
Abstract
Background:
Gas-filled phospholipid-based ultrasonic microbubbles (PUMs) are widely used in diagnostic imaging. The micro- or nanoparticle size and the physiochemical nature of shell provide the potential for a new way to improve pulmonary absorption for peptides and proteins.
Methods:
Male Sprague–Dawley rats were fasted for 12 h. Then insulin solution and insulin–PUM mixture solution were administered by intratracheal instillation. The hypoglycemic effect was observed to evaluate insulin absorption after lung administration. Fluorescein isothiocyanate–dextran (molecular mass, 4 kDa) was used as the index of evaluating drug alveolar deposition and absorption by visualization techniques.
Results:
Administration of insulin solution containing PUMs significantly reduced the blood glucose levels of Sprague–Dawley rats, compared with administration of insulin-only solution. The minimum reductions of the blood glucose concentration produced by insulin solution containing PUMs and by an insulin-only solution reached 60.81% and 34.60% of the initial glucose levels, respectively, and their bioavailabilities relative to subcutaneous injection were 48.58% and 29.09%, respectively. Histopathological study of the lung showed no changes in the morphology of the pulmonary alveoli after administration to these drugs. Only a slight inflammatory cell infiltration in the alveoli could be found in some rats.
Conclusion:
These results suggested that PUMs might be used as an effective way to improve pulmonary absorption for peptides and proteins.
Introduction
Gas-filled phospholipid-based ultrasonic microbubbles (PUMs) are widely used in diagnostic imaging. Recent developments have greatly enhanced the potential application of PUMs as drug vectors and therapeutic agents. 9 The applications of PUMs as drug or gene delivery systems in various tissues in vivo have been reported, such as cardiac, vascular, skeletal muscle, and tumor. 10 –12 With advantages such as uniform microparticle size, good barrier-penetration effect, and safe material components, PUMs might be used as an effective way to improve pulmonary absorption for peptides and proteins.
Diabetes is a class of diseases characterized by elevated blood sugar in the face of inadequate insulin production or insulin action. Individuals with type 1 diabetes mellitus are dependent on insulin for survival and rely on subcutaneous administration by injection or continuous infusion. 13,14 Such methods of administration are painful to these patients. However, delivery of insulin via inhalation is a potential alternative to subcutaneous insulin in the management of diabetes. 14
Therefore, the aim of this study was to investigate the potential of PUMs to improve insulin pulmonary absorption. The hypoglycemic effect was observed to evaluate insulin absorption after lung administration. Relative bioavailability was evaluated compared with insulin subcutaneous injection.
Fluorescein isothiocyanate (FITC)–dextran with various molecular masses of 4 kDa, 10 kDa, 20 kDa, 40 kDa, and 70kDa have been widely used to assess to the membrane permeability in perfusion studies in animals, internalization of FITC–dextran by suspension cultured plant cells, and the study of fluid pinocytosis in leukocytes. 15 –17 In this study, FITC–dextran with an average molecular mass of 4 kDa was used as the index of evaluating drug alveolar deposition and absorption by visualization techniques.
Materials and Methods
Preparation of PUMs
PUMs were prepared by the sonication–lyophilization method, which was reported in our previous study. 18,19 In brief, preparation was as follows: hydrogenated phosphatidylcholine (>99%) (Doosan Corp. Biotech BU, Kyonggi Do, Korea), polyethylene glycol 1500 (Qingming Chemical Plant, Qingming, Zhejiang Province, China), and poloxamer 188 (Shenyang Chemical Plant, Shenyang, Liaoning Province, China) were dissolved in normal butanol (analytical grade) (Beijing Chemical Plant, Beijing, China) and sonicated at 30°C (model JY 92-II ultrasonic processor, KunShan US Instrument Inc., KunShan, China) at a frequency of 40 kHz and power of 160 W for 3 min. The solution was stored at 0°C for 30 min and at −20°C for 1 h. Then, the coagulated solution was lyophilized at 5×10−4 Pa pressure for 20 h (primary drying at −48°C for 15 h, and then the temperature was gradually raised to 10°C within 5 h). Lyophilized powder was put in 10-mL vials containing penicillin (100 mg per vial) and saturated with perfluoropropane (electronic grade) (Institute of Special Gas, Tianjing, China).
PUM suspension was obtained by dissolving 100 mg of gas-saturated lyophilized powder in 2 mL of physiological saline followed by gentle shaking to form an emulsion-like solution.
Characterization of PUMs
Morphologic characteristics of PUMs were determined using an optical microscope (model YS100, Nikon, Tokyo, Japan). The PUM suspension was gently shaken before one drop was applied to the microscope slide. A coverslip was used to cover the sample before the sample was examined under×200 magnification.
Particle size and concentration of PUM were analyzed on a Coulter counter (Coulter Corp., Hialeah, FL). For each sample, 10–15 μL of PUM solution was analyzed. The Coulter unit aperture was flushed with distilled water before and after use.
Dosage design
Insulin solution
Insulin (Wangbang BioPharma Corp., Jiangsu, China) for injection (40 U/mL) was diluted with physiological saline to the concentration of 2 U/mL.
Insulin solution containing PUMs
PUM suspension was mixed with an equal volume of insulin for injection (4 U/mL). The insulin–PUM mixture solution contained the same concentration of insulin as insulin solution.
