
Abstract
Background:
Self-monitoring of blood glucose (SMBG) is a simple tool to monitor the effects of lifestyle change on blood glucose. Recently, the ROSSO-in-praxi Study demonstrated that addition of SMBG to a 12-week lifestyle intervention was associated with significant improvements in glucometabolic control and quality of life in insulin-naive patients with type 2 diabetes mellitus (T2DM). So far it is unknown if this short-term intervention also has long-term effects. Therefore, participants were followed up for a mean period of 2 years.
Methods:
Participants (n=327) were asked by mail for current weight, hemoglobin A1c (HbA1c), performance of SMBG, and quality of life (SF36 and CES-D questionnaires). Participants who did not reply were contacted by phone.
Results:
Two hundred twenty-eight participants (70%) completed the follow-up. During the 12-week lifestyle intervention they had significantly reduced weight (2.2 kg) and HbA1c (0.3%; P<0.001 each). After 2 years they achieved a further reduction of weight (0.2 kg; P<0.001), whereas HbA1c increased again, remaining 0.1% lower than baseline. The numbers of depressed participants remained stable during follow-up, whereas physical and mental health-related quality of life remained better compared with baseline. During follow-up 20% of participants continued SMBG daily, 35% several times a week, and 33% irregularly. It is interesting that participants with daily SMBG demonstrated an HbA1c decrease of 0.3% at time of follow-up, whereas in those who stopped SMBG HbA1c increased by 0.1% (P=0.05).
Conclusions:
Integration of a short-term, motivational, and low-cost intervention into basic therapy of T2DM has had beneficial long-term effects on weight and quality of life and, if SMBG was continued daily, also on HbA1c.
Introduction
Recently, we developed a short-term, highly motivational but low-cost program: 10 the SMBG-structured 12-week lifestyle guidance ROSSO-in-praxi demonstrated a significant and clinically relevant improvement of glucometabolic control (e.g., HbA1c reduction of 0.3%) and other cardiometabolic risk factors combined with a significant improvement in quality of life. So far it is unknown if such a short-term intervention also has long-term effects. Therefore, study participants were followed for a mean period of 2 years, and performance of SMBG, body weight, HbA1c, and quality of life were assessed again.
An abstract containing the data of this article had been presented as a poster at the 46th annual conference of the Deutsche Diabetes Gesellschaft, and an abstract has been published. 11
Subjects and Methods
SMBG-structured 12-week lifestyle intervention
Study population and content of the SMBG-structured 12-week lifestyle intervention had been described before. 10 In brief, patients with T2DM, duration of diabetes of ≤5 years, ≤75 years old, with a body mass index (BMI) of ≥27 kg/m2, treated with diet or oral antidiabetes medication but not insulin, and who had no experience with SMBG were included in the study. The study was performed according to the rules of the Declaration of Helsinki, and all participants gave informed written consent. Participants (n=405) were sent a manual with basic information about healthy diet and physical activity, a tape for measuring waist circumference, a step counter, and a blood glucose meter with 100 test strips (Accu-Chek® Aviva system, Roche Diagnostics, Mannheim, Germany). Blood glucose diurnal profile and event-driven measurements had to be performed. The participants were motivated to draw their own conclusions from the SMBG results and to modify their daily habits. The manual offered guidance, how to change eating habits, and how to react to elevated blood glucose levels with physical activity. The participants were not instructed to change their antidiabetes medication. At baseline and at the end of intervention weight, waist circumference, HbA1c, blood pressure, and lipid levels were measured by the treating physician. Physical and mental health–related quality of life was estimated using the validated SF36 questionnaire. 12 As depression often occurs in patients with T2DM, depression was estimated by self-assessment using the German version (ADS-L; “Allgemeine Depressionsskala”) of the validated CES-D questionnaire. 13 Depression was defined to be present at a score >23.
Follow-up after 2 years
After 2 years, participants were contacted again. They were sent the SF36 and CES-D questionnaires and asked for information about their SMBG performance and current weight and HbA1c. Questionnaires were sent out in September 2010. Participants who did not reply by the end of October were contacted by phone and asked to send the questionnaires.
