
Abstract
Background:
Endothelial function is known to be impaired in response to heat in people with diabetes, but little has been done to see how air humidity alters the skin blood flow response to heat.
Methods:
Seventeen male and female subjects were divided in two groups, one with type 2 diabetes and the other the control subjects without diabetes, age-matched to the diabetes group. All subjects participated in a series of experiments to determine the effect of the warming of the skin by air on skin temperature and skin blood flow. On different days, skin temperature was warmed with air that was 38°C, 40°C, or 42°C for 20 min. Also, on different days, at each temperature, the air humidity was adjusted to 0%, 25%, 50%, 75%, or 100% humidity. Skin blood flow and temperature were measured throughout the exposure period. This allowed the interactions between air humidity and temperature to be assessed.
Results:
For the control subjects, the moisture in the air had no different effect on skin blood flow at air temperatures of 38°C and 40°C (analysis of variance, P>0.05), although skin blood flow progressively increased at each air temperature that was applied. But for the warmest air temperature, 42°C, although the four lower humidities had the same effect on skin blood flow, air at 100% humidity caused the largest increase in skin blood flow. In contrast, in the subjects with diabetes, blood flow was always significantly less at any air temperature applied to the skin than was observed in the control subjects (P<0.05), and skin blood flow was significantly higher for the two higher humidities for the two higher air temperatures. Skin temperature paralleled these findings.
Conclusion:
These data show that individuals with diabetes do not tolerate moist, warm air above 50% humidity as well as controls without diabetes.
Introduction
One of the principal stressors that affect the skin is temperature. 19 –21 An increase in skin temperature due to a local heat source (local heat) causes a biphasic response vascular response. In the first phase of the response, transient receptor potential vanilloid (TRPV) 1 voltage-gated calcium channels in sensory tactile nerve endings cause the release of substance P and calcitonin gene-related peptide. 19 –21 These substances diffuse into vascular smooth muscle, causing the muscle to relax and blood flow to increase. This response is short lived because of accommodation of tactile sensors to heat. 19 The sustained response, which begins a minute or so after heat is applied, is mediated by TRPV4 voltage-gated calcium channels in the vascular endothelial cells themselves. 22 –25 These channels then cause the influx of the calcium from the extracellular space to the intracellular space. Because there is a calcium binding domain on endothelial nitric oxide synthetase, the increase in tissue temperature directly causes an increase in tissue blood flow mediated by nitric oxide. 7,26,27 In younger individuals, a prostaglandin compound, prostacyclin (prostaglandin I2), also aids in the vasodilatation to heat. This mediator is not generally important in older individuals or people with diabetes. 22
It is commonly known that people with diabetes have an impaired circulatory response to heat. 9,28 –33 In addition, there is an impaired circulatory response to contrast baths and global heat as well. 34 All of these factors make people with diabetes much more susceptible to heat stress and thermally related burns. 9 Another limitation in the response to heat is due to thinning of the dermal layer of the skin and increase in subcutaneous fat in people with diabetes. 35 –37 Thinning of the dermal layer is associated with a reduction in capillary density (capillary rarefication) and an increase in subcutaneous fat prevents conductive heat loss through the skin. 38
Most studies on local heat exposure have studied heat using a thermode, a device that lies on the skin and delivers a set temperature while skin physiology is studied. This corresponds to dry hot packs applied to the skin. In people with diabetes, the circulatory response to dry heat is impaired compared with age-matched controls. 39,40 An alternative is a moist heat source. Although age-matched controls still have a greater skin blood flow response to moist heat than people with diabetes, the blood flow response is still much better than for dry heat. 28,41 –43 This is probably because of activity of TRPV4 osmotic receptors on vascular endothelial cells; the normal dry skin associated with diabetes and aging is moisturized with the moist heat source, and the circulatory response at the same skin temperature is enhanced. 44,45 Thus, compared with dry heat, moist heat has about 30% higher blood flow response than dry heat for warming the skin, making it a much safer modality. 42,44,45 However, all studies of the blood flow response of the skin have either used dry heat or heat with 100% humidity. In the normal climatic exposure seen by people with diabetes or controls, humidity varies from 0% to 100%, and thermal contact is largely through air movement, not water. With exposure to air, sweat is an important variable in that sweat can help cool the skin. 46,47 Sweat glands are lost first from the feet and legs and later in other areas such as the arm. 48 Thus sweat may also be an important variable in any differences in the response to warm air in controls compared with people with diabetes.
