
Abstract

Kraegen, Chisholm, and colleagues in Australia found in the early 1980s that fully closed-loop insulin delivery with intravenous glucose sensing and intravenous insulin infusion failed to control meal-induced hyperglycemia but that this could be improved by prompt augmented open-loop infusion with meals, mimicking the physiological early insulin release at meals. 4,5 They remarked that “glucose-controlled insulin infusion performs considerably better during the basal rather than meal periods. We suggest that a practical alternative, which has the advantage of also being simpler technically, is to relate insulin delivery to blood glucose intermittently (semi-closed loop) and to provide open-loop meal delivery.” 6
The problem of inadequate closed-loop control of meal-related hyperglycemia is of course hugely compounded by subcutaneous glucose sensing and subcutaneous insulin delivery, the most feasible routes for an artificial pancreas that is usable in routine outpatient clinical practice. As Hovorka 1 has pointed out, with subcutaneous sensing/subcutaneous insulin delivery, the delay between a rise in blood glucose concentration after a meal and insulin action to lower that blood glucose concentration may be about 100 min, making fully closed-loop management of postprandial hyperglycemia very difficult. However, in a hybrid artificial pancreas, addition of a small manual premeal priming bolus is able significantly to reduce mean peak postprandial glucose levels, for example, in the system reported by Weinzimer et al., 3 from 12.6 mmol/L (226 mg/dL) seen in a fully closed-loop system to 10.8 mmol/L (194 mg/dL) with semi-closed-loop insulin delivery.
A recent notion in insulin delivery has taken the idea of hybrid systems a step further—instead of a long period of closed-loop (basal±the last part of the meal) and a short period of open-loop (premeal) insulin delivery, “control-to-range” or “control-to-target” systems are based on a long period of open-loop and a short period of closed-loop delivery (Fig. 1). Here, continuous subcutaneous insulin infusion (CSII) is used to control blood glucose in usual open-loop mode for most of the day. Glucose levels, as measured by continuous glucose monitoring (CGM), are allowed to fluctuate between quite wide preset levels, but when the blood glucose falls below a preset threshold, the basal insulin infusion rate of the pump is automatically suspended for a temporary period to allow blood glucose to rise out of hypoglycemia, or when CGM readings exceed the preset high glucose level, a temporary boost of insulin is automatically given by the pump to lower blood glucose into the set range. A commercially available insulin pump with automatic low-glucose suspend (LGS) (Paradigm® Veo™, Medtronic Inc., Northridge, CA) has been in clinical use in the United Kingdom since June 2009 and in parts of Continental Europe since September 2009. With this pump, an alert sounds when the low glucose threshold is reached, and the basal insulin rate is automatically suspended. The user has an option to continue the suspend for up to 2 h or to cancel the suspend at any time up to 2 h, when insulin delivery resumes immediately. A pump with high glucose-initiated insulin boost (in addition to or instead of LGS) has not yet been marketed by any company, but clearly will be the subject of research and development in the coming years.
