
Abstract
Background:
Sensor-augmented continuous subcutaneous insulin infusion (CSII) therapy is superior to CSII therapy alone, but little is known on the effectiveness of sensor-augmented multiple daily injections (MDI) therapy.
Methods:
We compared during everyday life mean glucose control and several variability indexes recorded for 3 days by a real-time glucose sensor (Medtronic, Northridge, CA) in two groups of children treated with either CSII or MDI. Fifty-five consecutive subjects were examined: 17 receiving CSII and 38 receiving MDI basal–bolus therapy (age range, 7–22 years). All subjects wore the sensor for 4 days, and 3 days were used for statistical analysis. Mean glucose and SD, coefficient of variation (CV), mean amplitude of glucose excursion (MAGE), mean of daily differences (MODD), continuous overall net glycemic action (CONGA) at 2 and 4 h, blood glucose (BG) rate, area under the curve (AUC) above 180 mg/dL and below 70 mg/dL, Low BG Index (LBGI), and High BG Index (HBGI) were calculated.
Results:
Patients receiving CSII administered more daily boluses than patients receiving MDI (5.2±1.5 vs. 3.2±0.3, respectively; P=0.001). Mean glucose was lower in the CSII group. AUC above 180 mg/dL and HBGI were higher in the MDI group. CV, CONGA at 2 h, CONGA at 2 h during the day, and HBGI were worse in the MDI group, whereas MODD, LBGI, BG rate, and MAGE were similar. A positive correlation (r=0.95; P<0.05) was found between the paired sensor–meter values. For the glucose values <70 mg/dL, sensitivity was 40%, and specificity was 99%.
Conclusions:
In our pediatric patients during everyday life sensor-augmented CSII therapy seemed more effective than sensor-augmented MDI therapy, in terms both of glucose mean values and of intraday variability. Mild hypoglycemic episodes and indexes of low BG values were similar in the two groups, although the latter results may be inaccurate because of low sensor sensitivity at low glucose value.
Introduction
Despite opposing opinions focusing on the still insufficient scientific evidence, 3 there is a new awareness that glucose excursions may contribute to diabetes complications, through the accelerated formation of free radicals. 4,5 There are obviously stronger concerns for children with diabetes who are exposed to lifelong glucose fluctuations. Glucose variability therefore is at present considered a possible further parameter to evaluate overall metabolic control, 6 and several indexes can now be statistically calculated. However, reliability of the sensors, despite recent advances, is far from perfect, and sensor accuracy has represented so far a critical point in the achievement of a closed-loop system. 7
Recent studies 8 –10 have demonstrated that sensor-augmented insulin therapy with CSII in adults and children has resulted in a significant improvement in metabolic control compared with MDI therapy, and ongoing studies in subjects with suboptimal metabolic control 11 will provide further evidence as to whether adding CGM to CSII is helpful. The possibility of continuous feedback on glucose levels may in fact induce more frequent changes in both insulin therapy and lifestyle to improve overall metabolic control. So far, however, the use of CGM has mostly been limited to the minority of patients using CSII, possibly because of the opportunity of one of the commercially available pumps to include also a real-time glucose sensor. However, this new technology could theoretically be useful also for those patients following an MDI regimen. Two studies in a small sample of adult subjects compared sensor-augmented CSII therapy versus sensor-augmented MDI therapy, obtaining either a better result in the MDI group 12 or a similar efficacy in the two therapies. 13
The aim of the present study was to compare mean glucose control and 10 inter-intraday variability indexes recorded for 4 days by a real-time glucose sensor (Medtronic, Northridge, CA) in two groups of children treated with either CSII or MDI. This is a cross-sectional observational study carried out during everyday life in children with diabetes, comparing glucose patterns obtained during sensor-augmented MDI therapy with those obtained during sensor-augmented CSII therapy. The primary aim of this nonrandomized study was to observe glucose patterns and number of hypoglycemic episodes during everyday life. All subjects were observed during their normal activities and were specifically encouraged to behave as usual. As a secondary objective, glucose sensor accuracy was evaluated in the sample studied.
