
Abstract
Background:
The aim of the study is to describe glycemic and insulin outcomes by trimester and maternal and fetal outcome in patients with type 1 diabetes using an insulin pump with constant or intermittent continuous glucose monitoring (CGM).
Methods:
Twenty-five women with type 1 diabetes with newly diagnosed pregnancy were treated with insulin pump therapy (Medtronic 722, Medtronic Minimed, Northridge, CA) for at least 1 year. Insulin pump and CGM (Medtronic Paradigm Real-Time) were implemented at least 3 months before conception. Patients were randomized in two groups: constant CGM group, 12 patients on insulin pump with glucose sensor, 24 h/day; and intermittent CGM group, 13 patients on insulin pump with intermittent glucose sensor, 14 days/month. The following parameters were analyzed: glycosylated hemoglobin (HbA1c), mean blood glucose, insulin requirement (in IU/kg/day), weight gain, severe hypoglycemic events, diabetic ketoacidosis, macrosomia, cesarean section, and neonatal hypoglycemia.
Results:
Both groups achieved good glucose control during their pregnancies (P<0.05): 6.78±1.3% and 6.92±0.9% at the beginning of the study compared with 6.14±0.9% (constant CGM group) and 6.23±0.6% (intermittent CGM group) at the end of the study (last HbA1c before delivery). There was no significant decrease of HbA1c between the two groups. The constant CGM group had a significantly lower A1c in the first trimester compared with the intermittent CGM group. Maternal and fetal outcome did not show a significant difference between the two groups.
Conclusions:
Insulin pump therapy together with constant or intermittent CGM can improve diabetes control and pregnancy outcome in type 1 diabetes. The quality of the glucose profile at conception was the important factor for pregnancy outcome.
Background
Over the past few years, several randomized, controlled clinical trials have been undertaken to evaluate the impact of these devices in the treatment of type 1 diabetes, where the findings are diverse in achieving better metabolic control than traditional multiple daily injections. 9 –11
The Paradigm® Veo™ system (Medtronic Minimed, Northridge, CA) includes an insulin pump with a CGM system. The patient uses glucose readings from the pump monitor in conjunction with occasional confirmatory finger-stick blood glucose measurements to understand his or her current glucose level. The patient programs appropriate insulin delivery based on current glucose, previous bolus insulin, and amount of carbohydrates. The device can alarm if data transmitted from the sensor show decreased or increased glucose levels as defined. If the alarms for decreased glucose level are ignored, the insulin pump automatically suspends insulin delivery for up to 2 h, which may prevent potentially dangerous hypoglycemic events.
CSII and CGM therapy in Macedonia is covered by healthcare funds in a special program for type 1 diabetes. We use modified U.K. National Institute for Clinical Excellence criteria 12 for insulin pump coverage: patients with satisfactory glucose control (glycosylated hemoglobin [HbA1c] <7.0%), without nocturnal or unrecognized hypoglycemia, cannot receive this kind of therapy. Glucose control can be evaluated with the ambulatory glucose profile using blinded CGM, such as with the Medtronic Ipro™2.
Pregnancy in T1DM is a challenge for the patient and her doctor. The use of technology (CSII and CGM) might improve diabetes control and pregnancy outcome. This is the first study in Macedonia of evaluation on constant or intermittent use of glucose sensors in pregnant patients with type 1 diabetes.
The aim of the study was to describe glycemic and insulin outcomes by trimester and maternal and fetal outcome in patients with type 1 diabetes using an insulin pump with CGM either on a constant or intermittent basis.
Patients and Methods
All pregnant women with type 1 diabetes on an insulin pump (n=25) who attended the University Clinic of Endocrinology, Diabetes and Metabolic Disorders in Skopje, Macedonia were included in the study over a period of 3 years. The criteria were singleton pregnancies and CSII for at least 3 months before conception. Patients were randomized into two groups: constant CGM group, 12 patients with CGM (24 h/day); and intermittent CGM group, 13 patients with intermittent CGM (14 days per month).
