
Abstract
Background:
We evaluated how a structured patient/physician self-monitoring of blood glucose (SMBG) intervention influenced the timing, frequency, and effectiveness of primary care physicians' treatment changes with type 2 diabetes mellitus (T2DM) patients over 12 months.
Methods:
The Structured Testing Program (STeP) study was a cluster-randomized, multicenter trial with 483 poorly controlled, insulin-naive T2DM subjects. Primary care practices were randomized to the Active Control Group (ACG) or the Structured Testing Group (STG), the latter of which included quarterly review of structured SMBG results. STG patients used a paper tool that graphs seven-point glucose profiles over 3 consecutive days; physicians received a treatment algorithm based on SMBG patterns. Impact of structured SMBG on physician treatment modification recommendations (TMRs) and glycemic outcomes was examined.
Results:
More STG than ACG patients received a TMR at each study visit (P < 0.0001). Of patients who received at least one TMR, STG patients demonstrated a greater reduction in glycated hemoglobin A1c (HbA1c) than ACG patients (−1.2% vs. −0.8%, P < 0.03). Patients with a baseline HbA1c ≥8.5% who received a TMR at the Month 1 visit experienced greater reductions in HbA1c (P = 0.002) than patients without an initial TMR. More STG than ACG patients were started on incretins (P < 0.01) and on thiazolidinediones (P = 0.004). The number of visits with a TMR was unrelated to HbA1c change over time.
Conclusions:
Patient-provided SMBG data contribute to glycemic improvement when blood glucose patterns are easy to detect, and well-trained physicians take timely action. Collaborative use of structured SMBG data leads to earlier, more frequent, and more effective TMRs for poorly controlled, non–insulin-treated T2DM subjects.
Introduction
While the focus has primarily been on how often patients test (or fail to test), we suspect that a critical, and often unexamined, factor is the role of the primary care physician. A key value of SMBG is that it can provide physicians with the data they need to make timely and effective adjustments in medication and critical lifestyle recommendations. 19 In recent SMBG intervention studies where patients collected and recorded SMBG data but the patient's physician had limited or no access to the accumulated findings, no significant improvement in glycated hemoglobin A1c (HbA1c) occurred. 16,17 In contrast, in those studies that did provide physicians with SMBG data, as a vehicle to monitor and adjust therapy, significant glycemic improvement was observed. 13 –15
It also has been well documented that many physicians do not intensify diabetes therapies in a timely manner in patients who are above their recommended glycemic targets. 20 –24 For example, one recent prospective, multicenter study revealed that most insulin treatment was initiated only after HbA1c levels were ≥9.6% (±1.8%) for a sustained period of time. 25 In a recent pilot study, we showed that when primary care physicians are presented with structured, easy-to-visualize SMBG data, they recommended more timely and aggressive treatment changes. 26 Therefore, well-structured SMBG data may prompt primary care physicians to intervene earlier, more frequently, and more effectively to improve glycemic control than if no such data were available.
To explore this hypothesis, we examined data from the Structured Testing Program (STeP) study, a 12-month, cluster-randomized, multicenter clinical trial in primary care to evaluate whether poorly controlled (HbA1c ≥7.5%), insulin-naive T2DM patients would benefit from a comprehensive, integrated physician/patient intervention utilizing a structured data collection form that enabled patients to record and plot a seven-point SMBG profile on 3 consecutive days. 15 The experimental arm of the study required that both physicians and patients participate in a collaborative program to gather, interpret, and act upon the structured SMBG data, at quarterly intervals, to make treatment modifications. 15 At 12 months, there were significantly greater reductions in mean HbA1c in experimental group patients compared with control group patients (P = 0.04). 15 In addition, we found that experimental patients received treatment modification recommendations (TMRs) from their physicians (life-style and/or medication) significantly more often over the 12 months than control patients (P < 0.0001). 15 We also reported that patients in both study groups who received a TMR at the initial visit evidenced significantly greater glycemic improvement than those who did not receive an initial TMR, suggesting that early intervention yielded the best glycemic outcomes and that significantly more experimental than control patients received a TMR at the Month 1 visit (P < 0.0001). 15
For the current study, we sought to determine in more detail how the structured SMBG protocol influenced physician behaviors regarding the timing and effectiveness of TMRs during the study and, if so, whether these treatment recommendations were related to improved glycemic control.