Patients and Methods
We examined 59 consecutive subjects who agreed to wear the sensor for 4 days. All subjects gave written informed consent. In four subjects (one receiving CSII and three receiving MDI) the recording was stopped because of the loss of signal of the device before day 4, and they were not considered in the statistical evaluation. Therefore the study included 55 subjects. Seventeen subjects were receiving CSII (Medtronic Veo™ in 10 cases and Paradigm® RT in seven cases), and 38 were receiving MDI therapy. In total, the subjects receiving CSII represented 17 of 23 (74%) of our cases using a Medtronic pump, and 38 of 164 (23%) of our subjects were receiving basal–bolus MDI therapy. MDI consisted of a four-injection basal–bolus regimen with glargine and insulin aspart or lispro as premeal insulin in most cases. Therapy had previously been tailored to the patients. In patients receiving MDI glargine was injected at dinnertime in 40 cases and at lunchtime in three cases. Aspart and lispro were the most common insulins used for all boluses (33 cases), whereas five patients obtained a better control with regular insulin before breakfast and lunch.
To make the two groups more uniform, the following inclusion criteria were used: (1) first time of real-time glucose sensor use; (2) glycated hemoglobin (HbA1c) between 6.5% and 10%; (3) undetectable C-peptide levels; and (4) CSII use or basal–bolus therapy experience for at least 3 months.
Table 1 shows the clinical characteristics of the two groups. The two groups showed homogeneous characteristics at baseline. Age ranged between 7 and 22 years.
Data are mean±1 SD values.
BMI, body mass index; CSII, continuous subcutaneous insulin infusion; HbA1c, glycated hemoglobin; MDI, multiple daily injections.
The sensor was inserted between 4 and 6 p.m. in all cases in the diabetes outpatient clinic. The patient and/or the family were trained to self-measure blood glucose (BG) at least three times a day usually before boluses injections or during hypoglycemic episodes and to insert the data in the sensor. The number of hypoglycemic episodes (BG ≤60 mg/dL) detected by the meters were calculated.
The 4-day period included the weekend in seven of 17 (41%) of patients receiving CSII and in 15 of 38 (39.4%) of patients receiving MDI. In both groups, devices allowed the setting of acoustic and vibration alarms for hypo- and hyperglycemia. In the standard setting, they were fixed at 80 mg/dL and 250 mg/dL, but sometimes they were tailored to patients' characteristics or requests.
In our center all patients are educated on carbohydrate counting and on the possibility of correcting high glucose values (usually >200 mg/dL) between meals with extra boluses. In the case of low BG the patients were instructed to take 15 g of carbohydrate. All patients were encouraged to behave as usual and to continue all their ordinary activities, including sports. They were asked to keep a diary with all the changes made in relationship to extra boluses or possible dietary restrictions due to hyperglycemia outside the three main meals.
Methods
All patients used the Medtronic Sof-Sensor with MiniLink transmitter. For those receiving pump therapy, all using an integrated system (Paradigm Veo or Paradigm Real-Time); glycemic values were directly displayed on the pump screen. Subjects using MDI were given a dedicated monitor for real-time CGM (Guardian® Real-Time). The data of the first incomplete day were excluded from the analysis, and a full 72-h period was considered for statistical evaluation.
Besides average glucose, in order to assess glycemic variability the following parameters were considered: mean glucose; glucose SD and coefficient of variation (CV); mean amplitude of glucose excursions (MAGE), evaluated on peaks and nadirs encountered in a day; mean of daily differences (MODD), defined as the mean of the absolute differences between glucose values on two consecutives days at the same time; continuous overall net glycemic action (CONGA) at 2 and 4 h measured on the overall intra-day variation of glucose recordings (CONGA2 and CONGA4, respectively); BG rate as an index of the dynamics of BG fluctuations on the time scale of minutes; area under the curve (AUC) over 180 mg/dL (AUC 180) and under the curve below 70 mg/dL (AUC 70); and Low BG Index (LBGI) and High BG Index (HBGI). The calculation of the above parameters allows a complete evaluation of glucose variability, 14,15 including intra-day, inter-day, daytime, and nighttime, high and low glucose excursions, speed of fluctuation, 16 and risk of high and low glucose values. 17,18 The nearest HbA1c value (before or after 1 month) was correlated with all the parameters considered in the entire group of patients.