Statistical analysis
Differences between data at “baseline” and “end of intervention” were compared using the Wilcoxon signed-rank test. In the intention-to-treat analysis Wilcoxon matched-pairs test was used to compare baseline values from all patients with follow-up data from those participants who completed the follow-up. For the completers analysis, analysis of variance (the Friedman test plus Dunn's multiple comparison test) was used. Dichotomous variables were compared by Fisher's exact and χ 2 tests. Stratified analyses according to SMBG categories had been determined using the Mann–Whitney test. In order to analyze parameters that account for HbA1c reduction logistic regression analysis had been performed. The level of significance was 0.05. Data are mean±SEM values. For data analysis GraphPad Prism version 4.0 (GraphPad Software, San Diego, CA) and SAS statistical package version 8.2 TS2MO (SAS Institute, Cary, NC) were used.
Results
Baseline parameters of study recruits, 12-week intervention completers, and follow-up completers
From the recruited population (n=405) a total of 327 participants completed the 12-week lifestyle intervention. Participants who dropped out did not significantly differ from the study population regarding glucometabolic parameters and cardiovascular risk factors (data not shown). Only those participants who completed the whole program (n=327) were invited to fill in the follow-up questionnaires after 2 years. Of these, 228 (70%) replied and completed the follow-up, whereas 99 (30%) were lost-to-follow-up (Fig. 1). Baseline parameters of those participants who had been originally recruited for the study (n=405), those who completed the 12-week intervention period (n=327), and those for whom follow-up data were available (n=228) are nearly identical (Table 1). The only significant difference was longer duration of diabetes in the “follow-up” group compared with the “recruited” group (2.1±1.5 vs. 2.0±1.5 years; P=0.02). Therefore, it