
Abstract
Objective:
This study compared the efficacy, safety, device satisfaction, and quality of life (QOL) in people with diabetes using an insulin bolus-patch versus current devices (pen/syringe) to deliver mealtime insulin.
Research Design and Methods:
Thirty-eight subjects with diabetes (26 with type 1 and 12 with type 2) were randomized to bolus-patch or current injection device (55% pen and 45% syringe) to deliver mealtime insulin in a multicenter, 6-week crossover study. Efficacy was assessed by equivalence in mean daily seven-point blood glucose (MDBG). Safety assessments included severe hypoglycemia episodes, adverse device effects (ADEs), and adverse events (AEs). Device satisfaction was determined by the validated Insulin Delivery System Rating Questionnaire (IDSRQ) and QOL by the validated Diabetes Specific QOL Scale (DSQOLS).
Results:
Using bolus-patch, MDBG (mean±SE) was equivalent to that using pen/syringe (8.61±0.28 vs. 9.02±0.26 mmol/L; P=0.098). SD of the seven-point blood glucose measurements was lower using bolus-patch (3.18±0.18 vs. 3.63±0.17 mmol/L; P=0.004), as was the coefficient of variation (CV) (37.2±1.7 vs. 40.3±1.7%; P=0.046). Hemoglobin A1c, 1,5-anhydroglucitol, fructosamine, and insulin use were similar between groups. There were no severe hypoglycemia episodes or serious ADEs. Between-device AEs were comparable. Subjects scored better on six of seven subscales on the DSQOLS and five of six subscales on the IDSRQ while using bolus-patch versus pen/syringe. At study completion, 76% of subjects would choose to switch to bolus-patch (P=0.001).
Conclusions:
Delivery of mealtime insulin with bolus-patch compared with pen/syringe resulted in equivalent MDBG, lower SD and CV of seven-point blood glucose measurements, good safety, significant device satisfaction, and improved QOL.
Introduction
The aim of this feasibility study was to compare efficacy, device satisfaction, and quality of life (QOL) in people with type 1 or 2 diabetes delivering mealtime insulin using a novel insulin bolus-patch (Finesse™, Calibra Medical, Inc., Redwood City, CA) versus current devices that deliver bolus insulin (pen/syringe). The insulin bolus-patch (henceforth referred to as bolus-patch) is classified as a new Food and Drug Administration product code, OPP, under 21 CFR 880.5725.
A preliminary report of the results of this study has been published in abstract form at the Tenth Annual Diabetes Technology Meeting, November 11–13, 2010, held in Bethesda, MD. 10
Research Design and Methods
The primary end point was to test the hypothesis that delivering mealtime insulin (Humalog® U 100 [Eli Lilly and Co., Indianapolis, IN] or NovoLog® U 100 [Novo Nordisk Pharmaceuticals Inc., Princeton, NJ]) using bolus-patch results in equivalent mean daily (seven-point) blood glucose (MDBG) as injecting the same insulin with current pen/syringe. All subjects injected their basal insulin using their current pen/syringe. A secondary end point was to test for superiority of MDBG once equivalence was established. Daily glucose profiles (average of three non-consecutive-day measures) were obtained using seven-point self-monitoring of blood glucose (SMBG), which included a preprandial (for each meal), 2-h postprandial (for each meal), and bedtime measurement. The SMBG was used to calculate glycemic variability indices SD, coefficient of variation (CV), M-value, 11 and mean amplitude of glycemic excursion (MAGE). 12 Additional secondary end points included HbA1c, 1,5-anhydroglucitol, fructosamine, and safety parameters including severe hypoglycemia episodes as defined by the Diabetes Control and Complication Trial, 13 adverse events (AEs), and adverse device effects (ADEs). Device satisfaction for insulin delivery and QOL were also secondary end points.
The design was a randomized, open-label, crossover study in five centers with a 1-week run-in period followed by a 12-week treatment period with clinic visits at baseline, 6-week crossover, and the study end at 12 weeks. Subjects conducted standardized SMBG testing during the run-in period on their current pen/syringe and then were randomized to use either bolus-patch for mealtime insulin delivery for 6 weeks or to continue with pen/syringe (pens provided) during Phase 1. After Phase 1, subjects crossed over to the alternate treatment for Phase 2. This design was chosen to gain comparative device data while eliminating potential confounding effects of time. Subject allocation to treatment order by site and type of diabetes was centralized and conducted by a remote online system to guard against potential selection bias (Simplified Clinical Data Systems, LLC, Milford, NH). Subjects were allowed to adjust their insulin depending on their blood glucose during the study as they would have prior to entering the study as prescribed by their physicians. Subjects gave written informed consent approved by local Institutional Review Boards. The study was conducted in accordance with the principles of the Declaration of Helsinki and of Good Clinical Practice.