HbA1c levels were measured by high-performance liquid chromatography with the Auto A1c™ model HA 8110 analyzer (Kyoto Daiichi, Kagaku, Japan). The normal range was 4.3–5.9%.
To evaluate the accuracy of sensor readings, a comparison between the paired self-measured BG values using various meters and the next 15-min sensor reading was performed. The time difference took into account the adopted average lag between BG and interstitial glucose. Each patient performed a mean of 3.4±1.1 self-calibrations per day for a total of 822 paired values. For calibration, 10 patients receiving pump therapy used the Contour™ Link meter (Bayer Diabetes Care, Basel, Switzerland), which allows the automatic download of the value to the pump, whereas among the remaining 45 patients, 10 used the Breeze™ 2 (Bayer Diabetes Care), 19 the One Touch® Ultra®2 (LifeScan, Milpitas, CA), and 16 the Glucocard™ meter (Menarini Diagnostics, Florence, Italy). Correlations between the couple values, sensitivity and specificity, and negative/positive predictive values at three glucose levels were calculated (<70, 70–140, and >140 mg/dL).
Statistical analysis
Descriptive statistics were reported as mean±1 SD. Continuous Gaussian variables were compared by means of Student's t test for independent samples, whereas skewed distributions were compared using the Mann–Whitney test. Normality of distribution was tested calculating skewness and kurtosis values. Correlation analysis was performed, and the Pearson correlation coefficient r values were assessed. The agreement between sensor glucose and BG readings was evaluated by κ-statistic. A two-tailed value of P<0.05 was considered significant. For statistical analysis, Stata/SE version 11.0 for Windows (StataCorp LP, College Station, TX) was used.
Results
No subjects reported side effects, and only minimal discomfort was seen during the 4-day period. The patients receiving CSII administered more boluses than patients receiving MDI (daily mean, 5.2±1.5 vs. 3.2±0.3; P=0.001). Eight subjects of the 17 receiving CSII used extended boluses on 19 occasions. Patients receiving MDI reported preferring to adjust snacks if glucose was higher than expected. No serious hypoglycemic episodes occurred. Mild hypoglycemic episodes (≤60 mg/dL) were detected on 42 occasions, with similar frequency in the CSII group (eight of 230 [3.5%]) and in the MDI group (34 of 592 [5.7%]).
Table 2 shows the main differences obtained between the two groups in the parameters evaluated by the sensor. Mean glucose was lower in the CSII group. The AUC 180 and HBGI were significantly higher in the MDI group. Also, parameters of variability such as CV, CONGA2, CONGA2 day, and HBGI were worse in the MDI group, indicating higher variability above all toward hyperglycemic excursion. The day-to-day variation index (MODD) and the LBGI were not different between the two groups. Also, BG rate and MAGE were similar in the two groups.
Data are mean±1 SD values.
AUC 70, area under the curve below 70 mg/dL glucose; AUC 180, area under the curve above 180 mg/dL; BG, blood glucose; CONGA2 and CONGA4, continuous overall net glycemic action at 2 and 4 h, respectively; CSII, continuous subcutaneous insulin infusion; CV, coefficient of variation; HBGI, High Blood Glucose Index; LBGI, Low Blood Glucose Index; MAGE, mean amplitude of glucose excursions; MDI, multiple daily injections; MODD, mean of daily differences.