Animal experiments
Male Sprague–Dawley rats (weighing 200–300 g) (Slac Laboratory Animal Corp., Shanghai, China) were kept under a 12-h day–night cycle at 20°C and a relative humidity of 50% for 7 days. The animals were fasted but allowed free access to water for 12 h prior to each experiment. The insulin solution and insulin–PUM mixture solution were administered by a modification of the intratracheal instillation procedure of Schanker and Burton. 20 Following anesthesia with intraperitoneal injection of 350 mg/kg chloral hydrate, rats were placed in a supine position on a surgical board. With the rat hanging from the upper incisors, the trachea was subjected to a longitudinal along the ventral aspect of the neck. A needle was gently inserted into the exposed trachea between the fifth and sixth tracheal rings. Then the needle was removed, and a tube was inserted smoothly and rapidly until a slight resistance was felt. After 200–300 μL of insulin solution or insulin–PUM mixture solution followed by an equal volume of air was administered to the lung at the vertical through a pipette directly into the tube (Fig. 1), the tube was removed immediately, and the rat was held gently upright (vertical) by holding his anterior paws and moving them gently. The skin incision of the rats was sutured with a sterile 4/0 silk suture and swabbed with betadine solution. The glucose concentration of blood samples withdrawn from the tail vein at appropriate time intervals was measured with a Pro doctor® blood glucose (BG) monitoring system (HMD BioMedical Inc., Xinpu, Hsinchu, Taiwan). The bioavailability of pulmonary administered insulin was calculated relative to the subcutaneous route. In brief, an insulin solution for subcutaneous injection (1 U/kg) was injected on the nape (back part) of the neck of normal rats in the pulmonary absorption study. These animal experiments were approved by the ethical committee for treatment of laboratory animals of Wenzhou Medical College (Wenzhou, Zhejiang Province, China).
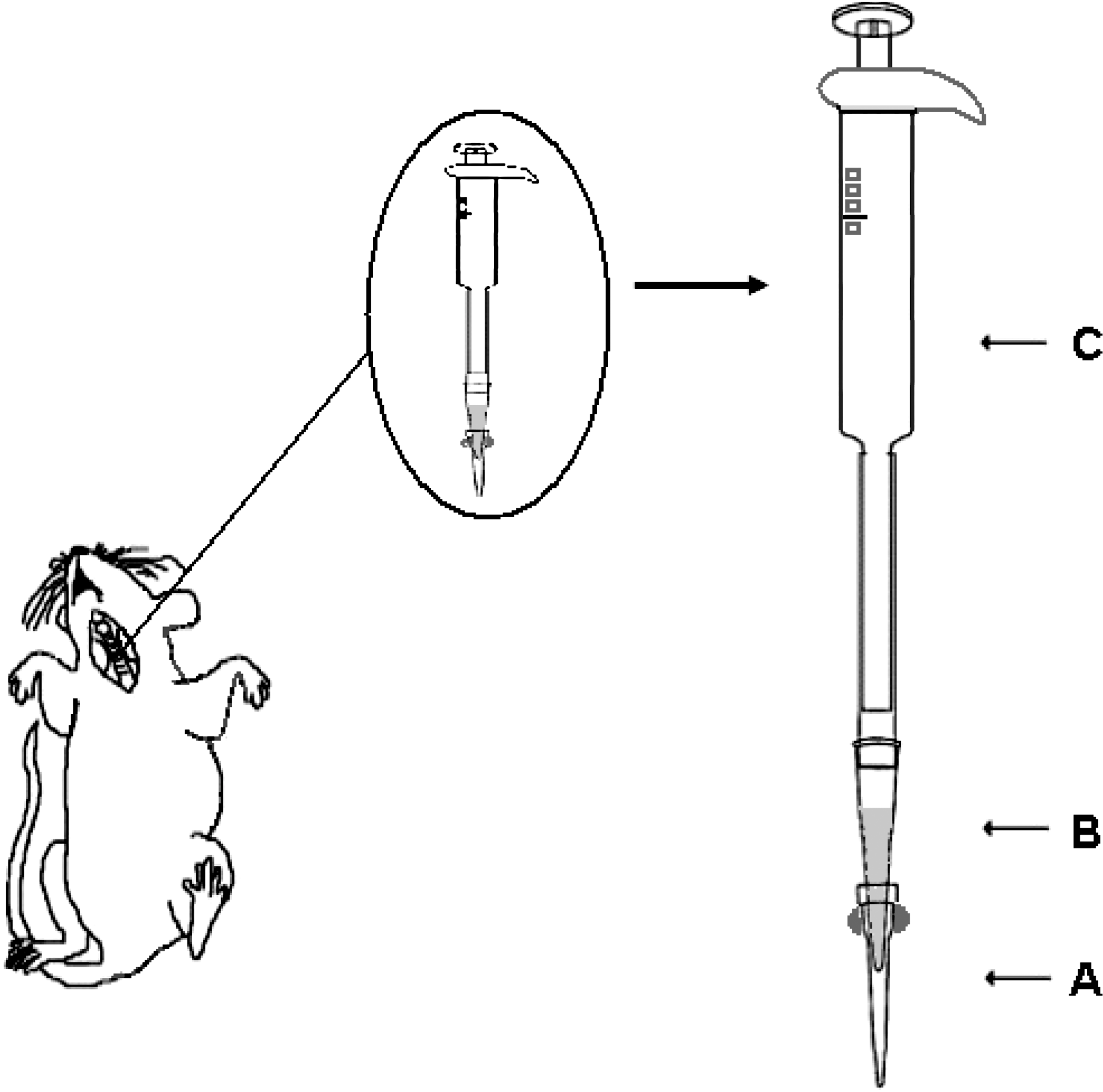
Administration by intratracheal instillation and apparatus: (
Data analysis
To estimate pulmonary absorption of insulin, the BG concentration was measured with the Pro doctor BG monitoring system at the indicated time intervals. The percentage minimum reduction of the BG concentration (%MRBG) at the time of maximum glucose reduction was derived directly from the each group's BG level. The percentage BG level was calculated from the equation
where BG0 is the fasting BG level at zero-time and BG
t
is the BG level at any time t.