Research Design and Methods
Participants
Details of the STeP study design and intervention have been presented elsewhere. 15,27 In brief, patients were recruited from 34 primary care practice sites across the eastern United States. Each practice generated a list of all patients who met inclusion criteria from their patient databases. Patients were then randomly selected from the list, using an external, study-defined protocol until the predetermined sample size was reached. The study protocol was approved by the Copernicus Group (central institutional review board) and is in compliance with the Declaration of Helsinki. 28
Inclusion criteria were as follows: T2DM for more than 1 year; age ≥25 years; HbA1c level ≥7.5% to <12.0%; currently treated by diet, exercise, oral diabetes medication, and/or injectable incretin mimetic; able to read and write English; and had not participated in any other research protocol within the last 30 days. Exclusion criteria were as follows: C-peptide level ≤0.50 ng/mL; used systemic oral or inhaled steroids for more than 14 days within the last 3 months; treated with chemotherapy or radiation therapy; pregnant or breast feeding; or had a severe psychological condition.
Recruitment and informed consent
The first patient entered the study in April 2008; the last patient completed follow-up in February 2010. Practices—not patients—were randomized to the intervention or control conditions (described below), based on a predetermined stratification system to assure a balance across practice size, urban–rural location, and case mix. Eligible patients were contacted by mail or phone by their primary care office and invited to attend a screening visit. At screening, the study was described, written informed consent was obtained, and relevant medical information was recorded. At a baseline visit (within 14 days), patients in both arms received a free blood glucose meter and test strips (Accu-Chek® Aviva meter system, Roche Diagnostics, Indianapolis, IN) and were instructed in their use. At all subsequent visits, clinic staff collected laboratory samples and recorded TMRs. All patients brought their meters to each visit so that data could be uploaded electronically.
Interventions
Structured Testing Group (STG) participants were trained with the Accu-Chek 360° View blood glucose analysis system (Roche Diagnostics), which enabled patients to record and plot a seven-point SMBG profile, on each of 3 consecutive days prior to each clinic visit. They were trained to interpret their SMBG results and to modify food intake and activity level based on the findings. Patients were instructed to bring their completed tool to each clinic visit. Active Control Group (ACG) subjects did not receive the tool or any additional SMBG training.
STG physicians received training on interpreting the SMBG data recorded on the tool and were provided an algorithm that described various pharmacologic/life-style treatment strategies to remediate problematic blood glucose patterns (STeP Study tools and resources are available at
Measures
TMRs were calculated using information entered into patient records at each clinic visit. These included recommended pharmacologic modification (initiation of a new medication, increase/decrease in the dose of an existing medication, and/or termination of an existing medication) and recommended life-style modification (defined as any change in diet, exercise, or other self-care behavior). The total number of visits with a TMR, time to first TMR, and quarterly HbA1c were recorded for all patients.
Statistical analyses
Between-group differences in the proportion of patients with a TMR at each scheduled visit were tested using Fisher's Exact Test. The number of scheduled visits with a TMR was compared between study groups using a two-sample t test. The differences between study groups in the proportions of patients who were recommended a particular class of medication were tested using Fisher's Exact Test. A Generalized Linear Mixed Models (GLMM) with SAS %GLIMMIX Macro 29 was used to evaluate the main and interaction effects of patients' baseline HbA1c (<8.5% and ≥8.5%), body mass index, duration of diabetes, and patient demographics on the proportion of scheduled visits with a TMR. A Linear Mixed Models (LMM) with SAS PROC MIXED 30 was used to assess the number of scheduled visits with a TMR.
The association between a TMR at the Month 1 visit and change in HbA1c was investigated using a similar LMM analysis. Change in HbA1c was the dependent variable, and TMR at Month 1 (yes/no) and baseline HbA1c were included as predictor variables, along with other controls. Interaction effects of TMR by study group and baseline HbA1c also were tested. All analyses included the intent-to-treat population, defined as all subjects who completed baseline and at least one other study visit.
Results
Enrollment and sample characteristics
We recruited 34 primary care practices and randomized them to ACG (n = 13) or STG (n = 21). More STG than ACG sites were recruited because of an expected higher attrition among STG than ACG patients over time.