Correlations
In the whole group of patients HbA1c correlated positively with mean glucose obtained with CGM (r=0.40; P=0.002) (Fig. 1), AUC 180 (r=0.34; P=0.011), and HBGI (r=0.35; P=0.008) and negatively with AUC 70 (r=−0.35; P=0.010) and LBGI (r=−0.42; P=0.002).
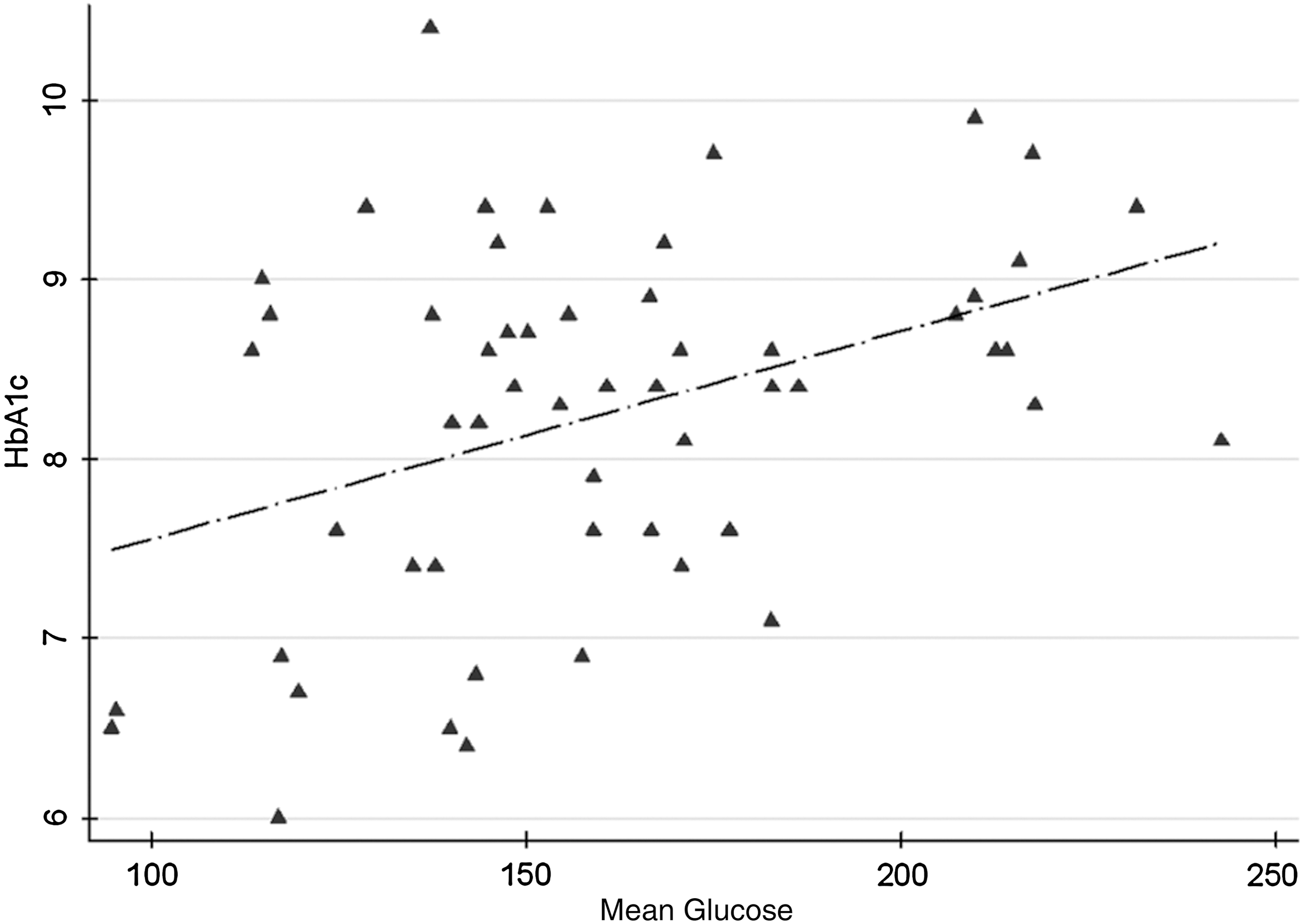
Correlation between glycated hemoglobin (HbA1c) and mean glucose (r=0.40; P=0.002).
