly associated with the Precision-Xceed and the Glucocard X-Sensor glucose measurements (Table 2). The same was true for low systolic blood pressure values, which for plasma glucose <55 mg/dL affected marginally glucose measurements obtained with the Accu-Chek Aviva and significantly those produced by the Precision-Xceed and the Glucocard X-Sensor. For overdiagnosed hyperglycemia, low systolic blood pressure and hematocrit values significantly affected glucose measurements obtained only by the Glucocard X-Sensor (Table 3).
Underdiagnosed hypoglycemia was defined as plasma glucose ≤55 mg/dL.
Overdiagnosed hyperglycemia was defined as plasma glucose ≥250 mg/dL.
Discussion
In this study we examined glycemia monitoring practices in hospitalized patients with diabetes. All three BGMs undersensed hypoglycemia and oversensed hyperglycemia to some extent. Compared with the Accu-Chek Aviva and the Precision-Xceed, the performance of the Glucocard X-Sensor in diagnosing diabetes disorders was slightly poorer.
Poor glycemic control is prevalent among hospitalized patients with diabetes and is related to longer hospital stays due to higher rates of complications during hospitalization. 1 Poor glycemic therapeutic management is recognized and studied mainly in the acute care setting among critically ill patients with diabetes; 2 however, data to support glycemia management in hospitalized patients treated for diabetes disorders continue to be established, and glycemic control in those patients who are not in intensive care remains unsatisfactory. 3,4
All of the three BGMs studied have often been reported as presenting high reliability under daily life conditions and in the hospital setting. It is notable that their systems per se have a measurement quality closely related to that of central laboratory analysis. 5 All three BGMs studied with their specific lot of test strips have been reported to fulfill the quality requirements stated in ISO DIS 15197(E). 6 However, in everyday clinical practice, we could not perform a daily quality control of the BGMs according to the manufacturer's directions and with the inclusion of both high- and low-control reagent testing. Thus, the results of this study permit us to question if all devices and lots of a qualified BGM also fulfill International Organization for Standardization requirements, especially under daily life conditions. Therefore, independent and systematic evaluation of BGMs' performance should be done on a regular basis.
Application of blood to the BGM test strip initiates a plasma-like filtrate reaction into the reagent layer of the test strip, which includes different enzymes, coenzymes, mediators, and indicators. We specifically choose three BGMs that use the same enzyme (i.e., glucose dehydrogenase), aiming to eliminate the oxygen dependency of their test strips. However, glucose dehydrogenase is not completely specific for glucose. Therefore, each one of the BGMs uses a different enzyme–coenzyme combination: specifically, Accu-Chek Aviva uses pyrroloquinoline quinone, Precision-Xceed uses nicotinamide adenine dinucleotide, and Glucocard X-Sensor uses flavin adenine dinucleotide coenzyme.
In the present study, we isolated the misleading impact of major substances studied known to affect the reliability of BGM measurements massively, and especially those known to interfere with pyrroloquinoline quinone coenzyme (i.e., maltose, galactose, and xylose); however, we could not eliminate the impact of all other substances that could potentially interfere with the BGMs' performance. 7 One such pharmaceutical parameter is acetaminophen, an analgesic and antipyretic agent, frequently used in hospitalized patients and often contained in numerous drugs. Above certain concentration levels, acetaminophen is reported to affect BGMs' measurements, causing inaccurately high glucose results. Because of different drug metabolization rates, the concentration level of acetaminophen at which BGMs' results are affected varies from patient to patient. 8 The risk of acetaminophen-containing drugs and their possible interference with the reliability of BGMs' measurements is not yet sufficiently studied, or even reported by the manufacturers in the labeling of the BGMs. Thus, our results indicate that further study of the substances frequently used in hospitalized patients that possibly may sabotage capillary glucose measurement may be needed.
In the present study, all three frequently used BGMs in hospital setting were practically unsuccessful in supporting the judicious treatment of hyperglycemia with the avoidance of hypoglycemia with a range of 1–4%. Furthermore, they inefficiently diagnosed hypoglycemia in 10% to almost 40% of the cases studied. Therefore, the results of this study permit us to partially question the daily guidance of current blood glucose monitoring for the adjustment of correction insulin doses and regimens to achieve glycemia control in hospitalized patients with diabetes.