seems that there was no special selection for both the group of participants who completed the intervention period as well as those who completed the follow-up. As demonstrated by the analysis of the 12-week lifestyle intervention, 10 participants who completed the 12-week program (n=327) significantly reduced their mean weight (P<0.0001), BMI (P<0.0001), and waist circumference (P<0.0001). These improvements led to a significant reduction of HbA1c by 0.3% (P<0.0001), systolic (P=0.0006) and diastolic (P=0.002) blood pressure, and low-density lipoprotein cholesterol (P=0.0007).
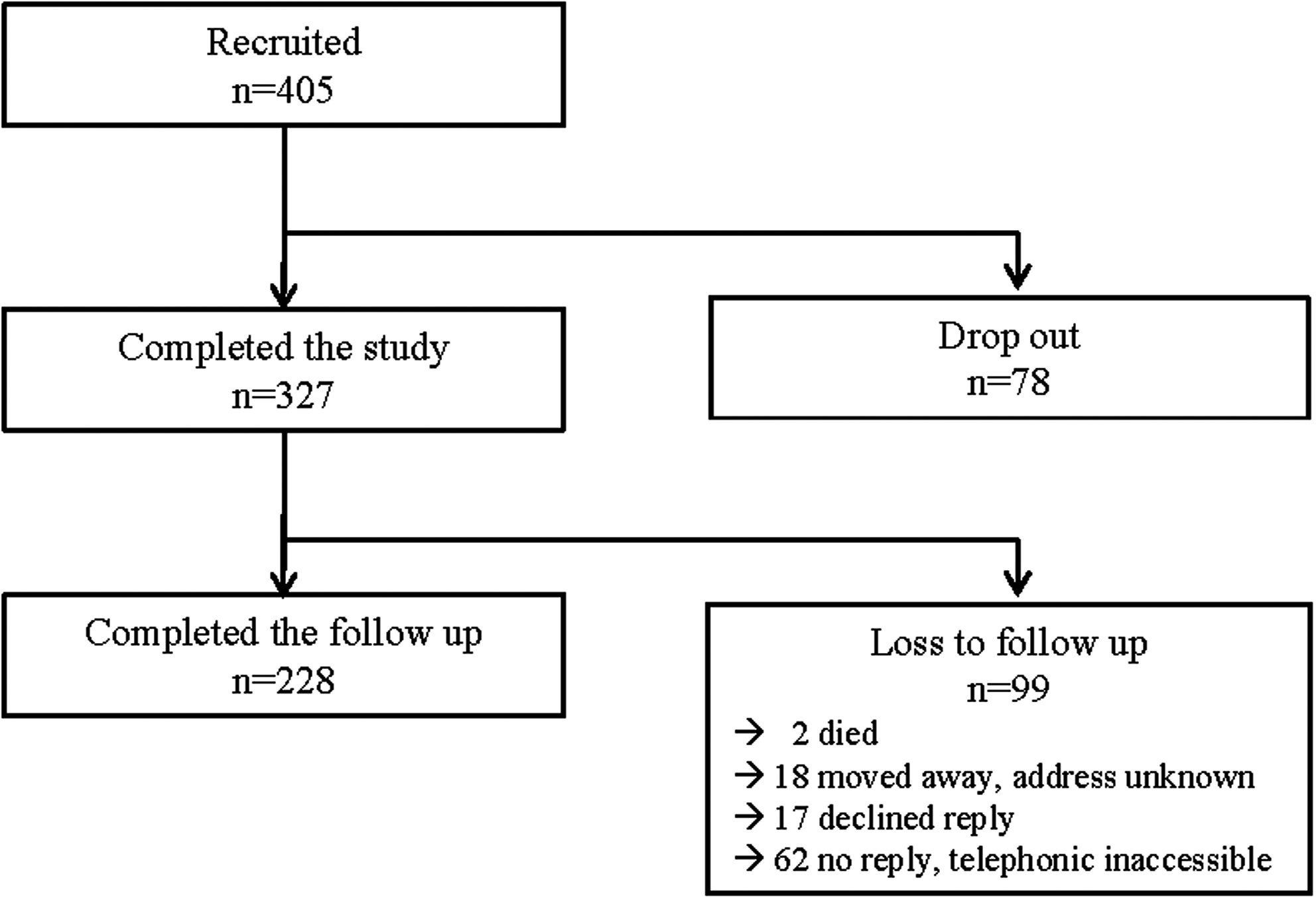
Flow chart for ROSSO-in-praxi follow-up.
Data are mean±SD values. Dichotomous variables were analyzed by χ 2 test. Wilcoxon matched-pairs test was used to analyze differences between baseline parameters (* P<0.05).
BMI, body mass index; BP, blood pressure; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Improvements in weight and BMI could be maintained during 2 years of follow-up
The participants with complete follow-up (n=228) consisted of 91 men (40%) and 137 women (60%) with a mean age of 59.8±8.6 years and a mean duration of diabetes of 2.1±1.5 years. During the intervention they had been able to continuously reduce their weight and BMI with a mean reduction of 2.2 kg and 0.6 kg/m2, respectively, in total (from 92.6±16.3 to 90.4±15.9 kg and from 32.3±5.3 to 31.7±5.3 kg/m2, respectively). During the 2 years of follow-up participants were able to maintain this weight loss and BMI reduction, ending up with a mean weight of 90.2±15.7 kg (−2.4 kg vs. baseline; P<0.001; Fig. 2A) and a mean BMI of 31.5±5.1 kg/m2 (−0.8 kg/m2 vs. baseline; P<0.001; Fig. 2B). During the 12 weeks of intervention participants were able to reduce their HbA1c by a mean of 0.3% (from 6.7±1.0% to 6.4±0.7%; P<0.001). During the follow-up time period an increase of 0.2% was observed, leading to a final mean HbA1c of 6.6±0.8% (P=0.06 vs. baseline; Fig. 2C).
