
Abstract

Dear Editor:
This equation is used bidirectional for transformation of HbA1c(IFCC) values into corresponding HbA1c(NGSP) values, and vice versa. For the imprecision of results expressed with IFCC units (mmol/mol) or NGSP units (%) the equation is not applicable. The difference between CV% for the two scales are shown in Figure 1. A CV% of “5” for HbA1c(IFCC) corresponds to a CV% of “4” for HbA1c(NGSP) at the HbA1c level of 100 mmol/mol but to “3” at the level of 40 mmol/mol. The CV% for HbA1c(IFCC) is always higher than the CV% for HbA1c(NGSP) even if the analytical quality is the same.
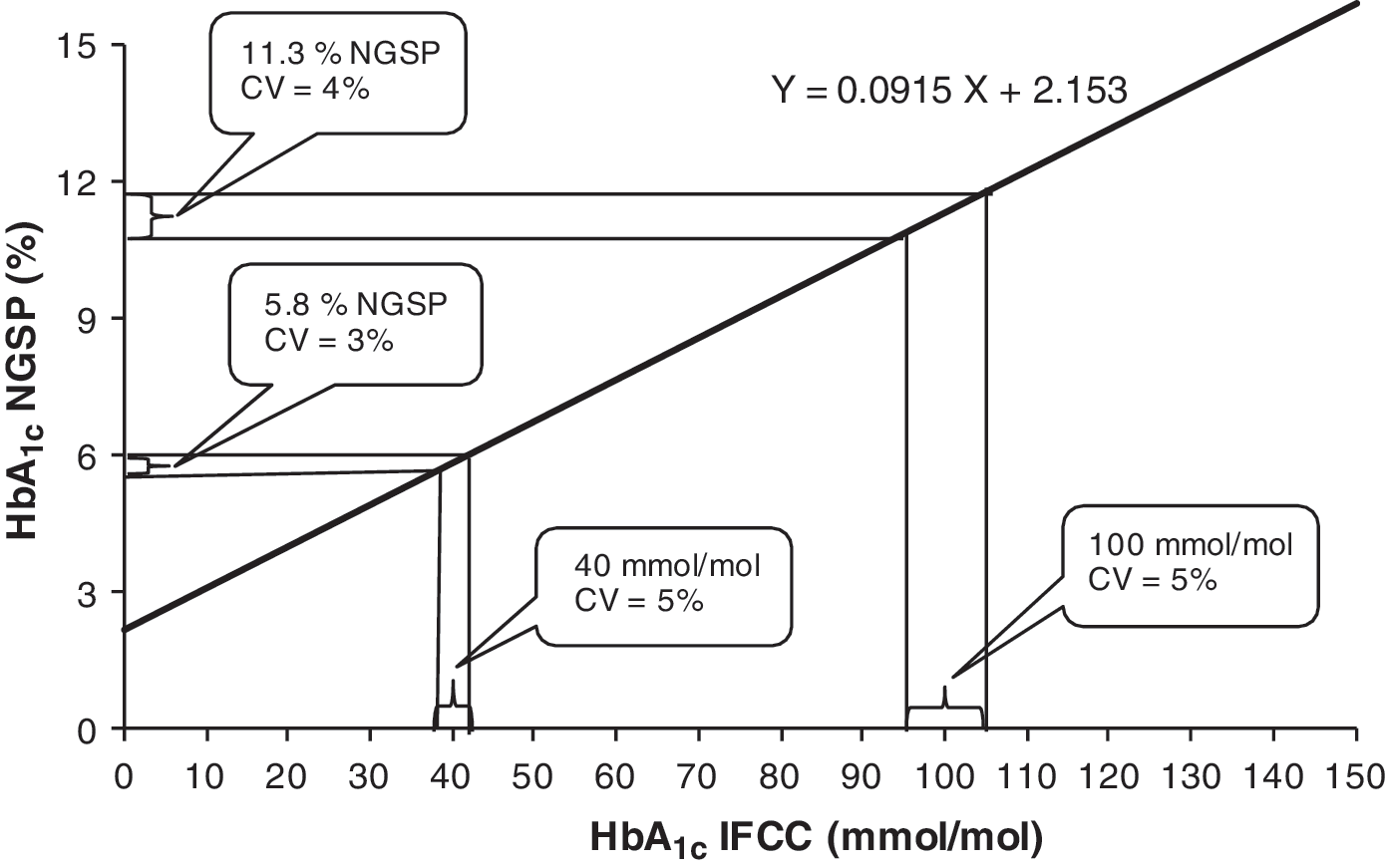
The relation between hemoglobin A1c (HbA1c) in National Glycohemoglobin Standardization Program (NGSP) units and HbA1c in International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) units according to the “master equation.”1 Two values of HbA1c(IFCC)—100 mmol/mol and 40 mmol/mol, respectively—are indicated together with±5% limits on the IFCC scale and the corresponding limits on the NGSP scale.
