
Abstract
Background:
Diarrhea, constipation, flatulence, and abdominal pain are common complaints in type 2 diabetes patients. Impaired intestinal motility is often followed by small intestinal bacterial overgrowth (SIBO). Therefore, this study was planned to determine the incidence of SIBO and its relation with orocecal transit time (OCTT) in type 2 diabetes patients.
Subjects and Methods:
SIBO and OCTT were measured by using noninvasive glucose and lactulose hydrogen breath tests, respectively. For this study, 84 patients with type 2 diabetes mellitus in the age range 30–65 years and 45 age-matched apparently healthy controls were enrolled.
Results:
The glucose hydrogen breath test was suggestive of SIBO in 15.5% of patients with type 2 diabetes mellitus but in one (2.2%) of controls. There was a significant increase (P<0.001) in OCTT in type 2 diabetes patients compared with controls. It was also observed that OCTT in type 2 diabetes patients with SIBO was significantly delayed (P<0.001) compared with type 2 diabetes patients without SIBO.
Conclusion:
This study indicates that SIBO in diabetes patients may be due to delayed OCTT.
Introduction
Optimal bowel cleansing is poorer in diabetes patients with autonomous neuropathy than in those without autonomous neuropathy and in controls. 3 It is well known that abdominal discomfort, flatulence, nausea, vomiting, constipation, and diarrhea are more common in diabetes patients than in the general population. 4 The pathogenesis is unclear. Multiple factors like hyperglycemia and the motility disturbances resulting from diabetic autonomous neuropathy are probably responsible for these symptoms. 5 Diabetic autonomous neuropathy is a debilitating complication of diabetes mellitus. It impairs quality of life and can be clinical or subclinical depending upon the presence or absence of symptoms. 6,7 Delayed gastric emptying and disturbance of intestinal motility are frequent findings in diabetes patients. 8 –10 Impaired intestinal motility is often followed by small intestinal bacterial overgrowth (SIBO), which can possibly lead to deconjugation of bile acids, diarrhea, steatorrhea, malabsorption of vitamins and/or micronutrients, weight loss, mucosal injury, bacterial translocation, and worsening of small bowel motility. 11 However, patients in whom bacterial overgrowth is found may also be asymptomatic. 12
Until now, little attention has been devoted to the relationship among autonomous neuropathy, impaired intestinal motility, and SIBO in diabetes patients. 11,13,14 However, there is not a single study in the literature from north India on this subject. Therefore, the present study was planned to evaluate the incidence of SIBO and orocecal transit time (OCTT) by using noninvasive glucose and lactulose hydrogen breath tests, respectively, in type 2 diabetes patients from North India.
Subjects and Methods
This is a prospective study. A total of 127 subjects were enrolled for this study. Forty-three patients were excluded according to exclusion criteria. Two groups of subjects were enrolled: the study group and controls.
Study group
Eighty-four type 2 diabetes patients between the age of 30 to 62 years, attending the Diabetic and Gastroenterology Clinics of the Postgraduate Institute, Chandigarh, India, were enrolled between January 2006 and December 2009 for this study. Duration of diabetes was >5 years. These patients had chronic diarrhea (more than three loose stools per day) since at least 3 weeks before the test. The subjects' demographic characteristics are given in Table 1. The Institute's Ethical Committee approved this study before the work was started.
Data are mean±SD values.
Exclusion criteria
The following exclusion criteria were applied: (1) patients with prior gastric surgery/vagotomy; (2) history of peptic ulcer and therapy with H2 antagonist/proton pump inhibitors; (3) patients with history of corrosive injury, systemic sclerosis, liver cirrhosis, hypothyroidism, intestinal pseudo-obstruction, blind-loop syndrome, small intestinal bypass, duodenal and massive duodenojejunal diverticulosis, or chronic infection of main bile duct; (4) patients who had received broad-spectrum antibiotics during the month preceding the test (which may influence the results of the hydrogen breath test, making it false-negative); (5) those who had taken drugs that are known to interfere with gastrointestinal motility (such as anticholinergics or antidepressants); (6) colonoscopy within 1 week before the hydrogen breath test; (7) patients treated with metformin (which can cause diarrhea); (8) positive stool examination for parasitic infection; and (9) patients with celiac disease, pancreatic insufficiency, anorectal dysfunction, strictures, web, or diverticula.