Subjects
Adults with type 1 or 2 diabetes using a stable basal plus bolus insulin regimen (four or more injections per day) for at least 3 months were eligible for this study. Other inclusion criteria were 18–75 years of age, HbA1c 7.0–9.5%, stable oral medication for 3 months, and body mass index of ≤32 kg/m2. Exclusion criteria were unstable cardiac disease (medical history), abnormal hepatic (alanine or aspartate aminotransferase levels ≥2.5 times the upper limit) or renal (creatinine >265.2 μmol/L) function, evidence of gastroparesis (treatment with medication), current use of NPH insulin, regular insulin, pramlintide (Symlin®, Amylin Pharmaceuticals, San Diego, CA), or exenatide (Byetta®, Amylin Pharmaceuticals), use of continuous subcutaneous insulin infusion within the preceding 3 months, women who were pregnant or breast feeding, one or more severe hypoglycemia episodes as defined by the Diabetes Control and Complications Trial 13 during the preceding 6 months, and hypoglycemia unawareness (medical history).
Study treatments
The bolus-patch is small (65×35×8 mm) (Fig. 1A) and wearable for up to 3 days (Fig. 1B) and allows manual delivery of bolus insulin subcutaneously through a soft cannula. The bolus-patch is discreet for use in social situations (insulin can be dosed through clothing) without a portable digital accessory (Fig. 1C). The bolus-patch holds 200 units of insulin, administered in 1- or 2-unit increments by actuating the buttons (Fig. 1D). The bolus-patch requires 15–20 min of self-training or training by a healthcare provider.
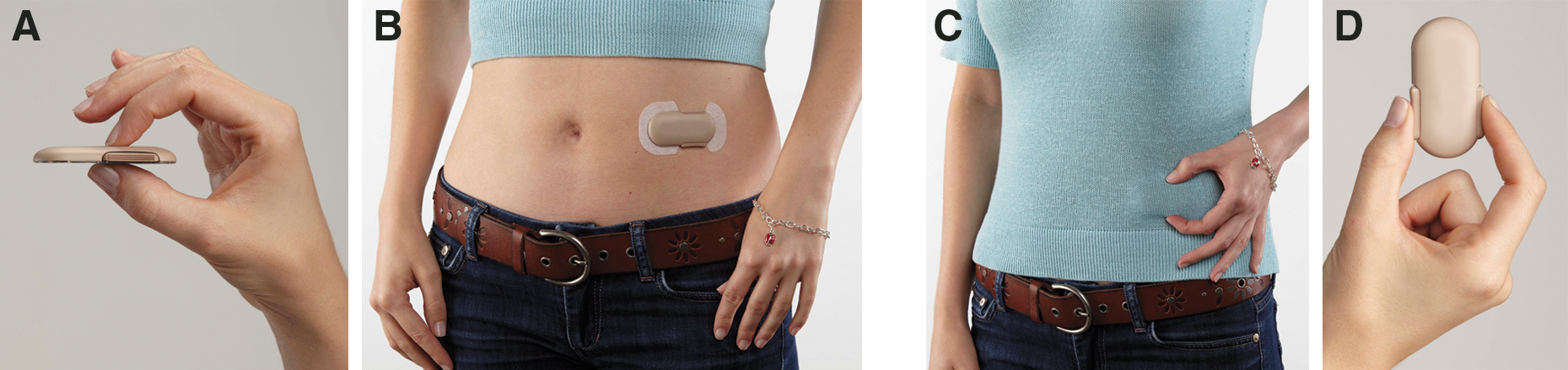
Insulin bolus-patch (Finesse, Calibra Medical Inc.). (
Subjects were instructed to perform SMBG daily per standard of care, to record insulin doses and SMBG (seven-point) for three non-consecutive days during run-in and the last week of Phases 1 and 2, and to record AEs, ADEs, and severe hypoglycemia episodes. Study supplies were provided and included glucose meters and consumables (lancets and test strips), insulin pens and consumables (needles), and vials of rapid-acting insulin. Healthcare providers completed insertion site reaction assessments for all devices.