Of the 770 patients screened, 287 failed to meet inclusion/exclusion criteria or did not attend the baseline (training) visit, leaving 483 eligible patients (ACG, 227 patients; STG, 256 patients). By 12 months, 40 (17.6%) ACG patients and 68 (26.6%) STG patients had dropped out, yielding a combined attrition of 108 (22.4%) patients. Of note is that there was no significant difference in the dropout rate between the STG and ACG groups (P = 0.15). Dropouts in both groups were slightly younger (P < 0.02) and more likely to be African American (P < 0.02), had a higher HbA1c at baseline (P < 0.01), and had fewer co-morbid conditions at baseline (P < 0.02). Between-group demographic and disease-related characteristics at baseline differed only by age and ethnicity (Table 1). The sample included 227 patients and 13 physicians in the ACG and 256 patients and 21 physicians in the STG.
Values are numbers (percentages) unless stated otherwise.
BMI, body mass index; HbA1c, glycated hemoglobin A1c.
Timing and frequency of physician TMRs
Significantly more STG than ACG patients received a TMR at each quarterly visit (P < 0.0001), regardless of patients' baseline HbA1c, body mass index, duration of diabetes, and patient demographics (Fig. 1A). Of those who completed the study, only 10 STG patients (5%) did not receive a TMR across the 12 months, whereas 66 ACG patients (35%) did not receive a TMR. There was no significant difference in baseline HbA1c between STG patients who did (8.9 ± 1.1%) versus those who did not (8.9 ± 1.0%) receive a TMR over the 12 months (P = 0.9); in contrast, baseline HbA1c was significantly higher in ACG patients who received at least one TMR over the 12 months (9.0% ± 1.2%) versus those ACG patients who did not (8.4 ± 0.8%) (P < 0.0001).
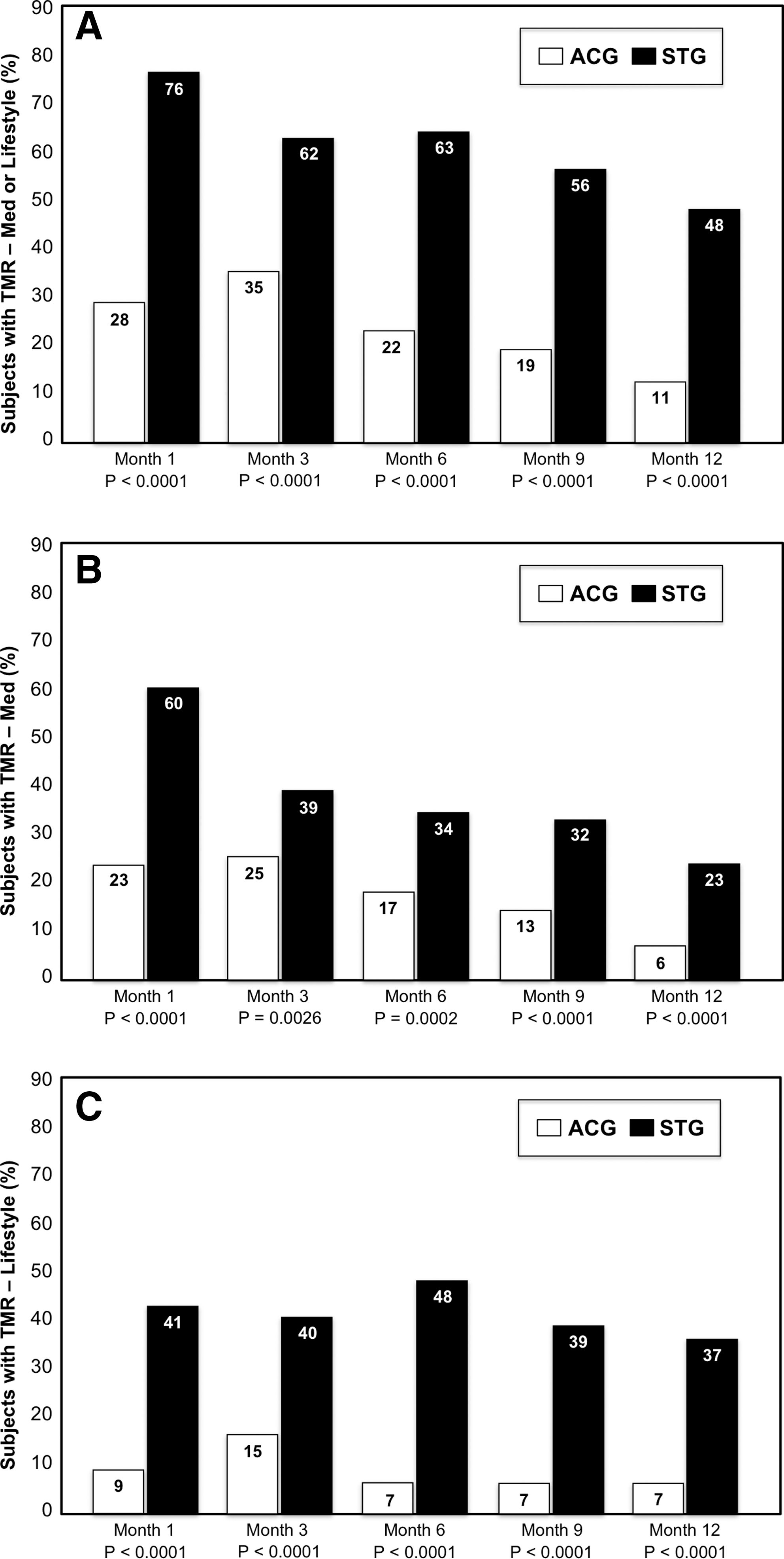
Percentages of patients who received a treatment modification recommendation (TMR) by study visit: (
When medication and life-style TMRs were examined separately, we again found that STG patients received significantly more of each at each quarterly visit (Fig. 1B and C). Over the 12 months, more STG than ACG patients received at least one medication and at least one life-style change recommendation (STG, 57%; ACG, 31% [P < 0.0001]). Of note is that STG patients were started significantly more often than ACG patients on incretins (glucagon-like peptide-1 agonists or dipeptidyl peptidase-4 inhibitors) (22% vs. 13% [P < 0.01]) and on thiazolidinediones (23% vs. 12% [P = 0.004]).