Controls
Forty-five age-matched apparently healthy relatives of patients were enrolled as controls. Their blood sugar was normal, and they had not taken any antibiotics for 1 month preceding the hydrogen breath test. They were also not taking drugs that are known to interfere with gastrointestinal motility (such as anticholinergics or antidepressants). They also did not have a history of gastric surgery/vagotomy, peptic ulcer, and therapy with H2 antagonist/proton pump inhibitors.
Procedures
The details of the study were explained to both the groups (subjects and controls), and informed consent was obtained. Type 2 diabetes mellitus was diagnosed in all subjects according to the World Health Organization criterion (any individual with two fasting plasma glucose levels of 126 mg/dL or greater). All patients in the present study had two fasting values of >126 mg/dL, postprandial glucose of >145 mg/dL, and hemoglobin A1c percentage of >6.0%.
A detailed history was obtained, and a physical examination was done for all patients.
In all subjects, endoscopic assessment of gastrointestinal transit was done for the presence of any peptic ulcer and gastric or esophageal obstruction.
All patients with type 2 diabetes received standard treatment and had good glucose control at the time of study.
Glucose hydrogen breath test for SIBO
Patients were instructed to eat a low fiber diet 3 days before the glucose hydrogen breath test. They were given 80 g of glucose in 200 mL of water to drink after taking a basal end expiratory breath. 15 Then breath samples were collected at 15-min intervals for 2 h. Breath hydrogen (H2) and methane (CH4) concentrations were measured by gas chromatography using an SC MicroLyzer™ (QuinTron Instrument Co., Milwaukee, WI). An increase in breath H2 and/or CH4 concentration >12 ppm over baseline value in two consecutive readings was defined as SIBO.
Lactulose hydrogen breath test for OCTT
OCTT was measured by using 15 mL of lactulose syrup containing 10 g of lactulose. 16 Patients were asked to give an end expiratory breath after a 12-h fast. They were also advised not to consume a high fiber diet 3 days before the test because these foods may cause prolonged excretion of hydrogen gas and a high fasting value. Cigarette smoking and exercise were not allowed for at least 2 h before and during the test. End expiratory breath samples were taken after every 15 min up to 3 h. Samples were analyzed by the QuinTron Micro H2 breath analyzer. Time taken for the rise to >12 ppm over the baseline value was taken as the OCTT.
Statistical analysis
Results were expressed as mean±SD and percentage. The χ2 test was used to analyze the presence of SIBO in both the groups. Student's unpaired t test was applied to compare the OCTT between the study and control groups and between SIBO-positive and -negative type 2 diabetes mellitus patients. All statistical analyses were performed by using SPSS version 16.0 for Windows (SPSS, Inc., Chicago, IL). Regression analysis for independent determinants of SIBO was done.
Results
The study population from North India consisted of 84 patients (33 women and 51 men) with a mean±SD age of 40.5±12.6 years (range, 30–62 years). The control group consisted of 45 subjects (16 women and 29 men) with a mean±SD age of 43.4±13.8 years (range, 32–65 years). Age and sex ratio did not differ between the two groups (Table 1).
SIBO was observed in 13 of 84 (15.5%) type 2 diabetes patients but in only one (2.2%) of the control subjects. The difference was statistically significant (P<0.05) (Table 2). The mean hydrogen concentration in diabetes patients grouped on the basis of glucose hydrogen breath test at different time intervals is shown in Figure 1.