The purpose of the present investigation was to characterize, in people with diabetes, the relationship between the moisture of the air and the skin blood flow response and temperature by looking at a variety of skin temperatures and humidity applied to the skin. This is a more realistic evaluation of how the skin in people with diabetes responds to the environment.
Subjects and Methods
Seventeen subjects participated in these experiments. The subjects were divided into two groups: one group was the diabetes group, and the other group was age-matched controls. Subjects were recruited by flyer from Loma Linda, CA. Subjects had no diagnosed cardiovascular disease, were not taking any medications that would affect the cardiovascular system, and had no known peripheral circulatory diseases. Subjects were not taking α- or β-agonists or antagonists. For the subjects with diabetes, the average hemoglobin A1c was 7.8±2.5%. All subjects were nonsmokers. For all subjects blood pressure and heart rate was measured at rest, and subjects were excluded if blood pressure was >140/90 mm Hg or <100/60 mm Hg. A screening history was taken. Sensory testing was done on the arms and legs, and subjects were excluded if they failed a 10-g sensory test on more than two points on their feet. Lack of feeling of pressure to a 10-g monofilament is a standard clinical measure for the diagnosis of diabetic polyneuropathy. The general characteristics of the subjects are given in Table 1. There was no statistical difference between the subjects. All protocols and procedures were approved by the Institutional Review Board of Loma Linda University, and all subjects signed a statement of informed consent.
BMI, body mass index.
Skin temperature
Skin temperature was measured with a thermistor (SKT RX 202A) manufactured by BioPac Systems (BioPac Inc., Goleta, CA). The thermistor output was sensed by an SKT 100 thermistor amplifier (BioPac Inc.). The output, which was a voltage between 0 and 10 V, was then sampled with an analog to digital converter at a frequency of 1,000 samples per second with a resolution of 24 bits with a BioPac MP150 analog to digital converter. The converted data were then stored on a desktop computer using Acknowledge version 9.1 software for analysis. Data analysis was done over a 5-s period for mean temperature. The temperature was calibrated at the beginning of each day by placing the thermistors used in the study in a controlled temperature water bath that was calibrated against a standard thermometer.
Measurement of skin blood flow
Skin blood flow was measured with a Moor laser Doppler imager (Moor Instruments, Axminster, Devon, UK). The imager used a red laser beam (632.8 nm) at a power of 2.5 mW to measure skin blood flow using the Doppler effect. The laser, in this case, was used in single-point mode. After the laser was warmed for 15–30 min prior to use, the laser was focused through the capsule and on the skin, and, by comparing the reflected with the source light, the change of the frequency of the light and absorption of the light was used to calculate the red blood cell velocity and the red blood cell content in that area of the skin. The Moor laser Doppler imager measured blood flow through most of the dermal layer of the skin but did not penetrate the entire dermal layer. Blood flow was then calculated in a unit called flux based on the red blood cell concentration and red blood cell velocity with a stated accuracy of ±10%. 49 The tissue thickness sampled was typically 1 mm in depth.
Measurement of air flow
Air flow was measured with a Fox inline flow meter (Fox Thermal Instruments, Marina, CA). The sensor had a ½-inch inlet and measured air flow to 10,000 mL/s. By using a thermal dilution principle, the flow meter provided gas temperature and flow of air linearly.
Measurement of skin moisture
Skin moisture was measured with a Corneometer 810 capacitance skin moisture meter (Courage Khazaka Electronics, Koln, Germany). The moisture was in units of between 1 and 100. The Corneometer has been validated in numerous studies as stated below. It uses tissue capacitance assessed by applying electromagnetic waves at a frequency of 100,000 cycles/s to image the skin surface. 50,51 It has been used extensively to evaluate the effect of different treatments on skin condition. 52 The Corneometer uses a a frequency of 100,000 cycle/s. 53,54
Moisture is measured in the superficial layers of the stratum corneum as deep as 10–20 μm to ensure that the measurement is not influenced by capillary blood vessels.