CSII was performed using aspart or lispro in a Medtronic insulin pump (model 722 or Veo) with a Medtronic MiniLink® sensor. CareLink® Pro software was used for analyzing the glucose trends. Patients were followed every 1–3 weeks by a diabetologist and an obstetrician. The constant CGM group used CGM continuously (24 h/day) with a minimum of two blood glucose calibration per day, and the intermittent CGM group used CGM intermittently (1 week with the sensor and 1 week without the sensor). Patients from the intermittent CGM group measured blood glucose at least six times a day every second week (when not using the sensor).
The following patient characteristics were evaluated (self-reports and previous medical history): age, duration of diabetes, prepregnancy body mass index, smoking habit (smoker/nonsmoker), prior pregnancy, prior miscarriages, and prior macrosomia.
Insulin requirements were calculated as IU/kg/day (current weight), and mean blood glucose was calculated as the weighted mean of self-monitored blood glucose (average of mean values before and after main meals, at bedtime, and during the night) using the CareLink software. Insulin dose was retrieved from the insulin pump in both groups. Patients from the intermittent CGM group, when not using the CGM system, entered the self-monitored blood glucose measurements in the pump.
Measurement of ketonuria was recommended at least once a week and in the case of glycemia >11.1 mmol/L. Weight was measured at each visit. HbA1c (by high-performance liquid chromatography, reference value 4.6–5.8%) was measured monthly, and average values were calculated for each trimester of pregnancy. Mean blood glucose and insulin requirements were recorded weekly, and average values were calculated for each trimester of pregnancy (Table 1).
BMI, body mass index; CGM, continuous glucose monitoring; NS, not significant.
Frequency distributions and appropriate summary statistics for central tendency and variability were used to describe possible differences between the two groups. Statistica software version 8 (Statsoft, Tulsa, OK) was used with Pearson's test for categorical variables, and Student's tests for continuous variables were performed.
Maternal outcomes were weight gain during pregnancy, severe hypoglycemic events (defined as those hypoglycemic episodes where glucagon or intravenous glucose was required to solve the situation), and diabetic ketoacidosis (DKA) episodes (clinical signs with episodes of hyperglycemia, positive ketonemia/ketonuria, and metabolic acidosis pH<7.3). Both events were obtained using emergency room visits.
Fetal outcomes (obtained from the obstetrician's medical history after delivery) were preterm birth, cesarean section, macrosomia (birth weight >4,000 g), and neonatal hypoglycemia (capillary blood glucose lower than the cutoff criterion on two or more occasions in the first 48 h of life, with the cutoff at 1.66 mmol/L).
Results
In total, 25 pregnant patients with T1DM were included in the study. There was no significant difference in demographic data between the two groups. The significant difference was found in prior pregnancies, which has no influence on glucose control. This is also confirmed with no difference in prior macrosomia or prior miscarriages in both groups.
All patients had HbA1c around 7% before conception (Table 2). The significant difference was found in HbA1c and mean blood glucose levels in the first trimester, where patients from the constant CGM group showed more of a decrease in these parameters more than the intermittent CGM group. There was no significant difference in total daily insulin requirements.
CGM, continuous glucose monitoring; HbA1c, glycosylated hemoglobin; MBG, mean blood glucose; NS, not significant.
Figure 1 shows HbA1c levels in both groups during pregnancy.