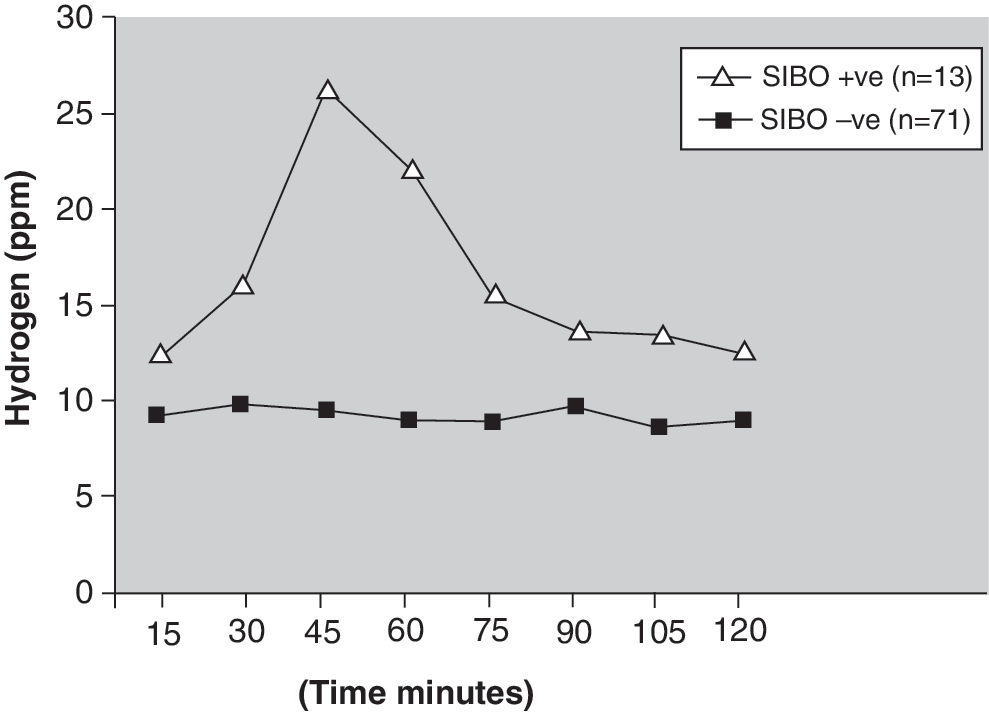
Mean hydrogen concentrations of small intestine bacterial overgrowth (SIBO)−positive and −negative type 2 diabetes patients at different time intervals.
P<0.05 between patients and controls.
H2BT, hydrogen breath test.
For 84 patients with type 2 diabetes mellitus, OCTT was >90 min in 75 (82.1%), whereas in nine (17.9%) OCTT was <90 min. In contrast, for 45 controls, only five (11.1%) had OCTT >90 min, and 40 (88.9%) had <90 min (Table 3). In this group of North Indian diabetes patients, mean±SD of OCTT was 138.93±40.4 min, whereas it was 90±14.67 min in controls. There was a statistically significant increase (P<0.001) in OCTT in type 2 diabetes patients compared with controls (Fig. 2). This difference was similar in male as well as female patients: mean±SD values of OCTT in men with diabetes was 139.7±44.8 min, whereas in women it was 133.6±35.4 min. SIBO was observed in 13 of the 84 (15.5%) type 2 diabetes patients, and in all these patients OCTT was delayed by >90 min; in another 62 diabetes patients also, the OCTT was delayed (>90 min), but there was no SIBO in these patients (Table 4). Of the 13 patients with SIBO, six were men (46.2%), and seven were women (53.8%). This difference was not statistically significant.

Orocecal transit time (OCTT) in type 2 diabetes mellitus (T2DM) patients (Pts), controls, and T2DM Pts with and without small intestine bacterial overgrowth (SIBO).
P<0.001 between patients and controls.
OCTT, orocecal transit time; SIBO, small intestine bacterial overgrowth.
Mean±SD OCTT in SIBO-positive diabetes patients was 192.7±40.4 min, whereas in SIBO-negative diabetes patients it was 129.1±34.9 min (Fig. 2). The difference was statistically significant (P<0.001). No significant difference was observed in any other parameter like age, fasting blood sugar, hemoglobin A1c, body mass index, or duration of diabetes (years) between SIBO-positive and SIBO-negative type 2 diabetes patients (Table 5). In the multivariate linear regression analysis model that explained 0.361% (adjusted multiple R 2 =0.312) of the variation in SIBO, the independent determinant was only OCTT (P≤0.001) (Table 6).
Grouping variable was small intestinal bacterial overgrowth.