Control of air temperature and humidity
To accomplish these goals, the following design was developed. First, compressed air was supplied by a central air compressor with a 1,000-L reservoir and adjusted to a pressure of 10 bars. A dryer on the tank eliminated much of the trapped moisture, and a fan kept the tank at near room temperature. In such a system, air pressure varies when the compressor motor cycles on and off as the pressure sensor senses a pressure drop and engages the pump. The variation in pressure was ±0.2 bar. To stabilize this pressure variation, the air supply was down-regulated into a 40-L pressure reservoir at a pressure of 2 bars. The low pressure reservoir had a moisture collection chamber to remove excessive moisture that might be in the lines from the main air supply. The tank was made of metal and cooled with a fan. The output of this pressure reservoir then passed through 15.3 m of copper tubing, which was 63.5 mm in diameter. The tubing was submersed in a well-stirred and temperature-regulated water bath with a volume of 0.1 m3 so that the air was brought to the desired temperature for the study. The temperature of the water in the bath was regulated by a Fisher model 2100 Isotemp heater digital temperature regulator (Fisher Scientific, Waltham, MA) with 1,000 W of heat capacity and a water stirring motor. This kept the water temperature variation to less than ±1.0°C in the bath. The air pressure at this point was 0.5 bar. The warmed air was then separated through two air flow valves (MR3000 series, Key Instruments, Trevose, PA) capable of regulating air flow up to 1,500 mL/s. The two separate air paths then routed air through either a pressurized container of Drierite (Hammond Drierite, Xenia, OH) or through a 2-L glass bottle filled with water and also lying in the water bath. The air pressure after the water bottle or Drierite was reduced to 0.26 bar.
A bubbler made of perforated copper pipe in the bottom of the water bottle saturated the air with water as it moved from the bottom to the top of the bottle. Because the bottle was placed in the water bath, the moist air was at the bath temperature. A fiberglass layer near the outlet valve in the bottle kept water from entering the exhaust line. The two sources of air—one dry and one at 100% humidity—then were mixed and traveled through a 15.24-m piece of 63.5-mm-diameter copper tubing in the water bath (length×width×depth, 92.5×38.9×39.8 cm). This allowed the mixed air to remain at the desired temperature. Here the air pressure was now 0.02 bar. As it left the tubing, the air flowed through a humidity and temperature sensor (heavy-duty moisture meter number 407777, Extech, Waltham). The sensor was a combined calcium chloride moisture sensor with a thermistor for temperature of the mixed gas. The sensor chamber itself was sealed. The air pressure at the output of the sensor was 0.01 bar. The pressure reduction through the lines created a problem as the gas emerged from the submerged coils in the water bath. The drop in pressure was enough to cause adiabatic cooling, which, for moist air, caused the air to condense as before it arrived at the skin. To prevent this, the air flow lines to and from the capsule and the capsule itself were temperature controlled. The air lines were all covered with 63.5-mm-diameter plastic tubing, which also carried water that circulated from a pump in the water bath such that the temperatures of the sensor and air lines were maintained near bath temperature. The water flow lines were arranged with the line closest to the body connected to the bath, and the return was placed near the bath. This was used to make the heat delivery system a counter current multiplier. The capsule that was in contact with the skin was rectangular with dimensions of 28.11 mm height, 47.95 mm width, 49 mm length, and 10.27 mm thickness. A water jacket was integrated into the capsule. Water from a pump perfused the capsule with water to maintain the capsule temperature at bath temperature. Thus by adjusting the two flow meters on the moist and dry air sources, any possible combinations of temperatures and humidities could be set into the capsule in contact with skin. A hole that was 8.64 mm in diameter in the center of the capsule allowed a laser to penetrate the capsule and provide the skin blood flow during the heating process.
Procedures
Subjects entered a thermally neutral room (22°C) and rested comfortably for 20 min. Baseline blood flow was recorded for 1 min. After this period of time, the thermode was placed on the arm above the center of the brachioradialis muscle for 20 min. On different days, the air temperature was 38°C, 40°C, or 42°C for 20 min. At each temperature, the moisture (humidity of the air) was adjusted to 0%, 25%, 50%, 75%, or 100% humidity. This allowed the interactions among skin moisture, temperature, and aging to be assessed. Skin moisture was measured before and after the 20-min period, and blood flow was measured continuously.
Analysis of data
Analysis of data involved the calculation of means and SDs and related and unrelated t tests. Data were analyzed on Excel (Excel 2010) (Microsoft, Redmond, WA). The level of significance was P≤0.05.