Impact of physician TMRs
Because early intervention and persistent titration of treatment are keys to preventing long-term complications, we explored both the timing and frequency of TMRs by physicians. We first compared changes in HbA1c between the subsample of STG patients (n = 222) and ACG patients (n = 137) who received at least one TMR during the 12 months; STG patients who received a TMR demonstrated a significantly greater reduction in HbA1c than ACG patients who received a TMR (STG, −1.2%; ACG, −0.8%; ΔHbA1c, −0.4% [P < 0.03]).
Previously, we reported that patients in both study groups who received a TMR at the initial visit evidenced significantly greater glycemic improvement than those who did not receive an initial TMR, suggesting that early intervention yielded the best glycemic outcomes. 15 Further investigation, however, revealed a significant interaction with baseline HbA1c, indicating that initial TMR was associated with greater glycemic improvement only for those patients with baseline HbA1c ≥8.5% (mean HbA1c change, −1.8% vs. −1.3% [P = 0.002]). There were no significant differences in glycemic improvement between those who did and did not receive an initial TMR among those patients with a baseline HbA1c <8.5%. As noted above, however, far more STG patients received a TMR at the first study visit than ACG patients. Finally, there was no significant association between the total number of visits with a TMR and glycemic change over the study period.
Conclusions
We find that the routine availability of structured SMBG data for knowledgeable physicians in primary care leads to earlier, more frequent, and more effective interventions to improve glycemic control, compared with settings in which only limited, unstructured, or unsystematic SMBG data are available. The current findings point to the critical role of the engaged and well-informed physician in this process. The STeP intervention involved patients who were willing and able to collect SMBG data in an intensive, structured manner and to share these data with their physician and physicians who were trained to interpret and respond to such data in targeted ways. Our findings suggest that this patient/physician collaboration led physicians to recommend earlier and more effective TMRs, both medication and life-style, than physicians in the control condition.