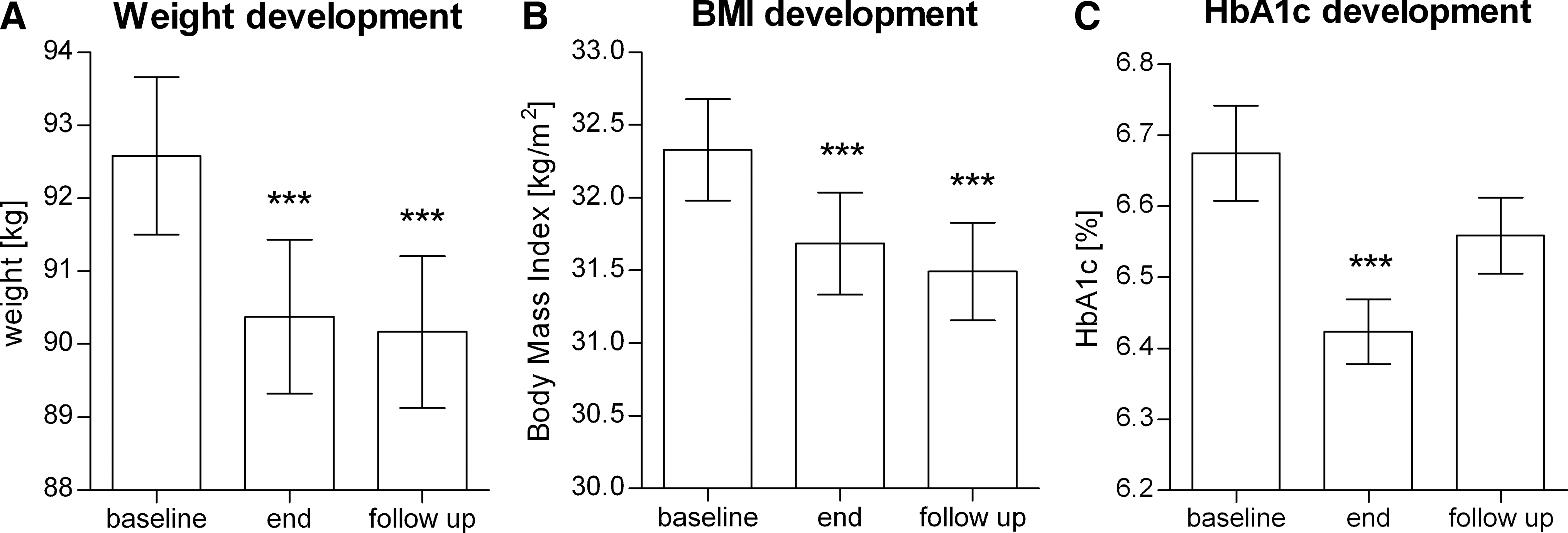
Development of
Improvements in mental health–related quality of life could be maintained during 2 years of follow-up
Self-assessment of physical (Fig. 3A) and mental (Fig. 3B) health–related quality of life using the validated SF36 questionnaire demonstrated a significant increase on the respective scores during the intervention (P<0.001 each). Although the achieved improvements in physical health could not be maintained during follow-up, the mental health–related quality of life remained significantly better compared with the baseline value (P<0.05). The percentage of T2DM patients with depression measured using the validated CES-D questionnaire had been low at baseline (n=18; 7.9%) and remained stable over time with n=11 (4.8%) at the end of the 12-week lifestyle intervention and n=16 (7.0%) at time of follow-up (Fig. 3C). We found no significant correlation between SMBG performance and depression or quality of life.

Development of (
Participants who continued SMBG daily maintained improvements in HbA1c
After the 2-year follow-up period participants were asked about SMBG frequency. Twenty percent continued to measure their blood glucose daily, with a mean of 2.0±1.0 measurements/day. Thirty-five percent measured several times a week, with a mean of 2.3±2.2 measurements per week. Thirty-three percent continued to use SMBG irregularly as needed, and 12% did not perform SMBG any longer. In total, 88% of participants continued to perform SMBG, and only 12% did not. According to those four categories of SMBG performance, a stratified analysis was used to analyze the HbA1c reduction between “baseline” and “follow-up.” Compared with the baseline values, participants who measure their blood glucose daily demonstrated an overall HbA1c reduction of 0.28±1.21% on average at the end of follow-up. Participants who measured several times a week or performed SMBG irregularly showed a nearly constant HbA1c with slight reductions of 0.11±0.68% and 0.09±0.70%, respectively. In contrast, those participants who discontinued SMBG demonstrated a marginal increase in HbA1c of 0.07±1.19%. A comparison of those groups with daily or no performance of SMBG demonstrated a borderline significant upward tendency (P=0.05) in HbA1c development (Fig. 4). Such a trend, although also not statistically significant, was also seen for weight development (baseline vs. follow-up) with highest weight loss in the group with daily blood glucose control (−3.3±10.8 kg) and lowest in those who stopped SMBG (−1.8±5.3 kg; data not shown).