P<0.001, orocecal transit time (OCTT) was significantly increased in small intestinal bacterial overgrowth−positive type 2 diabetes mellitus patients.
BMI, body mass index; FBS, fasting blood sugar; HbA1c, hemoglobin A1c.
Adjusted multiple R 2=0.312.
BMI, body mass index; FBS, fasting blood sugar; HbA1c, hemoglobin A1c; OCTT, orocecal transit time.
Discussion
Several mechanisms have been proposed to explain the structural and functional abnormalities associated with diarrhea in diabetes. 17,18 Autonomous neuropathy and SIBO appear to be two major contributing factors, but patients with autonomous neuropathy were excluded from this study. The role of SIBO in diarrhea in diabetes was suggested for the first time in 1957 by Malins and French. 19 The incidence of SIBO has been reported in the literature from other countries to be less than 20%. 17,20,21 Our study in North India showed that the incidence of SIBO was present in approximately the same number of patients with type 2 diabetes mellitus (i.e.,15.5%). Direct evidence of SIBO by jejunal aspiration is the reference method 22 for the diagnosis of SIBO. However, the chance of contamination is high while taking out the jejunal aspirate, and the method is invasive.
Major progress has been made with hydrogen breath testing, which can now evaluate intestinal transit time with lactulose or intestinal permeability with mannitol or detect SIBO with glucose. 23,24 The glucose hydrogen breath test is a useful test because it is easy to perform, noninvasive, and inexpensive, and its diagnostic value is high. 16 The present study provides the evidence for an association between SIBO and OCTT in Indian type 2 diabetes patients.
It is difficult to investigate transit time through the small intestine, and studies in diabetes have been few. 25 To the best of our knowledge, this is the first study in Indian type 2 diabetes patients that demonstrates delayed OCTT, a greater risk of SIBO, and an associated greater risk of diarrhea and gas-related symptoms. The findings of radiological studies showed contradictory results about the OCTT, with some reporting an increased transit time, whereas others have shown a decrease in OCTT. 26 Use of the breath hydrogen test provides a simple method of estimating the transit time of a bolus of fluid through the small intestine. The rise in the amount of breath hydrogen, observed when non-absorbed carbohydrate reaches the colonic bacteria, is easily measured. Reproducibility in this series was good, and our results for normal controls were similar to those of Bond and Levitt. 27 OCTT was >90 min in 75 of the 84 (82%) diabetes patients compared with only 17.9% of the controls. However, SIBO was present only in 13 of these 75 diabetes patients. These 13 patients had a longer duration of diabetes mellitus. These results support the concept that small intestinal transit is delayed in diabetes. This may be because of initial changes in the gastrointestinal tract due to type 2 diabetes mellitus. Slow intestinal transit could allow bacteria to proliferate in the lumen, and this seems to explain diarrhea in some people with diabetes. 23 In the present study, it was also observed on multivariate analysis that there was no significant relation between age, hemoglobin A1c, and fasting blood sugar level (except OCTT) in type 2 diabetes patients who had SIBO. Although OCTT was delayed in 82% of the type 2 diabetes patients, it was more delayed in SIBO-positive patients than in SIBO-negative patients.
We would speculate that type 2 diabetes patients with bacterial overgrowth have even more sluggish small intestinal transit than patients with only type 2 diabetes, but we cannot prove this with the present study. These findings are in contrast with those studies in which investigators failed to show any significant delay in gastric emptying of solid meals in patients with diabetes and autonomous neuropathy. 6 All of our three patients with diabetes with the longest time for hydrogen appearance had normal gastric emptying rates. Thus it is possible that, whereas slow intestinal transit is probably caused by vagal denervation, the stomach can empty solid meals at a normal rate even when it is deprived of some of its vagal supply.
Conclusions
This study indicates that OCTT is delayed in patients with type 2 diabetes mellitus who have symptoms suggestive of SIBO. This study shows that some patients with type 2 diabetes mellitus having symptoms of a disordered gastrointestinal tract (i.e., diarrhea and flatulence) show SIBO and delayed OCTT. Therefore, they should be treated with prokinetic agents and antibiotics.
Footnotes
Author Disclosure Statement
No competing financial interests exist.