
Abstract
Background:
Severe hypoglycemic episodes are a barrier for achieving optimal glycemic control. Sensor-augmented pump (SAP) therapy with insulin in combination with a novel mechanism of automatic insulin shutoff (low glucose suspend [LGS]) can be used to prevent and reduce hypoglycemia. In a prospective study, we investigated the effect of the LGS algorithm on the frequency of hypoglycemia in children and adolescents with type 1 diabetes under real-life conditions.
Methods:
Twenty-one patients with type 1 diabetes (10.8±3.8 years old, duration of diabetes 5.9±3.0 years, pump therapy for 3.7±1.7 years, glycated hemoglobin level 7.8±1.1%) from three pediatric centers used the Paradigm® Veo™ system (Medtronic Minimed, Northridge, CA) during two subseqent time periods: SAP without LGS for 2 weeks and then SAP with LGS enabled for 6 weeks. The primary objective was to assess the frequency of hypoglycemic episodes when using the LGS feature with an insulin delivery shutoff of a maximum of 2 h at a sensor glucose level below 70 mg/dL (3.9 mmol/L).
Results:
In total, 1,298 LGS alerts occurred (853 shorter than 5 min). Forty-two percent of LGS activations (>5 min) lasted less than 30 min, whereas 24% had a duration of 2 h. The number of hypoglycemic excursions (average/day) was reduced during SAP+LGS (<70 mg/L, 1.27±0.75 vs. 0.95±0.49, P=0.010; ≤40 mg/dL, 0.28±0.18 vs. 0.13±0.14, P=0.005) as was the time spent in hypoglycemia (average minutes/day, 101±68 vs. 58±33, P=0.002) without significant difference in the mean glucose level (145±23 vs. 148±19 mg/dL). No episodes of severe hyperglycemia or diabetic ketoacidosis were observed following LGS activation.
Conclusions:
The present investigation provides evidence that SAP with LGS reduces the frequency of hypoglycemia without compromising safety.
Introduction
The integration of the insulin pump with a CGM system—sensor-augmented pump (SAP) therapy—has been shown to lead to a significant improvement in diabetes management. In randomized controlled trials, significant reductions in glycated hemoglobin (A1C) levels were observed with SAP use compared with intensive insulin therapy by multiple daily injections or pump alone. 8 –11 Real-time CGM offers the possibility of proactively avoiding hypoglycemic episodes through adjustable alert limits. 12 –14 However, patients do not always react to the alerts.
The Paradigm® VEO™ system (PRVEO) (Medtronic MiniMed, Inc., Northridge, CA) is equipped with a low glucose suspend (LGS) feature that leads to an interruption in the supply of insulin for a period of up to 120 min. This occurs when the glucose value falls below an adjustable hypoglycemia threshold (set by the patient and healthcare provider) and the patient does not respond to the alert and turns off insulin suspension to resume insulin delivery. After the LGS is triggered, if the patient fails to respond by resuming insulin delivery, insulin suspension will last for 120 min, after which insulin delivery will be automatically resumed for 4 h, even if the sensor glucose value falls below the set LGS threshold again. However, if at the 4-h interval the glucose value reaches the LGS threshold, another cycle of 120-min suspension followed by 4-h insulin delivery will be resumed. The goal of this algorithm with insulin delivery cycling on and off is to prevent the occurrence of diabetic ketoacidosis after LGS events. 15
The aim of our investigation was to determine whether the number, the duration, and degree of hypoglycemic episodes could be reduced through the use of the LGS feature under real-life conditions, using a hypoglycemia alert level of 75 mg/dL (4.2 mmol/L) and an LGS threshold of 70 mg/dL (3.9 mmol/L), and what effects the use of LGS had on metabolic control in pediatric patients.
Study Design and Methods
Twenty-one children and youth with type 1 diabetes (1–18 years of age, duration of diabetes ≥12 months, continuous subcutaneous insulin infusion [CSII] for ≥3 months) from three diabetes centers in Germany with experience in CSII, CGM, and SAP were included in the study. Prior to the start of the study, patients were placed on and patients and parents were trained on the use of the PRVEO system. The system is certified and available in Europe (EC Certificate number 1285 B2P3/5, EC Certificate number 1285/13485/2, and EC Certificate number 1285/13485/3).