Analytical measurements
Daily glucose was measured using a memory glucose meter (OneTouch® Ultra®2, Lifescan, Inc., Milpitas, CA) and was evaluated for non-severe biochemical hypoglycemia (glucose <3.89 mmol/L) and non-severe biochemical hyperglycemia (glucose >10 mmol/L). Laboratory tests (fasting plasma glucose, HbA1c, 1,5-anhydroglucitol, and fructosamine) were done by a central laboratory (Quest Diagnostics, Cincinnati, OH) at the end of phases 1 and 2. Subject satisfaction with insulin delivery was assessed by self-report on the validated Insulin Delivery System Rating Questionnaire (IDSRQ) 14 and QOL by the validated Diabetes Specific QOL Scale (DSQOLS). 15
Statistical methods
Pre-study power calculations using PASS version 2005 (Number Cruncher Statistical Systems, Kaysville, UT) determined that 28 completed subjects provided 90% power to detect equivalence (i.e., non-inferiority) for the primary end point of MDBG of bolus-patch compared with pen/syringe using a two-sided α level of 0.05, when the margin of equivalence for MDBG is 1.11 mmol/L, the true mean difference is 0.0, and the SD of the differences is 1.72 mmol/L. Equivalence will be established if the upper bound of the 95% confidence interval of the treatment difference for MDBG is below 1.11 mmol/L. For evaluating the subgroup of subjects with type 1 diabetes, 20 completed subjects would provide 78% power to detect equivalence for MDBG. A 2×2 crossover design with an equal number in each sequence was used for this estimate.
A secondary end point was to test for superiority of MDBG once equivalence was established. This was conducted at a two-sided α level of 0.05, and confidence intervals were calculated at 95%, two-sided. A two-period, two-treatment crossover analysis of variance model was used to compare devices for continuous measures. A subgroup analysis using the same crossover model was performed examining the interaction of treatment with the subgroups of diabetes type, injection device (pen vs. syringe), gender, and age (<65 vs. ≥65 years). For categorical measures, summary statistics including sample size, frequency, and percentages were performed by treatment. McNemar's test for paired responses was used for device comparisons. All analyses were implemented using SAS version 8.2 or higher (SAS Institute Inc., Cary, NC).
Results
Study population
Of 56 people screened for the study, 38 subjects with diabetes (26 with type 1 and 12 with type 2) were randomized to one of two sequence groups: bolus-patch followed by pen/syringe (19 patients) or pen/syringe followed by bolus-patch (19 patients). The 18 screen failures included 15 who did not meet the inclusion criteria for HbA1c, two who withdrew consent prior to randomization, and one with acute infection. Of 38 subjects randomized, 37 completed both phases of the study, and one was discontinued during Phase 2 because of hospitalization unrelated to the study device. All 38 randomized subjects comprised the intent-to-treat population and were included in all analyses. Six subjects had allowed protocol deviations at study entry including five with baseline body mass index >32 kg/m2 (32.2, 32.5, 35, 36.5, and 44.1 kg/m2) (results were maintained if these subjects were excluded) and one on a stable dose of lisinopril for 2 months instead of 3. Six subjects had allowed deviations during the study (three with follow-up dates outside the visit window and three with non-fasting clinic blood draws due to preceding hypoglycemia). Table 1 shows baseline characteristics of the 38 subjects in the intent-to-treat population according to randomized sequence group. Before entering the study, subjects in both sequence groups had similar daily insulin doses. During the study, insulin doses (mean±SE) remained within 10% of baseline and were similar for bolus-patch (total, basal, and mealtime, 60.4±4.5, 33.4±3.2, and 27.9±2.0 units/day, respectively) and pen/syringe (total, basal, and mealtime, 65.3±5.4, 37.7±4.7, and 28.4±1.9 units/day, respectively).
Data are mean±SD values. The insulin bolus-patch used was Finesse™ (Calibra Medical, Inc., Redwood City, CA). Humalog®, Lantus®, Levemir®, and NovoLog® are products of Eli Lilly and Co. (Indianapolis, IN), Sanofi-Aventis (Bridgewater, NJ), Novo Nordisk Pharmaceuticals Inc. (Princeton, NJ), and Novo Nordisk, respectively.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; HbA1c, glycated hemoglobin; Max, maximum; Min, minimum.