Sensor accuracy
A positive correlation (r=0.95; P<0.05) was found between the paired values (Fig. 2). The agreement between sensor glucose and BG readings, evaluated by κ-statistic, was 87.6% (P<0.001).

Correlation between sensor glucose (continuous glucose monitoring system [CGMS] from Medtronic) and blood glucose (BG) readings (r=0.95; P<0.05).
Sensitivity and specificity were calculated separately for the glucose values <70 mg/dL (hypoglycemia), 70–140 mg/dL (euglycemia), and >140 mg/dL (hyperglycemia) (Table 3). For the hypoglycemic range, sensitivity was 40%, and specificity was 99%; positive predictive value was 79%, and negative predictive value was 95%. For the euglycemic range, sensitivity was 88%, and specificity was 88%; positive predictive value was 80%, and negative predictive value was 93%. For the hyperglycemic range, sensitivity was 95%, and specificity was 91%; positive predictive value was 93%, and negative predictive value was 93%.
Hypoglycemic, euglycemic, and hyperglycemic ranges were defined as <70 mg/dL, 70–140 mg/dL, and >140 mg/dL, respectively.
BG, blood glucose.
Discussion
Our short-term, cross-sectional observational study showed that in our relatively small group of children and for the limited period of 4 days, the availability of a real-time glucose sensor is more useful in subjects wearing an insulin pump than in subjects receiving MDI therapy. The subjects on CSII, in fact, obtained a better mean glucose level and also better results in most of the intra-day variability parameters evaluated. If we consider only the mean result, a mean glucose level of 146 mg/dL maintained over time as in the CSII group would lead to an HbA1c of about 6.7%, whereas at the same time the group receiving MDI with a mean glucose level of 167 mg/dL would have obtained a HbA1c of about 7.4% 19 (Table 2). If we consider these theoretical data, both groups therefore obtained a short-term better metabolic control, and it is well known from the Diabetes Control and Complication Trial/Epidemiology of Diabetes Interventions and Complications follow-up that a similar decrease in HbA1c levels would lead to a consistent decrease in diabetes complications. 20 It is interesting to note that the mean glucose value over a 3-day glucose profile showed a significant correlation with HbA1c (Fig. 1), as in a previous study by our group. 21 This would confirm that the glucose patterns of the subjects were consistent with their overall metabolic control and would reinforce the possible long-term improvement if the device were worn for a longer period of time. Certainly our study, carried out during everyday life without a randomized design, has its principal limitation in it lasting only 3 days. Whether this difference in efficacy remains true upon continued use of the real-time sensor, for instance, after several weeks or several months, remains unknown.
The usefulness of the sensor-augmented therapy has already been proved in various studies 8 –10 that included also children and adolescents wearing the pump. The benefits of sensor use have often been related to the time of wearing, and it is well known that children and adolescents above all show a tendency not to wear it over time. 8 As far as we know, there are no studies comparing sensor-augmented CSII versus MDI therapy in children and adolescents. In adults one randomized study including a small number of patients obtained better results in the patients receiving MDI treatment; 12 the apparently surprising data were partially justified by the authors themselves in that included in the MDI group were some subjects with a short duration of disease and possible residual β-cell function. On the other hand, all our subjects showed undetectable C-peptide levels. Our short-term, nonrandomized study was designed to observe the glucose patterns in a non-experimental setting, during normal life. The future availability of less disturbing and cheaper sensors would possibly project our results in a sufficiently longer period that could lower consistently HbA1c levels. We would like to underline that the subjects on CSII tended to administer boluses more frequently, probably because it is painless and simpler than in MDI. It was equally evident that the changes in diet were less effective than an extra dose of insulin. On the other hand, pain caused by multiple injections is a notorious drawback to MDI therapy in children, and there is a general consensus that basal–bolus therapy in the pediatric age is equivalent to a four injections per day schedule in most cases. 22 The recent prospective 6-month study by Garg et al. 13 in adults found that CGM provided similar benefits for patients using MDI or CSII therapy in terms both of lowering HbA1c levels and of glucose variability; similar to our study, all subjects in their study were instructed to adjust insulin doses and/or food intake, and, although not reported, it is possible that the adult patients included in the trial with a mean HbA1c of about 7.5% were more prone to inject extra boluses of insulin.