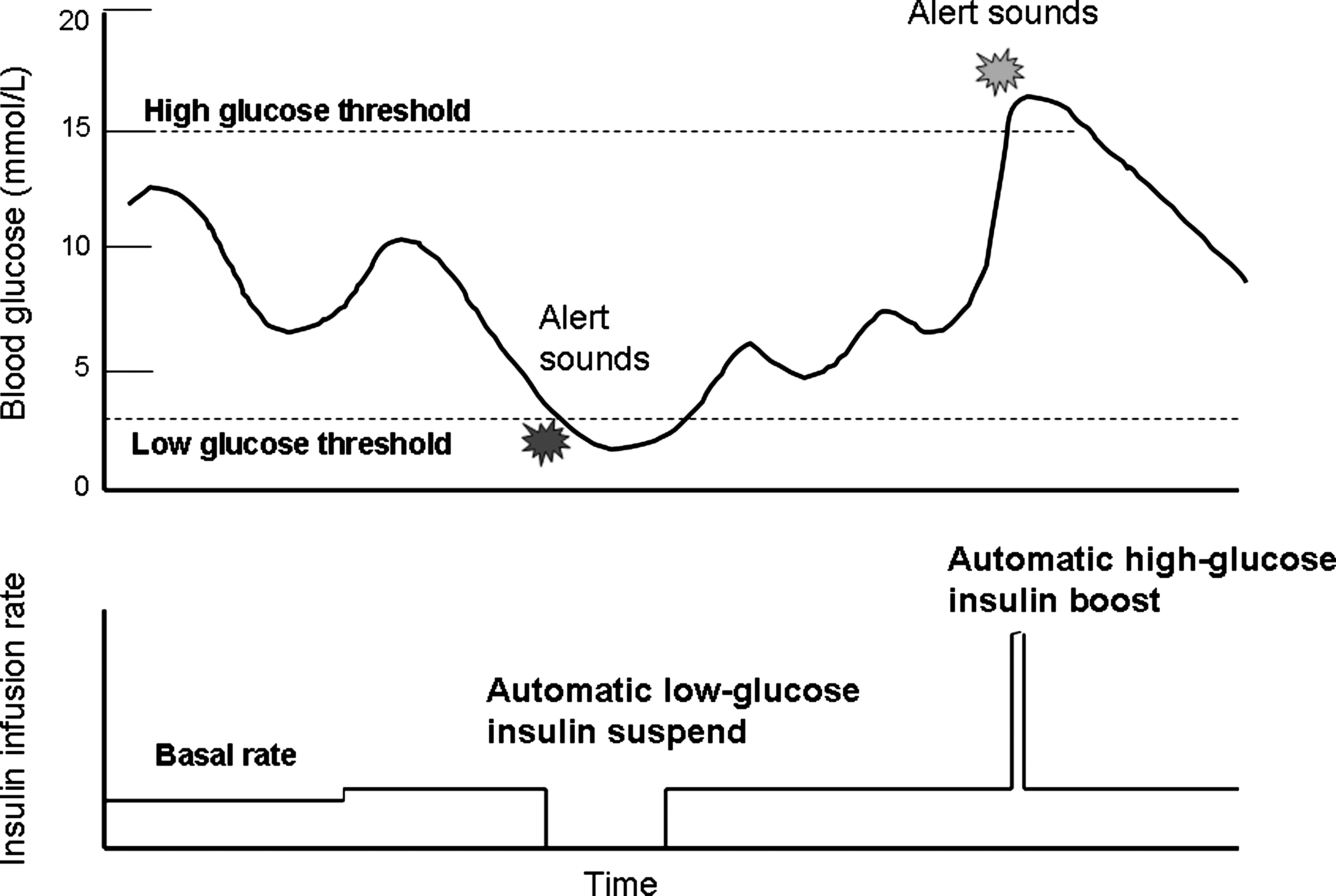
The concept of “control-to-range” semi-closed-loop insulin delivery systems. Blood glucose, tracked by continuous glucose monitoring, is allowed to fluctuate between a set high and low glucose threshold. When the continuous glucose monitoring reading falls below the theshold (or is predicted to do so), the basal insulin infusion rate is automatically suspended, and blood glucose rises into the target range. Future pumps could have the capacity to deliver an automatic insulin boost when the continuous glucose monitoring–tracked glucose rises above the high threshold.
What is the duration of insulin suspend likely to reduce the severity of hypoglycemia without causing dangerous hyperglycemia and ketosis? Clues to this again come from 30-year-old research. In an early study designed to examine the safety of CSII in the event of pump breakdown or planned removal, for example, for bathing, we deliberately stopped basal insulin infusion (using regular insulin) for up to 9 h in a group of pump-treated patients and found that blood ketones (3-hydroxybutyrate) did not rise above the reference range until 3 h after suspend; with a 2-h suspend the plasma glucose concentration rises only moderately, and ketosis does not develop. 7 Several subsequent studies where delivery from CSII pumps has been interrupted have confirmed the safety of a 2-h suspend, 8 –10 including when monomeric analog insulin is used, 8,9 where the increase in glycemia and ketonemia is similar at 2 h post-suspend for both regular and monomeric insulins. Furthermore, examination of data from closed-loop insulin delivery system runs shows that when insulin delivery was automatically interrupted on the basis of predicted hypoglycemia, or rapidly falling or below-target glucose levels, insulin suspend for up to 210 min did not give rise to severe hyperglycemia or ketosis. 11,12
First analysis of the clinical performance of an LGS pump is very favorable. In a recent six-center trial in the United Kingdom, we studied 31 adults with type 1 diabetes during a period of conventional CSII, followed by a 3-week period of CSII with LGS. 13 With a mean threshold of 2.4 mmol/L (43 mg/dL), the LGS was activated in 86% of the subjects, on average 1.9 times per week; 12% of the suspends were for the maximum 2-h period, with the majority occurring at night. Most of the LGS events were terminated at <10 min by the patients. In those subjects with the highest frequency of nocturnal hypoglycemia at baseline, the duration of nocturnal hypoglycemia (<2.2 mmol/L [40 mg/dL]) was reduced from 46.2 to 1.8 min/day (conventional CSII vs. LGS pump, P=0.02). Significant hyperglycemia did not occur; even after the 20 episodes of full 2-h insulin suspend, the median glucose at the termination of suspend was 3.9 mmol/L (70 mg/dL), and 2 h later it was 8.2 mmol/L (148 mg/dL). Although patient satisfaction questionnaires in volunteer trials of innovative technology are, of course, notoriously difficult to interpret, >95% of the trial patients would have liked to continue with the LGS pump if it were available, and all those studied thought the LGS feature was helpful in their diabetes management.