Glycemic control and variability indices
Indices are presented as mean±SE. Figure 2 displays MDBG at run-in and end point on the devices. The primary end point of equivalence of MDBG (in mmol/L) using bolus-patch (8.61±0.28) compared with pen/syringe (9.02±0.26) was met as the 95% upper confidence interval (mmol/L) of the treatment difference was within the upper equivalence margin of 1.11 (95% confidence interval, −0.97 to 0.16). For the subgroup of type 1 subjects, MDBG was also equivalent between bolus-patch (8.64±0.37) and pen/syringe (9.14±0.30) (95% confidence interval, −1.30 to 0.37). For secondary end points, there was a nonsignificant trend toward a lower MDBG by −0.42 using bolus-patch (P=0.098). The SD (mmol/L) of the seven-point blood glucose values was significantly (P=0.004) lower using bolus-patch (3.18±0.18) versus pen/syringe (3.63±0.17), as was the CV (bolus-patch vs. pen/syringe, 37.2±1.7% vs. 40.3±1.7%; P=0.046). The M-value also trended lower (P=0.097) using bolus-patch (368.4±40.5) versus pen/syringe (428.3±38.2). There was no difference in MAGE (in mmol/L) between devices (bolus-patch vs. pen/syringe, 5.66±0.41 vs. 6.11±0.37; P=0.396). The mean of premeal blood glucose values) also trended lower while using bolus-patch (bolus-patch vs. pen/syringe, 8.14±0.29 vs. 8.77±0.34 mmol/L; P=0.066). The mean of postmeal BG values was similar between devices (bolus-patch vs. pen/syringe, 8.84±0.34 vs. 9.30±0.31 mmol/L; P=0.234). There were no differences between devices for bedtime blood glucose values. HbA1c (bolus-patch vs. pen/syringe, 7.6±0.1% vs. 7.6±0.1%; P=0.944), 1,5-anhydroglucitol (bolus-patch vs. pen/syringe, 5.4±0.6 vs. 5.2±0.6 μg/mL; P=0.358), and fructosamine (bolus-patch vs. pen/syringe, 325.8±8.1 vs. 322.5±9.4 mmol/L; P=0.116) were similar between devices. Body weight during the study was stable (bolus-patch vs. pen/syringe, 87.1±2.4 vs. 87.2±2.4 kg). Secondary end points were maintained for the subgroup of type 1 subjects.
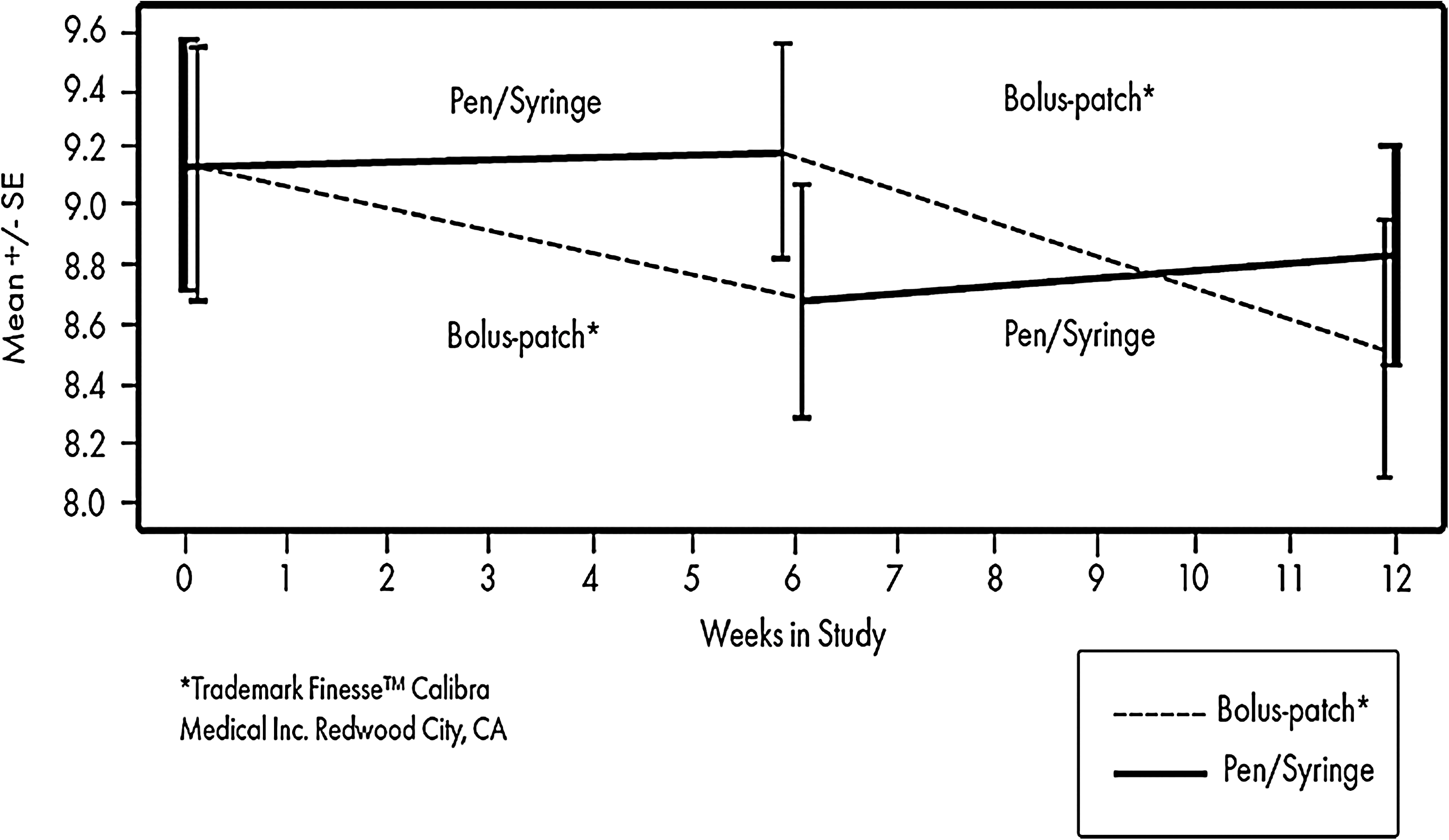
Mean daily blood glucose (in mmol/L) in 38 subjects (intent-to-treat population) by treatment sequence at baseline, the 6-week crossover (end of Phase 1), and the 12-week completion (end of Phase 2). Data are mean±SE values. The mean daily blood glucose was lower by −0.42 mmol/L using bolus-patch versus pen/syringe (P=0.098). *Bolus-patch is Finesse from Calibra Medical Inc.