Two phases were compared with each other in this prospective study. The first phase (2 weeks) consisted of SAP without the use of LGS, as previous research has shown that such CGM time is sufficient to determine the hypoglycemia rate in terms of statistical safety. 16,17 The second phase was longer, for a period of 6 weeks, as no previous experience on the behavior of patients using the LGS algorithm was available. The hypoglycemia alert was set at 75 mg/dL (4.2 mmol/L), thus slightly higher than that commonly defined for hypoglycemia. The rationale for the difference is the inherent “time lag” between blood glucose and sensor glucose (measured in interstitial tissue). A sensor glucose value of 75 mg/dL (4.2 mmol/L) may correspond to blood glucose values below 70 mg/dL (3.9 mmol/L) in the event of rapidly decreasing glucose levels. However, values below 70 mg/dL were used for our analysis of hypoglycemic episodes (see below). The hyperglycemia alert was set at 200 mg/dL (11.1 mmol/L) but could be adjusted individually by the patient. In the second phase (SAP+LGS), LGS was used for 6 weeks. A value of 70 mg/dL (3.9 mmol/L) was set for the LGS threshold. The hypoglycemia alert level was kept at 75 mg/dL, and the hyperglycemia alert was 200 mg/dL for Phase 2 of the study, like in Phase 1. Prior to the start of the second phase, a special training session on the use of the LGS was conducted again. After 2 weeks in Phase 2, a telephone visit was conducted to answer any questions that had arisen and to document any possible deficiencies from the patient's viewpoint. Additionally, at the end of the study, patients and/or their parents answered questions on the use of the PRVEO with the aid of the Device Satisfaction Questionnaire.
After each phase of the study, CGM data were processed using CareLink® Clinical Therapy Management software. For Phase 2, the frequency of LGS activations was determined. Statistical calculations of the number of hypoglycemic episodes (≤70 mg/dL, 3.9 mmol/L), the glucose average, and area under the curve per day as well as the time per day spent in the glucose range ≤70 mg/dL (3.9 mmol/L) in the two phases of the studies were carried out with the paired t test by using SPS program software (SPSS, Inc., Chicago, IL).
Results
Twenty-one patients from three pediatric centers (10.8±3.8 years old, duration of diabetes 5.9±3.0 years, CSII for 3.7±1.7 years) were available for analyses. All patients used the glucose sensor over 90% of the time over 8 weeks. The baseline A1C level was 7.8±1.1% (measured with the DCA 2000, Bayer, Leverkusen, Germany). A total of 445 LGS activations occurred in which the insulin supply was interrupted, or 0.89±0.67 LGS activations per patient per day. When subdivided into daytime and nighttime, the results were 0.38±0.32 LGS per patient per day for the time between 10:00 p.m. and 6:00 a.m. and 0.49±0.43 LGS per patient per day for the time between 6:00 a.m. and 10:00 p.m. (Fig. 1). If all LGS alerts are counted, including those that the patients confirmed and no interruption in insulin delivery occurred, there were 853 events <70 mg/dL (3.9 mmol/L). When these alerts are included in the total, this average comes to 2.56±1.86 LGS per patient per day.