21
The decrease in the BG concentration (D%) was calculated by the method of Leng
22
with the following equation:
where AUC0→12h is the area under the curve (AUC) of D% for 12 h and was calculated by the linear trapezoidal rule.
The bioavailability relative to subcutaneous injection (F) was calculated by a modification of the method of Lim et al.:
7
Alveolar deposition and absorption of FITC–dextran
To assess the alveolar deposition of the administration manner, 280 μL of FITC–dextran (average molecular mass, 4 kDa) (Sigma, St. Louis, MO) (25 mg/mL in physiological saline with an equal volume of PUMs) followed by an equal volume of air was injected into lungs by a similar administration manner as for the insulin–PUM mixture solution. Immediately after the FITC–dextran was given, the lungs were excised and observed with an ultraviolet transmission instrument (model ZF-90, Shanghai Light Equipment Inc., Shanghai). After that, the right lung was separated into three lobes (upper, middle, and lower), and the left lung was divided into two lobes (upper and lower) equally at the middle point of the long axis. Each lung was homogenized in 2 mL of physiological saline and centrifuged at 3,000 g for 15 min. Then the fluorescence intensity in the supernatant was measured using the enzyme-linked immunosorbent assay method at excitation and emission wavelengths of 500 and 520 nm, respectively. The FITC–dextran content of each lobe was calculated, to estimate the FITC–dextran deposition ratio. 20 –22
To assess whether PUMs enhanced the drug pulmonary absorption through intratracheal instillation into the systemic circulation, 280 μL of FITC–dextran solution and FITC–dextran with PUM mixture solution were injected as described previously at 15 min, 1 h, 3 h, 6 h, and 12 h before lung harvest in each rat, respectively. The fluorescence intensity of FITC–dextran in blood serum was measured using the enzyme-linked immunosorbent assay method under similar conditions as described above.
Histopathological study
At necropsy, the lungs were removed from each animal. The lung was perfused with 10% neutral-buffered formalin via the trachea and immersed in the same fixative for 72 h. Specimens were collected from the anterior and posterior regions of the left lung (two specimens per rat) of all the animals. Using the standard method, these specimens were paraffin-embedded and cut into thin sections. Thereafter, these sections were stained with hematoxylin and eosin. 23
Statistical analysis