We also find that early TMRs are associated with significantly greater glycemic improvement than later TMRs, especially in patients with the poorest glycemic control at baseline. This is important because significantly more STG patients received a TMR at the first study visit, and at all subsequent visits, than ACG patients. As we reported previously, the total number of visits in which a TMR occurred was three times greater among STG patients than ACG patients. 15 Furthermore, almost all STG patients (95%) received at least one TMR over the 12 months, compared with only two-thirds of ACG patients. ACG physicians were seemingly influenced by baseline HbA1c (those patients who received at least one TMR had significantly higher HbA1c values than those who did not receive one), whereas STG physicians chose to initiate at least one TMR across the entire range of (elevated) baseline HbA1c. In total, the increased frequency and timeliness of the interventions by STG physicians suggest that our structured testing protocol may have countered at least some of the negative clinical effects of “treatment inertia,” whereby aggressive interventions are often delayed for long periods of time, even in patient samples (similar to ours) where poor glycemic control is common.
These data also suggest that an STG physician-initiated TMR, based in large part on patient-provided SMBG data, is more effective in improving glycemic control than a TMR initiated by an ACG physician who does not have structured SMBG data available. STG patients were more likely to receive both types of TMRs, medication and life-style, than ACG patients. STG patients were also more likely than ACG patients to be started on incretins, thiazolidinediones, and—as was reported in our previous publication—intermediate and long-acting insulins. 15 This suggests that STG physicians made broader use of intervention options than ACG physicians. There was no relationship between the number of visits with a TMR and glycemic improvement in either study group, indicating that more TMRs do not necessarily lead to better glycemic outcomes. Thus, these findings point to the importance of TMR quality and suggest that STG physicians made better choices in the selection of available diabetes therapies and in their recommendations to patients. We suspect that this was the result of the training and resource materials provided in combination with the availability of structured, episodic SMBG data presented in a format that enabled physicians to easily identify, interpret, and act upon significant blood glucose patterns.
Our findings shed new light on why SMBG interventions in non–insulin-using T2DM have been shown to be efficacious in some trials, but not in others. 9 –15 For example, in current practice, non–insulin-treated patients are able to make only partial use of SMBG data on their own (i.e., changes in diet and activity level). Without the active involvement of their physicians or other healthcare professionals who actually use the SMBG data to initiate and adjust pharmacologic treatment, the clinical benefits of SMBG data most likely will be limited, as was found in some previous studies. 16 –18
Several limitations are noteworthy. First, the study did not include a third study arm that would have assessed the effect of increased attention paid to both study groups over the 12-month period; thus, we believe that the enhanced usual care received by ACG resulted in a very conservative estimate of between-group differences. Second, as discussed previously, we could not determine if the treatment changes initiated by physicians and patients were clinically appropriate; our measures examined the occurrence and number of TMRs, rather than the appropriateness of the TMR recommended. We note, however, that TMRs offered by STG physicians were more effective in improving glycemic control than TMRs offered by ACG physicians. Third, we could not determine how many of the recommended treatment changes actually occurred (i.e., whether or not patients actually followed through with treatment recommendations) or whether patients may have initiated treatment changes on their own, perhaps in the absence of a physician TMR.
In conclusion, our findings suggest that physicians can effectively utilize structured, episodic, patient-collected SMBG data in ways that significantly improve glycemic control. SMBG is a tool that can contribute to positive clinical outcomes, but only when the resulting data are used to inform appropriate treatment changes.
Footnotes
Acknowledgments
Funding for the study was provided by Roche Diagnostics, Indianapolis, IN.
Author Disclosure Statement
W.H.P. has received consulting fees from Roche Diagnostics and Abbott Diabetes Care. L.F. has received consulting fees from Roche Diagnostics. C.H.S. has received consulting fees from Roche Diagnostics. D.A.H. has received consulting fees from Roche Diagnostics and Abbott Diabetes Care. C.G.P. has received consulting fees from Roche Diagnostics and Abbott Diabetes Care. Z.J. has received consulting fees from Roche Diagnostics. M.A.-S., B.P., and R.S.W. are employed by Roche Diagnostics.
This study is registered at ClinicalTrials.gov with identification number NCT00674986.
Parts of this study were presented in poster form at the 69th Scientific Sessions of the American Diabetes Association, New Orleans, Louisiana, June 5–9, 2009, the 70th Scientific Sessions of the American Diabetes Association, Orlando, Florida, June 25–29, 2010, and the 45th Meeting of the European Association for the Study of Diabetes, Stockholm, Sweden, September 20–24, 2010.