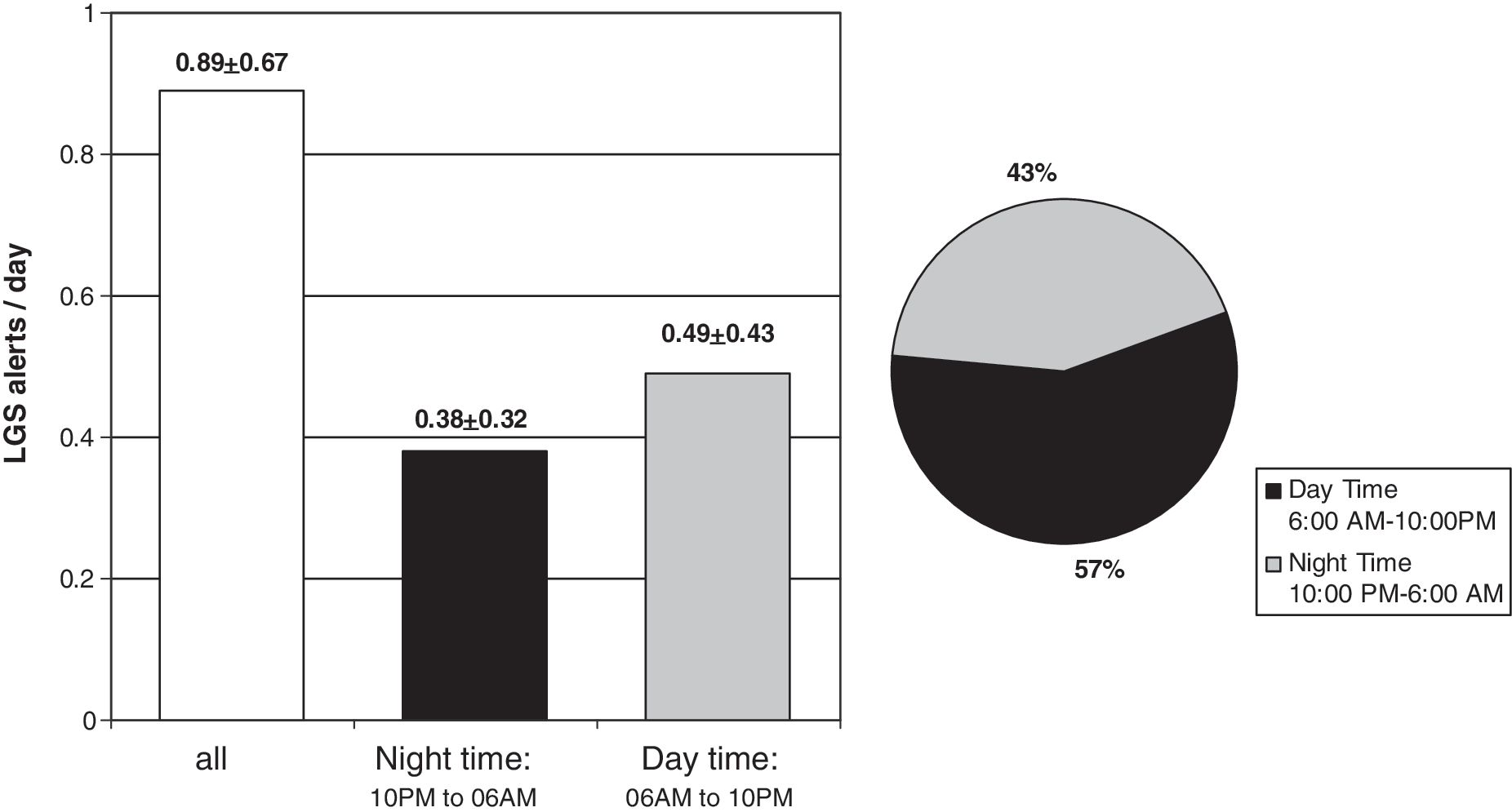
Frequency of low glucose suspend (LGS) activations/day in pediatric patients with type 1 diabetes: (
The distribution of the duration of LGS activation is given in Figure 2. A high percentage (24.5%) of interruptions of insulin supply for 120 min was detected. The insulin supply was automatically switched on and off without active intervention at a rate of 0.21±0.15 LGS per patient per day. In contrast to the total number of LGS alerts and the total number of LGS activations, the complete cycle occurred primarily during sleep time (84.4% of the 120-min interruptions). Comparing the glycemic parameters during the two phases of the investigation, a significant improvement in all parameters of hypoglycemia was observed with LGS, whereas average glucose or occurrence of hyperglycemia remained unaffected (Table 1).