Results
Skin blood flow
As illustrated in Figure 1, there was a difference in the resting blood flow (at 38°C) between the control subjects and the subjects with diabetes. The average resting blood flow under all conditions was 88.6±21.3 flux for the subjects with diabetes and 113.6±37.4 flux for the age-matched control subjects. This difference was significant (t test, P<0.01). After the warm air flow started to the skin, blood flow increased both with time and with their temperature as shown in Figure 1. For the control subjects, there was no significant difference at any time during which heat was applied throughout the entire exposure period or for 1 min after exposure in the blood flow for dry air or air at 25%, 50%, 75%, or 100% humidity (Fig. 1A) (analysis of variance, P>0.05 comparing all data at all times). The increase over time was significant (analysis of variance, P<0.01, pooled data comparing all times on the curve), whereas comparing the blood flow at each minute for dry heat and heat at 25%, 50%, 75%, or 100% humidity, there was no statistical difference at any point in time between any blood flow recorded at any humidity of air (analysis of variance, P>0.05).

Relationship between skin blood flow and duration of the heat exposure (x-axis) throughout exposure to air at 38°C: (
For the subjects with diabetes (Fig. 1B), there was also no statistical difference at any one point in time for the blood flow response at any of the five air humidities (P<0.05), but the average blood flow response was diminished compared with the control subjects (P<0.05). Statistical analysis showed that, averaging the blood flows for all five humidities, the average blood flow at any point in time was significantly less in the diabetes subjects compared with the control subjects (P<0.05). As shown in Figure 2, when air was applied to the skin of the control subjects at these same humidities but with an air temperature of 40°C, the same relationship was seen: that is, a linear increase in blood flow up to min 17, after which there was a slight decline throughout the end of the time (Fig. 2A). There was no statistical difference in the blood flow seen for air at any of the different humidities (P<0.05). The skin blood flow when subjects were exposed to the 