There was no significant interaction by sequence (carryover effect) or period (Phase 1 vs. Phase 2) for any of the glycemic control measures. Subgroup analyses showed no interactions of MDBG (bolus-patch minus usual device) (mean; 95% confidence interval) (in mmol/L) by treatments for pen (0.01; −0.03, 0.05) compared with syringe (0.04; −0.00, 0.08) users, by gender for females (0.45; −0.39, 1.29) compared with males (0.30; −0.22, 1.02), and by age for age <65 years (0.02; −0.01, 0.05) compared with age ≥65 years (0.03; −0.03, 0.09).
Device satisfaction and quality of life
Subjects preferred bolus-patch over pen/syringe on five of six IDSRQ subscales (Table 2). At study completion, 76% of subjects wanted to switch from their pen/syringe to bolus-patch (P=0.001). Pen and syringe users equally preferred bolus-patch over injection, as did subjects with type 1 or type 2 diabetes. The treatment order did not impact preference as patients preferred bolus-patch whether they used it in Phase 1 or Phase 2.
Data are mean±standard deviation.
The answers on the Insulin Delivery System Rating Questionnaire (IDSRQ)14 and the Diabetes Specific Quality of Life Scale (DSQOLS)15 were scored on a scale of 0–100 to standardize as described in the original articles except for IDSRQ, Overall Satisfaction, which was on a scale of 1–4.
Higher score is better.
Lower score is better.
Subjects scored significantly better on six of seven subscales on DSQOLS while using bolus-patch versus pen/syringe (Table 2). The QOL for subjects improved while using bolus-patch for both pen and syringe users and for subjects with type 1 or 2 diabetes.
Safety profile
Eighteen AEs were reported during the study: one at baseline and 17 during the study. Eight AEs were reported during bolus-patch use, and nine during pen/syringe use. Eight of 38 subjects (21%) during bolus-patch use and eight of 37 subjects (22%) during pen/syringe use reported one or more AEs. The frequencies of the most common AEs were similar between treatments and included gastrointestinal disorders, infections, musculoskeletal and skin discomfort, and respiratory disorders. There were two serious AEs, both unrelated to the study devices: one during bolus-patch use (acute bronchitis) and one during pen/syringe use (acute pancreatitis with subject withdrawal for prolonged hospitalization). There were no serious ADEs for bolus-patch or pen/syringe. Insertion site reactions showed no differences between devices for irritation (erythema or papular reaction), edema, or ecchymosis.