Similar results have been reported from a study in Germany where data were available from 21 pediatric diabetic subjects using the LGS pump; again, most suspends lasted for only short periods of time (66% were <5 min), but 24% were for the full 2 h or longer. 14 The area under the curve for <3.9 mmol/L (70 mg/dL) was reduced from 0.76 to 0.53 (conventional CSII vs. LGS pump, P=0.05), as was the duration of hypoglycemia (a reduction of 43%) and the number of hypoglycemic excursions. No episodes of severe hyperglycemia or ketoacidosis were observed following LGS.
In clinical practice, it is to be expected that those who are most likely to benefit from an LGS pump are patients who continue to have a high frequency of hypoglycemia and/or hypoglycemia unawareness on conventional CSII, for example, because of variable subcutaneous insulin absorption, gastroparesis, unpredictable responses to exercise, or renal impairment. Perhaps those with excessive fear of hypoglycemia may also be helped. The example LGS event shown in Figure 2 is a computer download for 1 day in a 55-year-old patient with a duration of type 1 diabetes of 48 years who has diabetic nephropathy and has been hypoglycemia-prone for many years. She was transferred from CSII to the LGS pump because of worsening hypoglycemia. After 5 months, no severe hypoglycemic episodes had occurred, nocturnal hypoglycemic episodes were largely prevented, the fear of hypoglycemia score was reduced by 50%, and hypoglycemic symptoms had reappeared. No post-suspend severe hyperglycemia or ketosis has occurred.

Computer download showing an example low glucose suspend event in a patient with hypoglycemia-prone type 1 diabetes. Note that the continuous glucose monitoring trace declines during the night from midnight and falls below the set low glucose suspend threshold at about 2 a.m. The patient terminated the suspend after 74 min, allowing the blood glucose (BG) concentration to rise into the target range. Color images available online at
Some thousands of type 1 diabetes patients have now been using LGS pumps in Europe, and now is the time to pool information on performance, best practice, and any untoward events noted so far. Much needs to be learned—the optimal setting of the LGS threshold for a particular patient, the duration of patient-determined suspend, and whether and what quantity of carbohydrate to take in response to an LGS alarm. Has LGS been associated with higher than anticipated post-suspend hyperglycemia at certain times and in certain individuals, such as in the psychologically stressed person, or after exercise or during illness?
The issue of how often the LGS is activated by a sensor reading an apparently low value when the blood glucose is not in the hypoglycemic range or clearly elevated is important. This is difficult to judge at the moment. Near-simultaneous blood glucose levels and sensor glucose readings at the time of the LGS alert have been obtained for only a minority of episodes, and often patients will have eaten carbohydrate before taking the capillary blood sample (about 75% of patients have given carbohydrate at some point around the time of the alert). Well-designed studies with systematic recording of blood glucose at the time of LGS alert and, above all, randomized controlled trials comparing CSII (with or without CGM) versus the LGS pump, with outcomes including hypoglycemia, quality of life, and treatment satisfaction, are needed.
How will the technology develop? In the current version of the LGS pump, suspension is triggered by the absolute prevailing glucose level, but there may be advantages to interruption of the basal infusion based on predicted hypoglycemia. Studies under short-term hospital conditions have already shown that algorithms that activate insulin suspend when hypoglycemia is predicted can significantly reduce both daytime and nocturnal hypoglycemic events. 15,16 The possibility in a future generation of semi-closed-loop pump of triggering a boost of insulin in response to sensor-monitored hyperglycemia is mentioned above.
Three other technologies under development may also be of relevance. The future use of ultra-short-acting insulin in insulin pumps 17 or intradermal microneedles for insulin infusion 18 may ensure swifter recovery from hypoglycemia on LGS activation, and therefore there is the possibility that the duration of suspend may need to be shortened to avoid hyperglycemia and ketosis with this type of insulin. New generations of glucose sensors will be more accurate, and it can be expected that concerns about false-positive LGS (inappropriate suspend when there is hyperglycemia) will be less. And, with the advent of increasingly more automatic insulin delivery based on subcutaneous CGM, will there be a paradigm shift in diabetes management from blood glucose- to interstitial glucose-based information about diabetes control?
Although clinical experience clearly is still limited, LGS pump technology does seem to be a practical, comparatively simple, and effective (semi-) closed-loop insulin delivery strategy for routine use in at least some patients. We look forward to more reports.