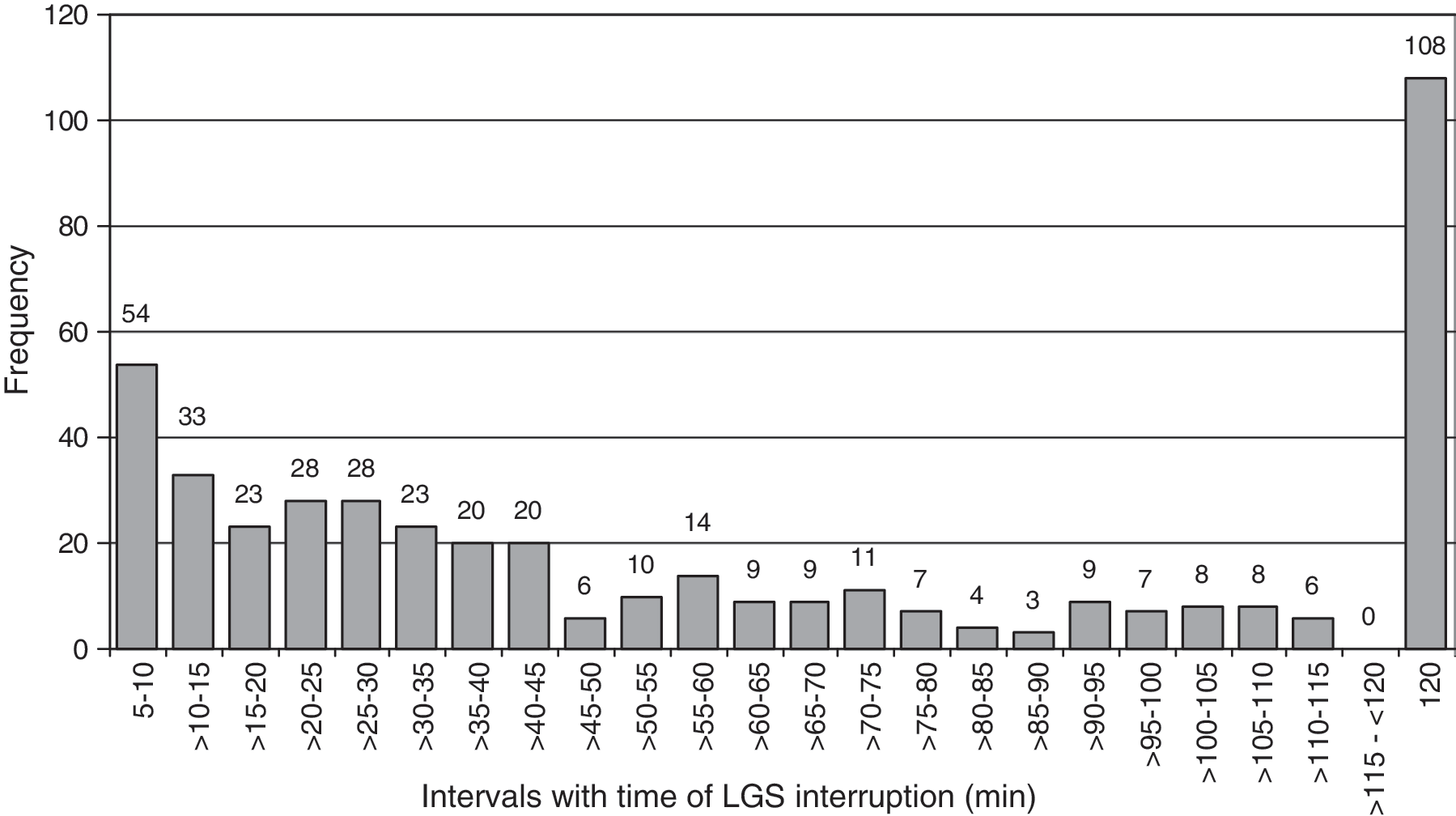
Distribution of the duration of low glucose suspend (LGS) interruptions in 21 pediatric patients with type 1 diabetes (5-min intervals).
AUC, area under the curve; LGS, low glucose suspend; NS, not statistically significant.
Using the Device Satisfaction Survey, the majority of patients and their parents evaluated the management of hypoglycemia and the PRVEO system very positively (Table 2), although patients with a high number of alerts tended to be a little less content. Corresponding to the evaluation according to the 7-step Likert scale (1=do not agree, 7=fully agree), a total score of 5.3±0.6 occurred for the respective questions. However, because of reimbursement restrictions in Germany only five patients were able to continue with SAP after the conclusion of the study.
The scale ranged from 1=do not agree to 7=completely agree.
LGS, low glucose suspend; PRVEO, Paradigm Veo system.
Discussion
The present study provides evidence for reducing the risk for hypoglycemia with LGS without compromising the safety of CSII therapy in children with type 1 diabetes. The occurrence of severe hypoglycemia has been labeled as the rate-limiting step in achieving optimal metabolic control. 18 Children with type 1 diabetes are particularly prone to hypoglycemia, 19 which leads to significant parental anxiety adding complexity to this issue. 20 Thus, SAP therapy with LGS may offer a new therapeutic option with potential long-lasting consequences.