Statistically significant differences for multiple groups were determined using a one-way analysis of variance with a Newman–Keuls post test. Statistical significance between individual group was determined using a Student's t test. All testing was done using SAS version 8.01 software (1999–2000, SAS Institute Inc., Cary, NC). The difference in data was considered to be statistically significant when the P value was <0.05.
Results and Discussion
Size distribution and morphology of PUMs
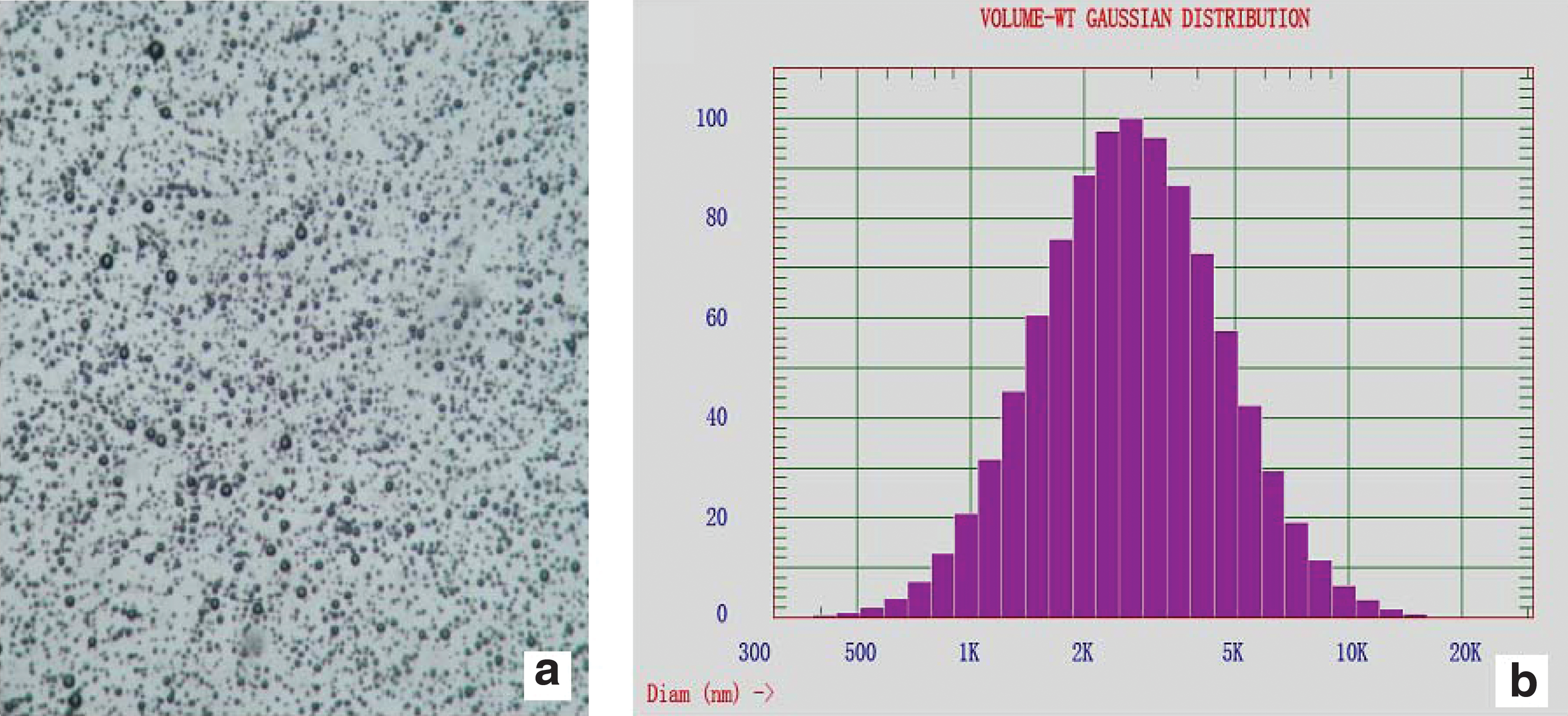
Figure 2 shows the morphology and particle size distribution of PUMs. Figure 2a is an example of morphology of PUMs observed by optical microscopy. All PUMs remained distinct in shape, and no aggregation or fusion was observed. Little change was observed between blank PUM solution and insulin–PUM mixture solution. As shown in Figure 2b, PUM size distribution profile showed a narrow Gaussian distribution, with an average diameter of 2.7 μm. Almost 90% of the PUMs were in the diameter range of 1–5 μm, which showed the potential in pulmonary delivery. (The ideal size for pulmonary delivery of particles into the deep lung region is between 1 and 5 μm in geometric diameter. 24 )
(
Animal experiments on BG level
D% following intrapulmonary administration of insulin and insulin–PUM mixture solution (2 U/kg) and of insulin solution by subcutaneous injection (1 U/kg) is shown in Figure 3, which directly represented the speed and degree of the hypoglycemia effect. From Figure 3 it can be seen that the hypoglycemic effect of subcutaneous insulin solution (1 U/kg) was stronger than those of pulmonary administrations, which agrees with previous reports. 7,21,22,25 Insulin bioavailability after pulmonary administration of insulin only was 29.09%, which was about twofold higher than that in the previous research. 7 The difference between insulin bioavailability in our experiment and in previous research might be ascribed to different sources of insulin used in the test. With various insulin sources, the titer might be different for the hypoglycemic effect. Among the different insulin pulmonary administration groups, the insulin–PUM mixture solution showed the best effect in decreasing the BG level. Also, its bioavailability (48.58%) was much higher than that of insulin solution alone and was statistically significant (P<0.01).
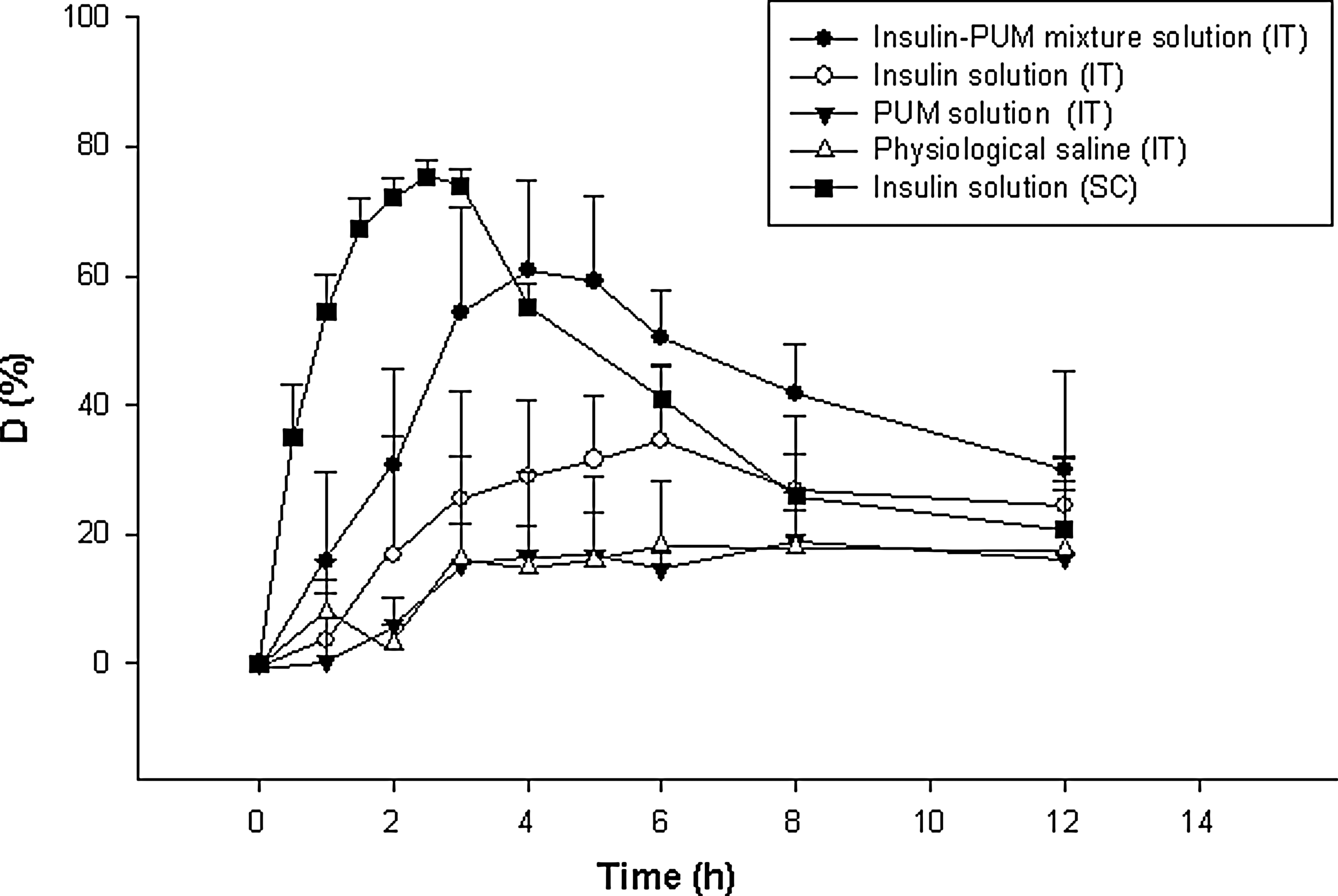