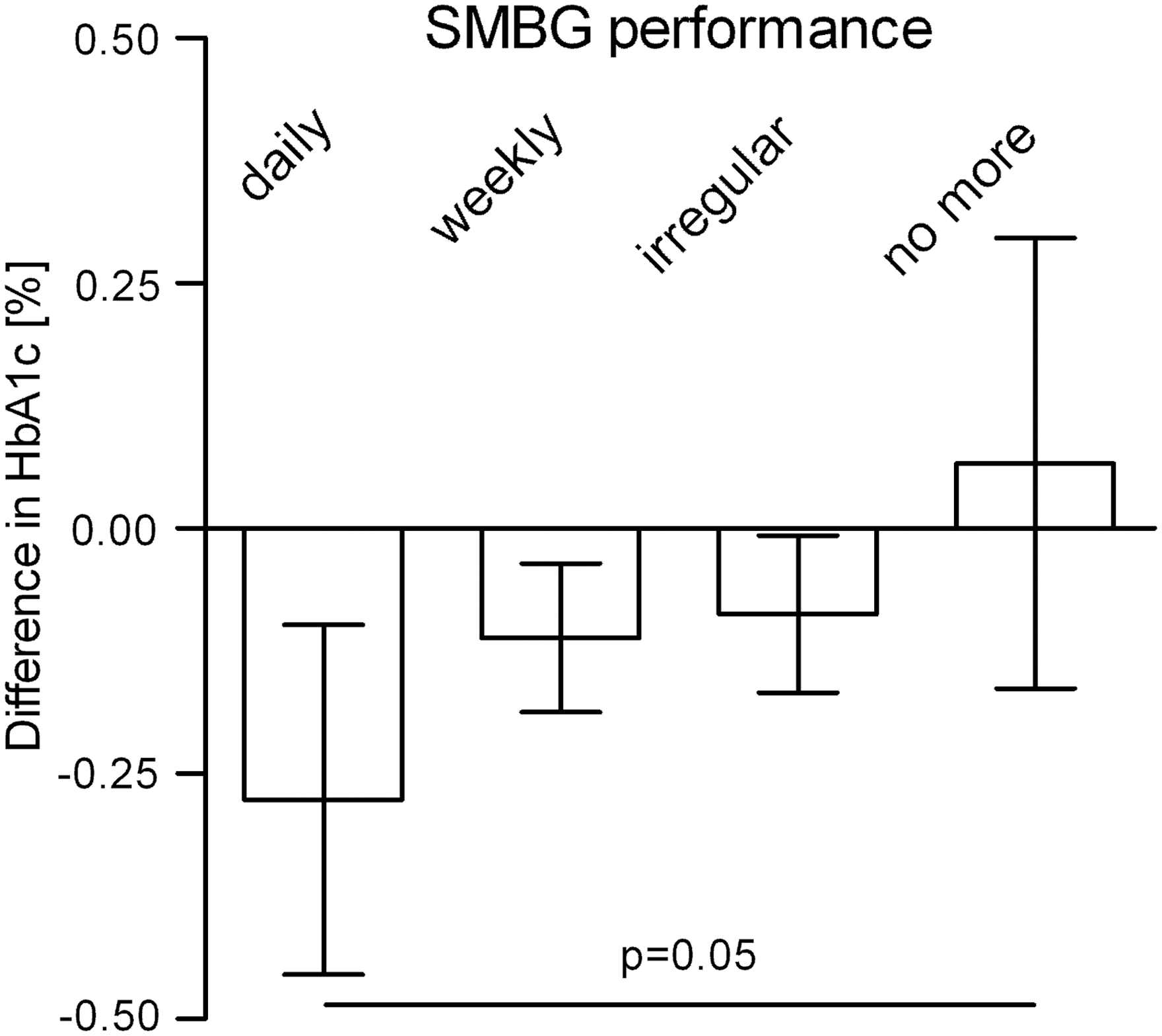
Performance of self-monitoring of blood glucose (SMBG) and hemoglobin A1c (HbA1c) development. HbA1c development at “baseline” versus “follow-up” is shown for the four SMBG performance categories “daily” (n=46), “weekly” (n=79), “irregular” (n=76), and “no more” (n=27), and differences between groups (“daily” vs. “no more”) were determined using the Mann–Whitney test.