A good understanding of the relevance of both pharmaceutical and clinical interfering factors having an impact on BGMs' measurements is needed to obtain the required quality. 9 Therefore, we further evaluated the three BGMs for clinical interferences likely to be encountered in hospitalized patients with diabetes, with the goal of identifying and discriminating BGMs' performance specifications likely to impact glycemia management during hospitalization. In accordance with previous studies, 10,11 hematocrit showed significant interference with all BGMs, with the magnitude of this interference also varying between BGMs, also possibly due to the different enzyme technology of the test strips used by each BGM. Although manufacturers set acceptable testing limits for hematocrit, BGMs do not exclude samples by hematocrit, and hematocrit is not always known at the time of testing. Proposed mechanisms include mechanical impedance of plasma diffusion into the reagent layer of the strip at lower hematocrit and decreased relative plasma volume at lower viscosity, resulting in higher diffusion of glucose. 12 The net result would potentially mask hypoglycemia in patients with anemia. 12
The effect of hematocrit on different BGMs was also examined by previous in vitro 13 and clinical 14 studies. At low hematocrit (<30%), most BGMs yielded a higher glucose result relative to plasma measurements. 13,14 Surgical patients may be most at risk for errors in glucose measurement as a result of fluctuations in hematocrit. 15 The HemoCue Glucose 201® (Hemocue AB, Ängelhom, Sweden) point-of-care system, which determines glucose concentration on lysed whole blood, might not show significant hematocrit dependence. 16 However, when tested with hospitalized patients of different ages, this was not repeatedly verified. 17 Nevertheless, BGMs that measure and automatically correct for hematocrit were recently described and had less error than other point-of-care devices. 18 Furthermore, their hematocrit-correcting feature leads to more appropriate treatment selection of patients. 18
In addition, we evaluated the impact of systolic blood pressure in the accuracy of BGMs' measurements and concluded that blood pressure interference is also a main clinical variable that differentiates BGMs. Low systolic blood pressure leads to poor perfusion, blood stagnation, and deregulation of glucose levels because of ongoing tissue metabolism. 19,20 The reduction of tissue perfusion and the increase in glucose utilization may potentially obscure the true result for capillary whole-blood samples. 21 Previous studies have evaluated hypotension (defined by systolic blood pressure <80 mm Hg) and its potential to enhance discrepancies between capillary and plasma blood glucose values for accuracy evaluation of BGMs. 22 Furthermore, inaccuracy of the BGM when compared with laboratory plasma glucose was demonstrated in medical intensive care unit patients with poor peripheral blood perfusion. 23 Both glucose dehydrogenase– and glucose oxidase–based BGMs previously demonstrated that in hypotensive patients (systolic blood pressure <90 mg/dL), capillary glucose values differed significantly from those of the central laboratory. 24,25 More recently, it was demonstrated that in cases of hypoperfusion, the accuracy of agreement between central laboratory and BGM readings may still result in undetected cases of hypoglycemia when a lower limit of 80 mg/dL is targeted. 26 We verified that similar perfusion problems can occur in hospitalized patients at significantly higher blood pressure variance. Therefore, BGMs that correlate with plasma glucose values measured by a reference method over a wide range of glucose concentrations and minimize the effects of hematocrit and blood pressure will allow better glycemic control for hospitalized patients with diabetes.
In contrast with several previous studies, 27 we tried to examine the performance of BGMs in the real hospital world, and the main focus of our study was to determine if an improvement in the analytical accuracy of BGMs would lead to improved clinical outcomes for hospitalized patients with diabetes. Regarding the precision and the accuracy of glucose monitoring in the hospital, the correlation between the glucose values obtained by the BGMs studied and the reference values obtained in the central laboratory ranged from 99% to 62%. More important is that almost 30% of the studied patients would have received different insulin dosages had the reference value been available at the same time as the BGM reading: in 5% of the patients the discrepancy resulted in symptomatic hypoglycemia. Therefore, the accuracy of BGMs in this study was relevant to treatment decisions, and a continuous quality control of the bedside monitoring of blood glucose levels is needed.
Asymptomatic hypoglycemia is frequent among hospitalized patients with diabetes; 28 inpatient hypoglycemia is especially dangerous since the symptoms may often go unrecognized because of, for example, an altered mental status. 29 Asymptomatic hypoglycemia was present in almost 30% of the patients studied with type 1 diabetes and in 20% of those with type 2 diabetes. In all cases, the BGMs were unreliable in sensing hypoglycemia. This is in accordance with the results of one recent study demonstrating that different BGMs have different accuracy in sensing hypoglycemia and that some are not accurate enough. 30 Thus our results further indicate that there is a need for the revision of the accuracy standards of current BGMs in hypoglycemia.
This study is not without limitations. Prior to the collection of blood samples and after the calibration procedure for new vials of strips, we were not able to perform quality control measurements for each BGM in daily clinical practice. Although it is recommended that quality control be performed daily in acute care settings, 31 this might have affected measurements performed. Moreover, the wide confidence intervals of the difference between some of the glucose meters results with the laboratory values during hyperglycemia imply less accuracy, and this should be considered in the management of the patients.
In conclusion, BGMs frequently used in hospital setting are not accurate enough in monitoring low and even higher blood glucose levels. Among hospitalized patients with diabetes, inaccurate glucose readings were most frequently falsely elevated, resulting in the misinterpretation of high glucose values or masking of true hypoglycemia. Patients and caregivers should be aware of these restrictions of the BGMs and be more prudent with insulin administration during hospitalization or at the emergency room to avoid overdosing and hypoglycemia. Finally, our results indicate that there is a further need for a revision of the accuracy and standards of BGMs, especially in low plasma glucose levels in the everyday hospital setting.
Footnotes
Author Disclosure Statement
No competing financial interests exist.