The percentage decrease in blood glucose concentration (D [%]) after intratracheal delivery (IT) and subcutaneous injection (SC) of insulin with phospholipid-based ultrasonic microbubbles (PUMs) and insulin solution. Insulin–PUM mixture solution by IT 2 U/kg (•), insulin solution by IT 2 U/kg (○), and insulin solution by SC 1 U/kg (▪) (n=7) were administered. Equivalent doses of physiological saline (▵) and empty PUM solution (▾) by IT were used as control groups (n=7). Data are mean±SD relative values of the initial glucose concentration. The decrease of blood glucose concentration corresponded to the blood glucose levels.
Values of pharmacodynamic parameters are listed in Table 1. The BG levels in the rats with each treatment decreased with time and reached minimum values at the following time points: 4 h (intratracheal insulin–PUM mixture solution) for percentage of minimum BG concentration (%MBGC) (39.19%), 6 h (intratracheal insulin solution) for %MBGC (65.40%), and 2.5 h (subcutaneous insulin solution) for %MBGC (24.68%). The %MRBG produced by the insulin–PUM mixture solution (60.81%) was greater than that by insulin solution (34.60%) for the initial glucose levels with pulmonary administration (Table 1). Comparison of the %MBGC of intratracheal insulin solution (65.40%) with that of the control group treated with intratracheal physiological saline (77.07%) and empty PUM solution (79.26%) at 6 h, the time that intratracheal insulin solution took to attain the %MBGC, showed that insulin solution administered by intratracheal instillation could reduce the BG concentration of normal rats, but its %MBGC was much higher than that with treatment by insulin–PUM mixture solution (P<0.01). These results showed that PUM could increase the uptake rate and the quantity of insulin for pulmonary absorption and agreed with the conclusion reported in previous experiments 7,21,22,25 that the profile of BG concentration by pulmonary administration could be very similar to that by subcutaneous injection administration. Because animals were fasted for 12 h before experimentation, their BG levels were low. With experiments lasting for 12 h, glycopenia appeared in most animals, as demonstrated by the decrease in BG concentration in both the PUM solution group and the physiological saline group shown in Figure 3.
Data are mean±SD values (n=7).
Statistical significance: * P<0.05; ** P<0.01.
AUC, area under the curve; F, bioavailability relative to subcutaneous injection; IT, intratracheal instillation delivery; MRBG, minimum reduction of blood glucose concentration; MBGC, minimum blood glucose concentration; PUM, phospholipid-based ultrasonic microbubbles; SC, subcutaneous injection; T%MRGB, time required to attain %MRGB.