There were no severe hypoglycemia or hyperglycemia episodes during the study. The incidence of non-severe biochemical hypoglycemia was similar for bolus-patch versus pen/syringe (34 of 38 subjects [89.5%] vs. 33 of 36 subjects [91.7%]; P=0.655). Non-severe biochemical hyperglycemia incidence was also similar for bolus-patch versus pen/syringe (37 of 38 subjects [97.4%] vs. 36 of 36 subjects [100%]; P=1.000).
Discussion
This feasibility study reports the first clinical use of a novel bolus-patch for patients prescribed a multiple daily injection insulin regimen. While using the bolus-patch, subjects had equivalent MDBG, less glycemic variability (SD and CV), improved device satisfaction, and better QOL compared with using their pen/syringe. Use of bolus-patch resulted in a safety profile that was similar to that of pen/syringe. All these findings suggest that the bolus-patch is a suitable alternative to current injection devices (pen/syringe) that deliver bolus insulin. Additionally, over a 3-day period, the bolus-patch required one skin penetration compared with nine skin penetrations with pen/syringe for administering bolus insulin.
That SD and CV (but not M-value and MAGE) only were significantly different with the bolus-patch may reflect the modest sample size of the study as the power calculation of the study was not based on glycemic variability. The study was powered to test the equivalence of MDBG but not powered to assess differences in glycemic control indices; it found no differences in HbA1c, 1,5-anhydroglucitol, and fructosamine between treatment groups. Nor was it powered to show device satisfaction by age, gender, or ethnicity. However, five of seven people over age 65 years preferred bolus-patch to injection.
Use of bolus-patch resulted in a safety profile that was similar to that of pen/syringe. AEs were similar between devices and were unrelated to the devices. Injection site reactions were not significantly different between devices and did not result in any subject withdrawing from the study. Incidence rates of non-severe biochemical hypoglycemia were similar between devices. The easier access to insulin with bolus-patch did not result in any severe hypoglycemia episodes. The similar incidence rates of non-severe biochemical hyperglycemia between devices suggest that subjects were able to easily use bolus-patch and had no problems with insulin delivery via a subcutaneous cannula. A safety feature on the bolus-patch alerts the patient if no insulin is delivered.
Other studies that compared pen versus syringe in adults with type 1 or 2 diabetes have shown patient preference for disposable pens but have not shown a change in glycemic indices versus the syringe. 16 –19 The present study showed a patient preference for bolus-patch over pen/syringe without a difference in glycemic control indices. The pen offers the convenience of having a prefilled insulin delivery device but still requires multiple daily injections and does not offer the ease of use and discreetness of the wearable bolus-patch. Although not intended to replace traditional pumps, the bolus-patch offers some of the pump advantages, including users have bolus insulin with them all the time, can discreetly dose bolus insulin in social situations, and only have to penetrate the skin once every 3 days for bolus dosing [they still need to give basal injection(s) daily]. The bolus-patch also has advantages over traditional pumps in that pumps are much higher in cost 20 and more complex to use. 21 However, the bolus-patch does not have the basal insulin infusion that traditional pumps have.
This feasibility study has limitations. Mealtime carbohydrate intake was not available to assess appropriateness of insulin dose during treatments. The limited days of diary recordings did not show differences in bolus insulin usage between devices. The short duration of the study precludes comments on longer-term outcomes.
In conclusion, bolus-patch offers the safety and efficacy of insulin administration by pen/syringe without multiple daily injections. Bolus-patch also allowed subjects greater ease in delivering bolus insulin and improved their QOL. The results of this study encourage larger and longer-term studies to evaluate if using the bolus-patch allows patients to more consistently cover meals and snacks as recommended by their clinical team compared with pen/syringe.
Footnotes
Acknowledgments
N.B., R.L.B., D.D., and M.T. wrote and edited the manuscript. R.B., R.C., M.M., P.R., and F.W. reviewed/edited the manuscript and contributed to the discussion. D.K., S.L., and E.M. reviewed/edited the manuscript and researched data. H.R. and S.S. researched data. We thank Vivien Zraick, M.S., Calibra Medical, Inc. (Redwood City, CA), for study management support, Kristin Hardymon, B2S Consulting (Carmel, IN), for data management support, and Nancy Yeh, Anaclim, LLC (Indianapolis, IN), for data monitoring support. The study was supported by Calibra Medical, Inc., the manufacturer of the Finesse Insulin Bolus-Patch.
Author Disclosure Statement
R.L.B., D.K., and M.T. have received consulting fees from Calibra Medical, Inc., and M.T. has ownership of equity. D.D. is an employee of Calibra Medical, Inc. and has ownership of equity. No other competing financial interests relevant to this article were reported.