100% humidity air was significantly higher than the other flows during exposure to the other four humidities for the subjects with diabetes. From min 4 to min 19, for the subjects with diabetes, air at 75% humidity also caused a larger increase in blood flow than dry air and air at 25%, and 50% humidity; however, this did not reach significance (analysis of variance, P=0.1). For an air temperature was 42°C, the blood flow responses for the control and diabetes groups are illustrated in Figure 3. Unlike the two cooler temperatures, when air was at a temperature of 42°C, there was a clearly greater increase in blood flow with air at 100% humidity than was the case with dry air or air of 25%, 50%, or 75% humidity as shown in Figure 3. From min 2 to min 20 of exposure, for the control subjects, this increase in blood flow above the other three air temperatures was significant (analysis of variance, P<0.05). The highest blood flow for the age-matched controls with 100% humidity was 628±103.2 flux achieved at 13 min. With moist air, this peak blood flow was significantly higher than that seen for the subjects with diabetes in Figure 3B (P<0.01). In addition, in the subjects with diabetes, although the blood flow was less for air at 75% humidity than it was for 100% humidity, blood flow in the skin in response to air at 75% humidity was still significantly higher than it was seen for dry air or air at 25% or 50% humidity for almost all study intervals as shown in Figure 3B (analysis of variance, P<0.05).
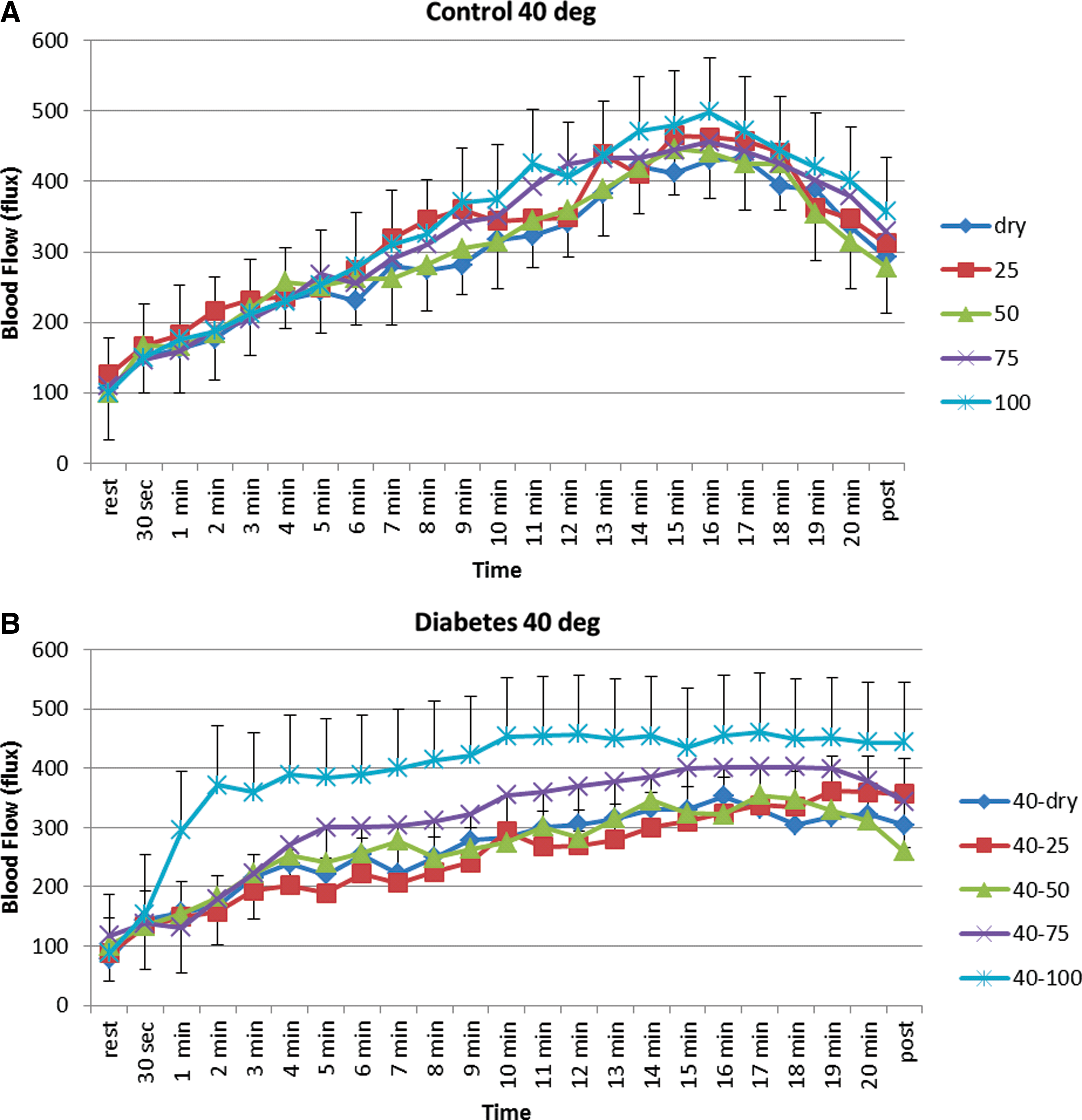
Relationship between skin blood flow and duration of the heat exposure (x-axis) throughout exposure to air at 40°C: (
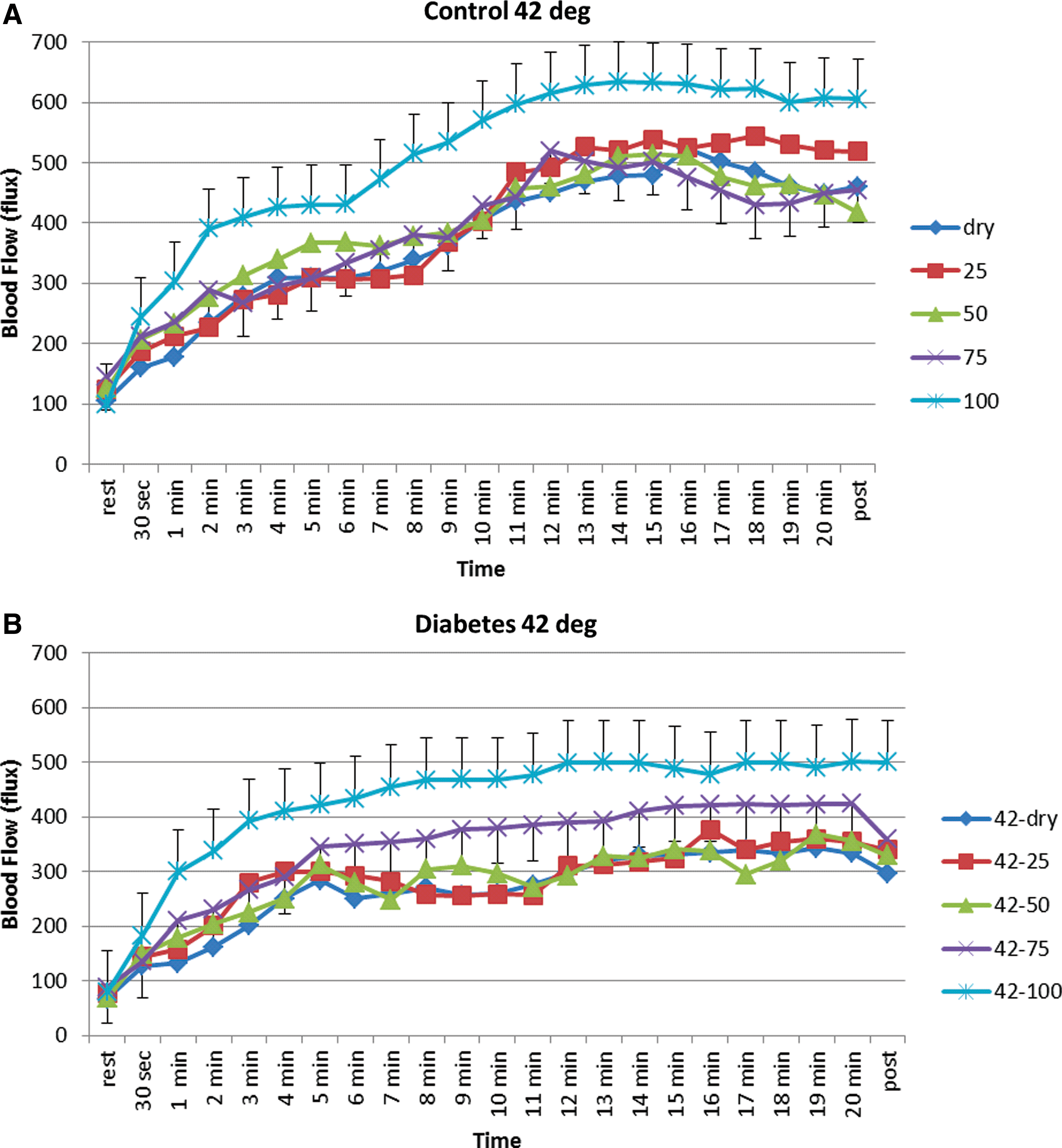
Relationship between skin blood flow and duration of the heat exposure (x-axis) throughout exposure to air at 42°C: (
Skin moisture
The skin moisture before and after heat exposure is shown in Table 2. Skin was initially moister in the control group, and the rise in skin moisture at each exposure was greater in the controls except for the dry air, where the skin was drier after exposure in both groups of subjects.
P<0.05, ** P<0.01.
Skin temperature