Weight reduction accounts for decrease in HbA1c
Formerly, successful participation in the SMBG-structured lifestyle intervention was defined by weight reduction. 10 Therefore, we analyzed again if maintenance of weight reduction until 2-year follow-up also is associated with reduction of HbA1c. In total, 140 out of 228 participants (61.4%) maintained a weight loss of at least 0.5 kg 2 years after the end of intervention. In 31 participants (13.6%) weight remained stable, and 57 participants (25.0%) reported an increase in weight of at least 0.5 kg. We performed logistic regression analysis, which demonstrated that weight reduction was significantly associated with HbA1c reduction. Indeed, weight reduction (odds ratio 0.90 [0.84–0.97]) was the only explanatory variable for HbA1c reduction after adjustment for sex, age, SMBG performance, and quality of life. Moreover, participants who could not maintain weight loss had HbA1c comparable to baseline values, a weight loss of 0.5–5.0 kg went along with a decrease of 0.1% in HbA1c, and weight reduction of >5.0 kg was associated with an improvement of 0.3%.
Discussion
ROSSO-in-praxi is a 12-week lifestyle intervention for patients with T2DM that was developed to evaluate the impact of an SBMG-structured handbook-based lifestyle intervention program on glucometabolic and general health parameters, with weight and HbA1c reduction as main outcome variables. Three hundred twenty-seven participants completed the 12 weeks of lifestyle intervention and showed significant weight loss, HbA1c reduction, and improvement of quality of life. After the end of the 12-week lifestyle intervention participants were followed up for 2 years. Two hundred twenty-eight (70%) participants completed the follow-up and demonstrated that improvements in weight could be maintained long-term and that improvements in HbA1c could be maintained in those patients who continued to perform SMBG daily.
Generally, glucometabolic control becomes impaired during the years after diabetes diagnosis. The United Kingdom Prospective Diabetes Study demonstrated for a period of 2 years after diagnosis that patients with T2DM with conventional therapy show an increase in HbA1c of about 0.1% and in weight of about 2.0 kg. 14 In parallel, the achieved improvement of −0.7% in HbA1c in the Look AHEAD study 1 became reduced to −0.36% after a follow-up period of 4 years. 15 With the 12-week ROSSO-in-praxi study we could demonstrate a beneficial effect of SMBG on HbA1c and weight with long-term effects on both parameters. During the 12 weeks of lifestyle intervention participants learned how to use SMBG to control their dietary pattern and physical activity and how to change their lifestyle in order to reach good blood glucose values. Indeed, the study population demonstrated an HbA1c reduction of 0.3% in total, whereas those who were able to lose 5.1–10.0 kg of weight had an improvement of 0.5%, and those who lost more than 10 kg reached a mean decrease in HbA1c of 0.9%. 10 Although there was an increase in HbA1c 2 years after end of lifestyle intervention, our results clearly demonstrate (1) that such an increase fits to the normal development (as shown by the United Kingdom Prospective Diabetes Study and Look AHEAD), (2) that the maintenance of HbA1c reduction strongly depends on the maintenance of weight loss (and this is strongly in line with the findings after 12 weeks of lifestyle intervention 10 ), and (3) and it is of particular interest that there was a trend that those participants who continued to perform SMBG daily could maintain the achieved HbA1c and weight reduction over time. These results suggest that those persons who were able to identify the relationship between their nutrition/physical activity and their blood glucose levels and to use this knowledge to improve their lifestyle might benefit from daily SMBG in the long run. Moreover, the high rate of 88% of those who actually continued to perform SMBG confirms that SMBG and SMBG-structured lifestyle changes could easily be integrated into general diabetes care. On the other hand, it clearly demonstrates that the continuous usage of SMBG can help patients to maintain favorable lifestyle behaviors.