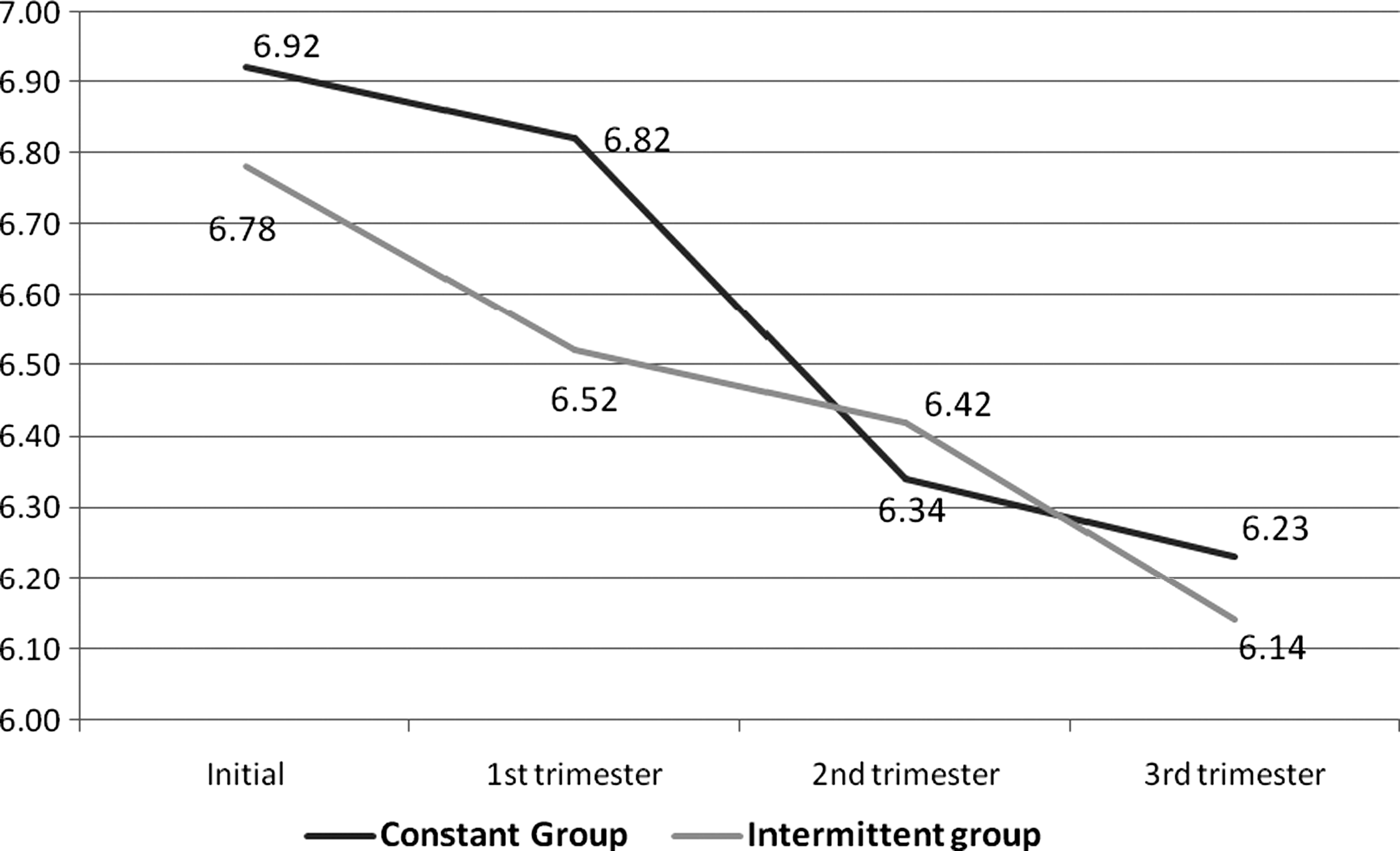
Glycosylated hemoglobin levels in both groups during pregnancy.
There was no significant difference in weight gain in both groups (Table 3). There was a difference between the two groups in severe hypoglycemic event occurrence (one vs. two) and DKA (one episode in the intermittent CGM group). One hypoglycemic event and the DKA episode occurred when patients did not used CGM, and the other hypoglycemic events when patients used CGM.
CGM, continuous glucose monitoring; DKA, diabetic ketoacidosis; NS, not significant.
Discussion and Conclusions
Our data show that pregnant patient with type 1 diabetes using CSII with constant or intermittent CGM can achieve and maintain good glycemic control. In the first trimester, there was a significant decrease in HbA1c levels in the constant CGM group compared with the intermittent CGM group, with a nonsignificant difference in fetal outcomes in the two groups. Hypoglycemic and DKA events occurred more in the intermittent CGM group, when the patients did not use CGM.