Alveolar deposition and absorption of FITC–dextran
Visualization of FITC–dextran in lung distribution could offer the direct demonstration of drug alveolar deposition. Figure 4 shows the change in total FITC–dextran deposition in lungs with interval after treatment of rats. The total intensity and distribution area of fluorescence in lung increased at first and then decreased. Fluorescence intensity in lung lobes was highest at 15 min, while some FITC–dextran solution was retained in the trachea following observation. Although lobe fluorescence intensity began to decline at 3 h, the FITC–dextran distribution area of lung was enlarged. As shown in Table 2, the result of FITC–dextran deposition in each lobe of lung was consistent with previous reports. 26,27 Following intratracheal instillation, the distribution rate of various lobes was not regular. The position and the depth of needle insertion into the exposed trachea, the interval of the rats were held upright, the speed of drug solution injection, the intervention of the operation, and individual animal differences might be factors producing different alveolar deposition of FITC–dextran following intrapulmonary administration.
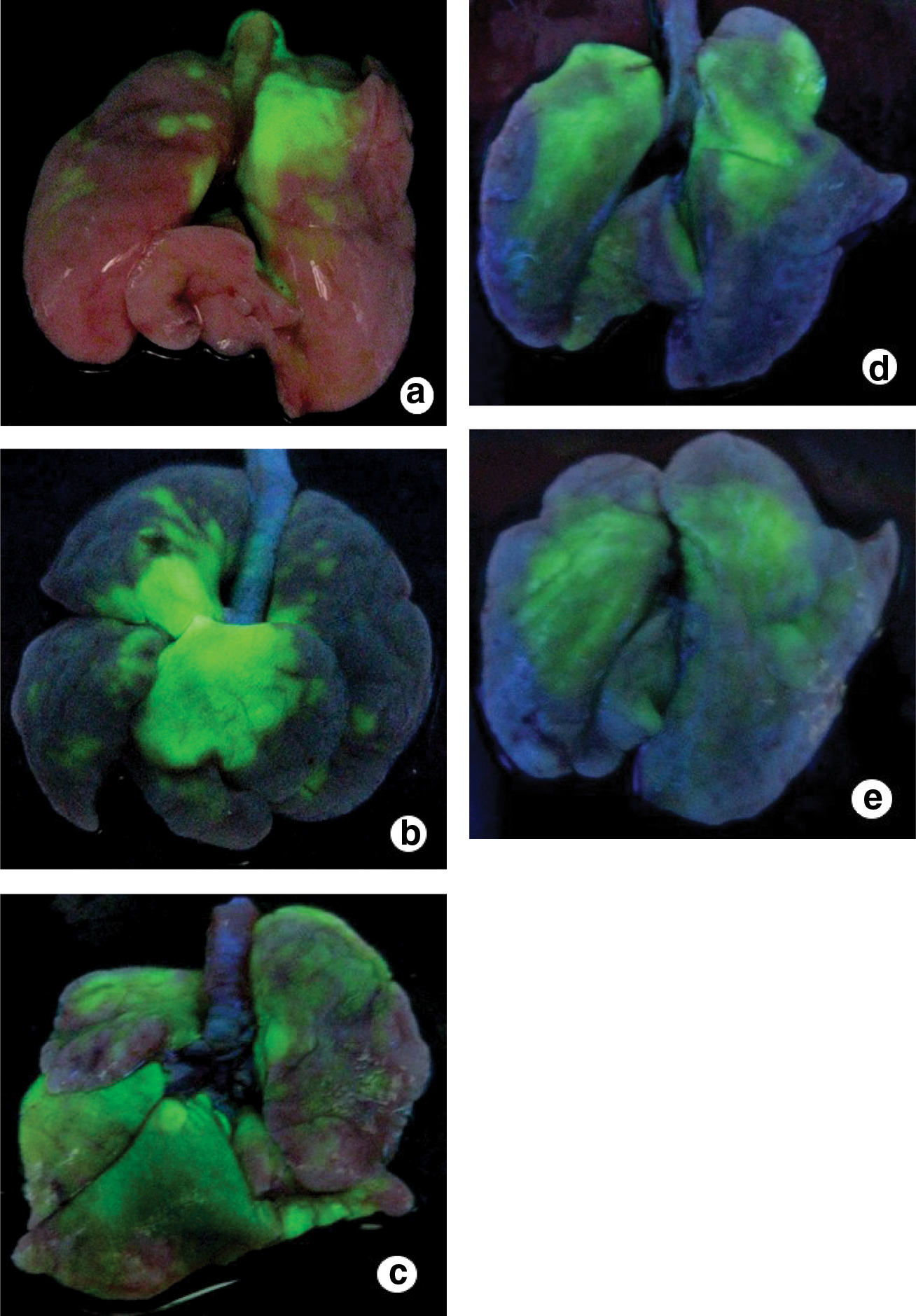
Photographs of the change of fluorescence in rat lung depending on the time interval after administration by intratracheal instillation of the hydrophilic fluorescence probe fluorescein isothiocyanate–dextran mixed with phospholipid-based ultrasonic microbubbles in solution. Rat lungs were harvested (
Data are relative amount of fluorescein isothiocyanate–dextran delivered to each lobe, expressed as a percentage of the sum of the right and left lungs.
Recovery rate expressed as a percentage of the initial dose.
After FITC–dextran was administered by the intrapulmonary route, it was absorbed into systemic circulation from the lung. The fluorescence intensity of FITC–dextran in blood serum measured with the enzyme-linked immunosorbent assay method showed the speed and extent of drug pulmonary absorption. As shown in Figure 5, the ratio of FITC–dextran deposited in lung and in serum showed a declining trend with increasing time after administration. The profile showed that drug was absorbed from the lung into the systemic circulation. Based on the results, PUMs could enhance lung–blood barrier penetration for FITC–dextran and therefore reduced the ratio of FITC–dextran deposited in lung and in serum. The ratio of FITC–dextran deposited in lung and in serum decreased to minimum value at 6 h in both two FITC–dextran treatment groups.