The physical health–related quality of life of 65.2 measured by the validated SF36 questionnaire points out that our study population feels physically impaired because the value is lower compared with those from a German control population of hypertensive patients (physical health–related quality of life=66.9) used for validation of the SF36 instrument. 16 Although by the end of the 12-week lifestyle intervention the physical health score had increased up to 69.0, this measurement remains lower than the score from a healthy control population (physical health–related quality of life=88.5), 16 and after 2 years it had decreased again to 66.7, which seems to be in the range of the hypertensive control population. In contrast, the baseline value for mental health–related quality of life of 67.9 in our study population is higher than those of the hypertensive control population (mental health–related quality of life=64.2) and increased up to 71.8, approaching the average score of 73.2 of the healthy control population. 16 Although during the 2 years of follow-up improvements in mental health–related quality of life became slightly reduced over time to a value of 69.9, it remained (1) significantly higher compared with baseline and (2) between the measurements of the hypertensive and the healthy control populations. Concomitantly, the percentage of depressed participants remained stable during follow-up. This might be explained by the fact that mental health–related quality of life becomes not only impaired by depression (which was low in this population) but is also influenced by diabetes-specific impairments. Therefore, it is possible that mental health–related quality of life became improved, although depression measurements did not change significantly, if, at the same time, diabetes-specific impairments were diminished and patient empowerment became increased.
Our study has several limitations that need to be considered. First, although non-responders were additionally contacted by telephone, a response rate of only 70% was reached. The patients who managed to maintain their metabolic improvements may have been more motivated to respond. This might have biased the results, and the effects might have been weaker (or even stronger) in the complete study population. Nevertheless, the fact that the baseline characteristics as well as the outcomes of the study population and of those who completed the follow-up did not differ except for the duration of diabetes argues against such a responder bias. Second, because of the study design, the follow-up is lacking a control group. This problem we thoroughly discussed before. 10 However, the follow-up data have the benefit that participants could be stratified according to their SMBG performance. Therefore, by using the group that discontinued SMBG as an internal control, we could demonstrate a superior outcome in HbA1c of those who continued SMBG. Nevertheless, the analysis of long-term effects of SMBG on metabolic control in a randomized controlled trial is warranted.
In summary, the SMBG-structured lifestyle intervention program ROSSO-in-praxi has shown to be effective in motivating T2DM patients for lifestyle changes and to improve glucometabolic and general health. Integration of this short-term, motivational and low-cost intervention 10 into basic therapy of insulin-naive T2DM patients can improve glucometabolic health and contribute to beneficial long-term effects on weight development as well as mental health–related quality of life and, if SMBG is performed at least daily, also on glycemic control. Therefore, SMBG might be a motivational tool for lifestyle change. However, any benefit will depend on the ability of patients to understand the results and to respond appropriately. This has been clearly demonstrated by the facts that (1) those patients who managed to lose weight during the study period had a much higher improvement in HbA1c and (2) HbA1c reduction could be mainly maintained by those patients who continued daily SMBG. Thus, SMBG could strengthen patient empowerment in order to change lifestyle, but it might not be useful for patients who lack the necessary skills and motivation for proper documentation and utilization of SMBG results. Therefore, a SMBG-structured lifestyle intervention program should be offered to those T2DM patients who are trying to adapt to a healthier lifestyle.
Footnotes
Acknowledgments
The study was funded by Die EigenInitiative of the Motivation zur Lebensstil-Änderung–Chance bei Diabetes in der Deutschen Diabetes Stiftung Foundation and a grant by Roche Diagnostics Deutschland GmbH.
Author Disclosure Statement
K.K. and S.M. received fees for lectures and consultancy from Roche Diagnostics Deutschland GmbH. The sponsors have not had influence on the analysis and interpretation of the data as well as in the writing of the report. J.K. has nothing to disclose.