The LGS algorithm was effective using 70 mg/dL (4.2 mmol/L) as the threshold for the onset of LGS. This value allowed for a reduction in time spent and number of episodes of <70 mg/dL (Table 1) without a concomitant rise in hyperglycemia (Fig. 3). Because of the sequential design of the study, it is possible that there were other factors that could account for differences between the study phases besides the LGS feature. However, most patients already had experience with CGM in the past. Overall parameters of insulin treatment such as number of boluses or total insulin dose remained the same. Although subtle changes in the insulin management cannot be ruled out as a contributing factor for this observation, this appears unlikely. Although the mean glucoses and time above target during both phases remained identical, all parameters of hypoglycemia changed significantly (Table 1).

Two example cases of successful prevention of likely severe hypoglycemia. (

Even though not all hypoglycemic episodes were avoided with this LGS threshold, it is possible that setting a higher LGS threshold of 80 mg/dL (4.4 mmol/L) or 90 mg/dL (5.0 mmol/L) may be successful in reducing low glycemic excursions even further. This may be desirable, for example, in patients prone to hypoglycemia or young children at greater risk for neurocognitive consequences. However, potential hypoglycemia reduction by setting the threshold higher has to be balanced with the occurrence of more LGS alerts. Increasing the overall number of alerts may affect the patient's sensitivity to the alerts and the overall patient acceptance of the device. Instead of raising the LGS threshold levels, implementing a predictive LGS when rapidly falling glucose values predicted to reach the hypoglycemic range would trigger insulin suspension could be even more effective in preventing low glucose. 21
In a 6-h cycle the 2-h suspended insulin delivery is followed by 4 h of basal insulin delivery. In the absence of intervention, this 6-h cycle continues indefinitely. For the period of the study five patients cycled twice, and one patient cycled three times. During the LGS time, there was an elevation in glucose concentration of 68.4±13.1 mg/dL (3.8±0.73 mmol/L) after the 2-h interruption or a rate of approximately 35 mg/dL/h. Reactive ketoacidosis is not to be expected, even in the presence of serious patient errors (e.g., calibration-associated errors). We observed a case of sensor failure due to an extension of the sensor implantation time way beyond the recommended duration. The erroneous low glucose readings due to sensor failure prompted subsequent interruptions in the insulin supply during the night but did not result in diabetic ketoacidosis (Medtronic data on file). The elevated morning glucose could be readily corrected in the morning as would have been the case without LGS.
The rate of LGS activations was higher during the waking hours (6:00 a.m.–10:00 p.m.) compared with sleeping time (10:00 p.m.–6:00 a.m.). Several reasons may account for this. Glycemic variability is generally higher in the daytime, and the alerts were frequently canceled by the patient (Fig. 3). This cancellation explains the high number of LGS alerts not leading to activation of insulin suspension (n=853). As expected, patients reacted by ingesting food, or they interrupted the insulin supply manually, just as the LGS algorithm would have done otherwise (Fig. 3). Afterward, the glucose profile of all patients exhibited an increase of the glucose gradient into the normoglycemic target range. According to our data, it can be assumed that the general usage of LGS without patient intervention would actually represent the best option as manual intervention regularly led to bigger glycemic excursions. This should be investigated in further studies.
In conclusion, the present two-phase study of 2 weeks of SAP therapy only compared with 6 weeks with the enabled LGS displayed a reduction in the frequency of hypoglycemic episodes by using the LGS function in children. The fact that no reactive negative effects on glycemia occurred emphasizes the safety and feasibility of this approach.
Footnotes
Acknowledgments
The study received financial support from Medtronic Germany.
Author Disclosure Statement
This study is an investigator-initiated trial supported by Medtronic Germany. Consumables and Paradigm VEO pumps were supplied by Medtronic. T.D. received honoraria for scientific lectures, consulting fees, and travel reimbursement from Medtronic, Abbott Diabetes Care, DexCom, Roche, Bayer HealthCare, E. Lilly, GSK, sanofi aventis, and NovoNordisk. O.K. received honoraria for scientific lectures and travel reimbursement from Medtronic MiniMed and Bayer HealthCare and consulting fees and travel reimbursement from Lilly Deutschland and NovoNordisk. M.H., H.H., S.G., K.R., S.B., T.W., and S.Z. are employed in hospitals and declare no competing financial interests. R.H. is a self-employed statistician and declares no competing financial interests. A.T. is an employee of Medtronic GmbH Germany.