Ratio of fluorescein isothiocyanate (FITC)–dextran deposited in lung and in serum from FITC–dextran solution and FITC-dextran with phospholipid-based ultrasonic microbubbles in solution following intrapulmonary administration. Data represent the values of fluorescence intensity in lung and serum at the same point time read with the enzyme-linked immunosorbent assay.
Assay of pathological changes
From our experiment mentioned above, PUM and insulin mixture solution was shown to be effective in promoting insulin pulmonary absorption. To clarify the local toxicity of PUMs that were administered to rats in a single intratracheal instillation, lung lesions were observed at 1–7 days after administration and were evaluated histopathologically. The micrographs (Fig. 6) showed no apparent histological damage in insulin–PUM-treated animals compared with normal (control) animals. The morphology of lung tissues was not observed to be abnormal, and the alveolar walls were all very thin with normal alveolar spaces. Severe lung lesions like a severe pulmonary inflammatory response with diffuse alveolar and bronchiolar cell hyperplasia and with interstitial fibrotic proliferation were not observed in our experimental sections. These lung lesions were found in a previous report 28 that surface-active agents like polyoxyethylene 9 laurylether (Laureth-9) or sodium glycocholate could induce lung injury from a single intratracheal instillation. From the following photomicrographs, the following process of lung response to PUM solution could be proposed: inflammation, alveolar cell hyperplasia, and alveolar macrophage infiltration to alveolar spaces were observed first at 5 days. Then the both the alveolar and bronchiolar epithelium recovered to a normal appearance at 7 days. These results suggested that one single dose of PUMs with insulin mixture for pulmonary delivery was relatively safe.
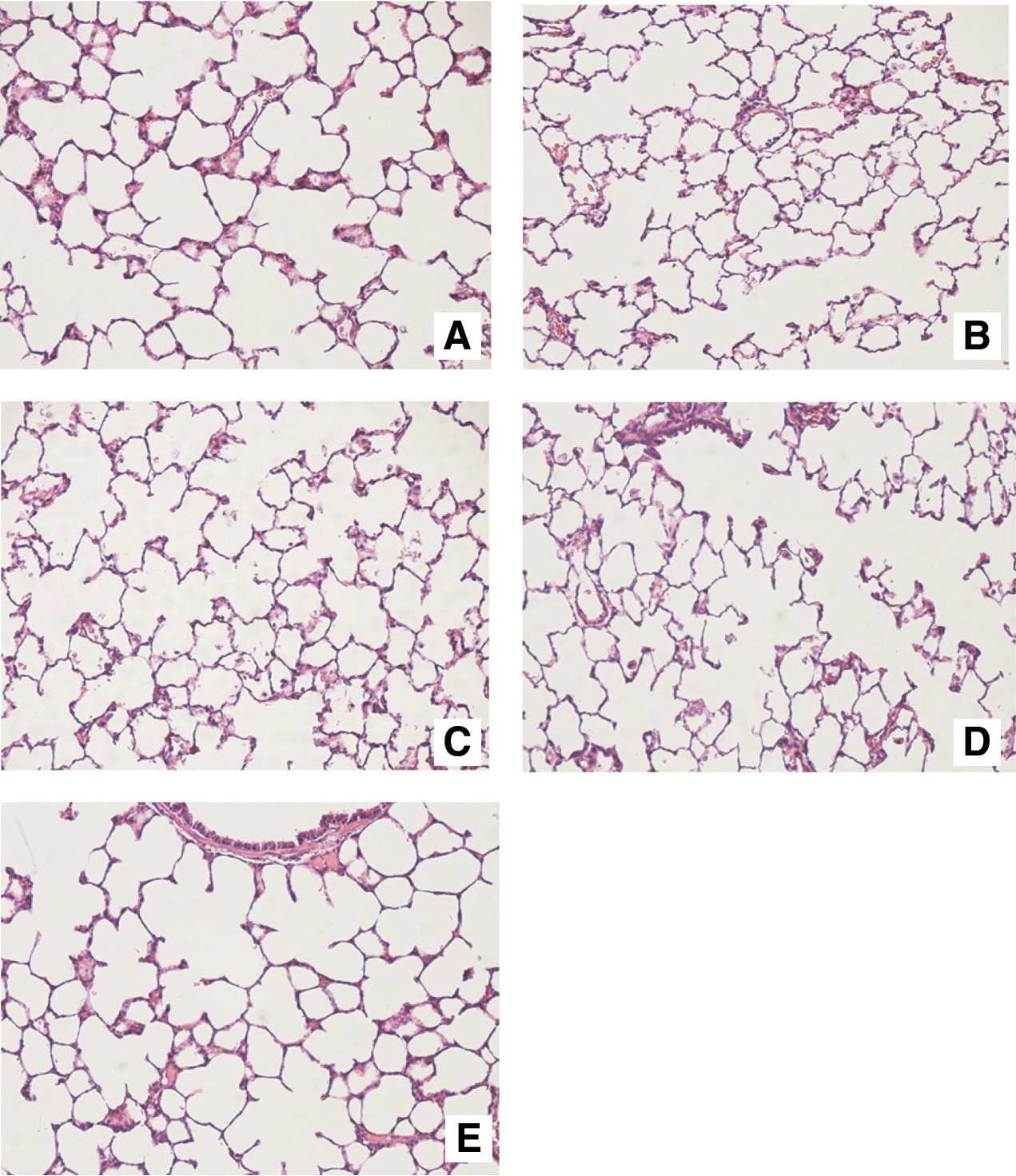
Photomicrographs of the lung showing inflammatory changes after a single intratracheal instillation of insulin–phospholipid-based ultrasonic microbubbles in solution. (
Hypoglycemia
Treatment strategies aimed at achieving euglycemia carry the risk of increased number and severity of hypoglycemic events. 29 There have been no adverse effects uniquely associated with a specific insulin formulation or delivery device of intrapulmonary administration. 14 Hypoglycemia was the major problem, which should be avoided in insulin treatment in both type 1 and type 2 diabetes mellitus populations. The inhaled insulin formulation carries less risk of severe hypoglycemia compared with subcutaneous insulin and increased risk in insulin-naive patients. 14 Therefore, the safe dosage range must be determined in order for patients to receive the appropriate amount of insulin to avoid hypoglycemia happening. In this study, we found that insulin with PUMs in the dose of 2 U/kg following intrapulmonary administration by intratracheal instillation was the correct dosage, producing a minimum BG value of 1.9 mmol/L. With an increase in the amount of insulin, symptoms associated with hypoglycemia, including tremor, sweating, and headache, appeared. When the dose of insulin reached 8 U/kg, hypoglycemia became worse, and severe hypoglycemia occurred that led to seizures, coma, and even death. The mortality after pulmonary administration of insulin–PUMs in solution (8 U/kg) was very high (67.7%). Lung injury following a large dose of insulin administered by intratracheal instillation showed severe hemorrhage (Fig. 7A and B).