The small study sample permitted a careful examination of many variability indexes, both within the same day and within the 3 days. In total, 47,520 glucose reading were considered in the analysis, and a complete evaluation on variability over a longer period of time and a higher number of patients would imply the evaluation of an enormous amount of data.
In our study sample there was a statistically significant difference between patients receiving CSII versus patients receiving MDI in glucose SD and in many of the intra-day variables examined. The SD values we obtained in our subjects were consistent with a low variability according to Kovatchev et al., 15,17 and most of our variability indexes were comparable with those obtained in other studies previously published in adult patients. 23,24 Therapy with CSII was better than that with MDI in blunting high glucose excursions, and the percentage of time spent with glucose above 180 mg/dL was doubled in the MDI group (Table 2). This is probably because of the higher number of boluses administered in the pump group, which was more effective than the possible changes in diet. At the same time there were no differences in the LBGI and in the glucose AUC 70. The fact that the latter was less than 1% in both groups confirms that glucose sensors are a useful tool to reduce the time spent in hypoglycemia. 25 Also, the low percentage of mild hypoglycemic episodes (BG ≤60 mg/dL) detected by the meter in both groups is in agreement with these results.
The better CONGA2 values (whole and day), reflecting short-term glucose variability, in the CSII group were probably due to more frequent boluses and to the possibility that these patients could use different types of boluses during the day.
MODD was similar in the two groups, showing that the patient's behavior was similar from one day to another. Also, the speed in glucose variations was similar, probably reflecting the same type of rapid-acting insulin used in most cases.
Finally, despite the fact that the present study was not specifically designed to test sensor accuracy, comparing the values obtained with a laboratory glucose test, our data confirmed on one hand that the sensor showed an excellent correlation with BG values, 26 whereas on the other hand that the sensitivity of the sensor was poor in the low glucose range (44%): the sensor identified in fact only 27 of the 68 glucose values below 70 mg/dL (Table 3). It has already been described that CGM systems tend to overestimate glucose levels in the low range 27 and that a specific algorithm is needed to improve hypoglycemia detection in the 40–120 mg/dL range. 28 It should also be taken into account that the number of low glucose values detected was relatively small, that commercially available meters are allowed an error of±15 mg/dL below glucose 75 mg/dL (ISO 15197), and, finally, that our patients, despite being carefully trained, sometimes performed the requested glucose calibrations during unstable glucose patterns. These data should be considered when in the future a closed-loop system is available and the calibration of the sensor becomes critical.
In conclusion, in our patients during during 3 days of everyday life, sensor-augmented therapy with CSII seemed more effective than sensor-augmented MDI therapy, both in terms of glucose mean values and in terms of intraday variability indexes. Inter-day variability was similar in the two groups. As expected, patients receiving CSII injected more insulin boluses and were more successful in blunting hyperglycemic excursions than patients receiving MDI. Mild hypoglycemic episodes and LBGI values were similar in the two groups, although the latter results may be inaccurate because of low sensor sensitivity at low glucose value. Long-term results in children are needed to confirm our preliminary conclusions.
Footnotes
Author Disclosure Statement
E.M. and L.M. are employees of Medtronic Italia, an affiliate of Medtronic Inc. All other authors have no relationship to disclose.