The main objective of glucose control in patients with T1DM is to maintain the levels close to normal in the absence of hypoglycemia, which can be done by using technology such as CSII and CGM. Pregnancy in combination with T1DM needs special care. Successful insulin pump therapy is dependent on each patient's ability and motivation to learn to use the insulin pump correctly and ongoing education delivered by qualified clinicians. 13 Besides frequent blood glucose monitoring, motivation is also an important key for optimal glucose control during the pregnancy in patients with T1DM. 14
Our study shows that CGM as part of CSII in pregnant patients with T1DM may prevent hypoglycemic events and DKA, but there is no difference in other fetal and maternal outcomes. Observational studies using CSII rather than multiple daily injections performed in pregnant women with diabetes have shown significant reduction in glucose variability. 15,16 Recent data showed that CSII can increase the rate of DKA and neonatal hypoglycemia. 17 Alternatively, the use of short-acting insulin analogs with or without CSII was beneficial in terms of hypoglycemic comas for fetal outcomes and had a favorable or an unfavorable influence depending on the specific outcome. 18 Further studies showed that both multiple daily injections and CSII can provide good glycemic control, and there is no significant difference in pregnancy outcome. 19,20
CGM can improve DKA and hypoglycemic events, 21 where the patient makes changes in insulin delivery based on glucose profiles. Several CGM systems are approved in T1DM, but only one (Medtronic MiniLink and Paradigm Real-Time 722) has direct communication between the pump and the sensor. The system can stop basal insulin delivery if blood glucose decreased to the programmed level (for example, <2.2 mmol/L) and can prevent nocturnal hypoglycemia. The other advantages of these systems are prediction of high and low glucose levels and Bolus Wizard calculations (bolus insulin calculated based on glucose value, carbohydrate intake, and previous bolus insulin delivery). Our study shows significant improvement in glucose control in the first trimester, when patients using constant CGM achieved better HbA1c compared with patients using internment CGM, but in the end there is no significant difference. The data show a difference in severe hypoglycemic events and DKA, but with a total number of three events we cannot conclude the relevance of this finding. Lower numbers of hypoglycemic episodes per woman in the group using CSII were also reported in other studies. 22 Patients suspended the insulin pump one or two times in a total period of 1 h/day for nonphysical activity (shower, bath). There was a slight increase in glucose values for an average of 32 mg/dL (1.8 mmol/L) after the suspend time. Patients were advised to give correction bolus insulin based on the basal dose rate and suspend time, where glucose values were slightly decreased in the next 2 h.
Despite the fact that tight glucose control in the first trimester is very important in decreasing congenital malformations, although our data showed a significant decrease in HbA1c levels in the first trimester in the constant CGM group compared with the intermittent CGM group, further investigations using CGM in the first trimester should be performed.
The limitation in our study is the number of patients, and we must emphasize that Macedonia (population around 2.5 million) has a low diabetes incidence and prevalence, compared with other countries (new type 1 diabetes cases per 100,000 inhabitants: 3.9 in Macedonia vs. 8.9 in Croatia, 18 in Germany, 20.8 in the United States, and 24.5 in the United Kingdom). 23
The number of publications on this topic is very low, and the number of patients is also very small. The other disadvantage for further evaluation is the very high cost of this kind of therapy (insulin pump, consumables, and sensors), where the average monthly cost only for a sensor is around $300 US and in most European countries is not covered by the health fund or insurance companies or there is a demanding procedure for financial coverage. 24 On the other hand, glucose sensors with transmitters for patients with T1DM are covered by the healthcare fund, using a special program for patients in Macedonia. Our results show that there is no difference in pregnancy outcome in both groups (constant and intermittent CGM in patients with T1DM using CSII).
Both continuous and intermittent CGM together with CSII achieved good glucose control and pregnancy outcome in patients with T1DM, where the constant CGM group had significantly lower HbA1c during the first trimester. The quality of glucose profile at conception was the important factor for pregnancy outcome. Further investigation on more data should be performed to confirm these findings.
Footnotes
Acknowledgments
We want to thank the Macedonian Ministry of Health and the Health Care Fund of Macedonia for financial support.
Author Disclosure Statement
No competing financial interests exist for any of the authors.