Severe hypoglycemia caused the death of an experimentally treated rat compared with a normal one. (
Mechanisms of PUMs enhancing pulmonary absorption of insulin
Results in this article showed that PUMs could improve the insulin pulmonary absorption markedly and make insulin pulmonary administration relatively safe. Although the reason was not clear, we tried to explore the mechanisms of PUMs enhancing pulmonary absorption of insulin. Based on the physics of the gas-filled PUM structure, the change of intrapulmonary pressure induced by respiratory movement might cause PUMs to oscillate, rupturing or rapidly reducing the volume until complete ablation. All these actions could increase the permeability of pulmonary epithelial cells and endothelial vasculature, which might enhance the entrance of insulin molecules into systemic circulation from the lung. Previous research showed that microbubbles oscillating near a cell membrane surface can cause hyperpolarization of the membrane, which may promote endocytosis of external macromolecules. 30
Lipid-coated PUMs with the lipid shell and gas core were bioinspired, as are the remarkable stability and compliance of lung surfactant. Lung surfactant was discovered based on the observation of stable PUMs formed from lung lavage. 31 Furthermore, the ability of lung-derived fluid to form stable PUMs is being pursued as a clinical means of assessing lung surfactant viability in neonates. 32 The PUM was the structure of lipid monolayer in which the hydrophobic acyl chains faced the gas and the hydrophilic headgroups faced the water. The high biocompatibility of PUMs with the lung showed their safe potential for drug intrapulmonary delivery.
The detailed and definite mechanisms of how PUMs improve the insulin macromolecule and why PUMs are relative safe for pulmonary administration will be examined in our subsequent work.
Conclusions
In this article, experiment was designed to investigate using PUMs to enhance drug pulmonary absorption. PUMs had a homogeneous spherical shape, with an average diameter of 2.7 μm and a narrow, monodispersed size distribution. A satisfactory mixing of insulin with PUMs was observed with high concentration of PUMs (8.36×107/mL). After administration of the insulin with PUMs to normal Sprague–Dawley rats by intratracheal instillation, BG levels were significantly reduced. The bioavailability of insulin administered by the intrapulmonary route with PUMs (48.58%) relative to subcutaneous injection was much higher than that of insulin solution (29.09%). Based on these inspiring results, further work will be carried out to investigate intrapulmonary administration of insulin combined with PUMs using large animals and protein analysis. 33
From these results, insulin combined with PUMs can enhance the speed and extent of insulin pulmonary absorption. The use of new PUM-mediated peptide/protein drugs with intrapulmonary administration was recommended, which might become an important therapeutic tool for lung delivery.
Footnotes
Acknowledgments
This research was supported by the National Natural Science Funds (grants 81071164 and 81071277), the Natural Science Foundation of Zhejiang Province (grants Y2110587 and Y2080915), the Natural Science Foundation of Beijing (grant 7112100), Medicine and Health Grants from the Wenzhou Bureau of Science and Technology (grants H20100017 and S20100049), and funds from the Zhejiang Province Health Department (grants 2009QN022, 2010ZQ007, and 2011ZDA017) and Zhejiang Province Education Department (grant Y201016664).
Author Disclosure Statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the article.