Diabetes Technology & Therapeutics is appreciated for publishing the HbA1c results expressed in the new IFCC unit together with the old NGSP unit, as has been agreed upon. 2 The interesting report by Lenters-Westra et al. 3 on reference change values (RCV) for HbA1c, based on the results from the Dutch and Belgian External Quality Assessment surveys for HbA1c, in addition illustrates the challenges in handling data from the two similar quantities in parallel. It is, however, not enough to report the two types of HbA1c values in parallel; also, the corresponding measures of imprecision and RCV must be reported specifically for the two quantities.
RCV is the smallest difference between two measurement values that signals a significant change of the quantity. In the article by Lenters-Westra et al. 3 the authors explain in the text under Table 2 that “For clarity of presentation, only Diabetes Control and Complications Trial (DCCT) values are shown.” On the contrary, for clarity it is necessary to show the IFCC values in parallel with the NGSP values, in order to avoid mistakes in data treatment and interpretation.
In their Table 1 the “analytical coefficient of variation” (CV%) achieved from results from various tested methods are presented. It is not stated whether these data refer to HbA1c(NGSP) or to HbA1c(IFCC). As the “CV%” value differs between the NGSP scale and IFCC scale this must be stated in order for the proper interpretation of data.
Based on the master equation (Eq. 1 above) it can be shown that the CV% on the NGSP scale can be transformed to the corresponding value on the IFCC scale with the equation:
As this equation contains the mean HbA1c value it is not possible to convert a “CV% (NGSP)” to a “CV% (IFCC),” or vice versa, without knowledge of the mean HbA1c of the original data set. The mean HbA1c value for the data referred to in the article by Lenters-Westra et al. 3 is not given. Assuming that the given data on imprecision are NGSP-specific and assuming a mean value of HbA1c(NGSP) for the surveys to be approximately 7%, we can roughly convert, for example, an analytical CV%(NGSP) of “3.1” to a corresponding CV%(IFCC) of about “4.5” {7×3.1×10.93/([7×10.93]−23.54)}.
As the relation between the two HbA1c quantities is linear, any difference between two HbA1c(NGSP) values might be converted into a difference in HbA1c(IFCC) values by the following equation:
Also, for changes such as RCV, Eq. 3 should apply, if the changes are expressed as absolute values and not as relative changes. In the example given in the article by Lenters-Westra et al., 3 the RCV is assumed to be 0.5% HbA1c(NGSP), which corresponds to a relative RCV of 7.1% at the HbA1c(NGSP) level of 7.0% HbA1c (100×0.5/7.0=7.1). The RCV in HbA1c(IFCC) units can, from Eq. 3 above, be calculated as 5.5 mmol/mol (0.5×10.93=5.5 mmol/mol), and the relative RCV in HbA1c(IFCC) units is thus 10.3% (100×5.5/53=10.3%). In the article this discrepancy between the IFCC and NGSP scales is not clear.
When the reference interval or other variables derived from the biological variation are known, it is possible to express measurement results in relation to such an interval. This technique can be used to make data for different quantities comparable. As HbA1c(IFCC) and HbA1c(NGSP) values are linearly related, a 25% change of an HbA1c(IFCC) value relative to its reference interval range will correspond to a 25% change of HbA1c(NGSP) value relative to the NGSP reference interval. The same principle can, with some approximation, be applied also for non-linearly related quantities (e.g., when data on analytical variation are compared for the inversely related plasma concentration of creatinine and estimated glomerular filtration rate).
It is a challenge for all engaged to handle results from two quantities in parallel for which the unit is the only difference. Even when the relation between the numerical values of quantities is expressed by a single factor, such as data reported with units “mg/dL” and “g/L,” the situation can be confusing. When the relation between the scales is nonlinear or includes an intercept, which is the case with HbA1c, the conversion of values becomes complicated. Another aspect of the conversion problem is illustrated in a Letter to the Editor of Clinical Chemistry 4 published while this letter was being prepared, addressing the same problem. The analytical goal for HbA1c, expressed as “maximal allowable error,” is taken as an example and stated to be 6.7% for HbA1c(NGSP) and converted to the value 8.6% HbA1c(IFCC). With proper rounding of the figures used for calculation the correct value should rather be 9.4% HbA1c(IFCC).
The best solution to all the problems with reporting HbA1c data is to use only one unit, the IFCC unit, as has been decided and implemented in many countries. Until full uniformity in reporting has been achieved, all professionals, including the scientific journals, must be aware of the necessary steps for proper conversion of data between the two different measurement scales for HbA1c. In addition, older published data on biological variation for HbA1c(NGSP) need to be recalculated after conversion of the values to HbA1c(IFCC) units.