For exposure to air at 38°C, Figure 4A shows that skin temperature in the control subjects increased to just over 36°C after 20 min of exposure for the three driest air temperatures, whereas for the moistest air (100% humidity), skin temperature was elevated by almost 2°C above this. The difference in skin temperature in the control subjects at 100% humidity versus the other four humidities was significant (analysis of variance, P<0.01). For the subjects with diabetes, at 38°C air temperature, the same phenomenon was seen except that here the skin temperature was higher with exposure to both 100% humidity air and 75% humidity air compared with the other three temperatures (analysis of variance, P<0.05).

Skin temperature (°C) recorded from the skin on the forearm at rest and throughout the 20-min exposure, where the skin was exposed to air at 38°C that was either dry or at 25%, 50%, 75%, or 100% humidity: (
This same response was seen for 40°C air and 42°C air. For the 40°C air (for the control subjects, Fig. 5A) with 100% moist air, skin temperature rose to 40°C, whereas with dry air it was maintained at 38°C. Thus, the warmer the air, the higher the skin temperatures, as might be expected. However, for the diabetes subjects (Fig. 5B) skin temperature also rose to 40°C with the moist air, with the second highest increase in skin temperature occurring with the air that was 75% humidity. This is also seen in Figure 6 for air at 42°C. For the subjects with diabetes, the data stratified with the three lowest humidities: that is, dry, 25%, and 50% humidity values were clearly distinct from those with 75% and 100% humidity air.

Skin temperature (°C) recorded from the skin on the forearm at rest and throughout the 20-min exposure, where the skin was exposed to air at 40°C that was either dry or at 25%, 50%, 75%, or 100% humidity: (

Skin temperature (°C) recorded from the skin on the forearm at rest and throughout the 20-min exposure, where the skin was exposed to air at 42°C that was either dry or at 25%, 50%, 75%, or 100% humidity: (
Discussion
It is well established that diabetes is associated with impaired endothelial function. 11,22 Impaired endothelial function affects most organs systems in the body. 7 One major area that is affected by impaired endothelial function is skin circulation. 10,30,34 The response to pressure, 29 the response to local heat, 20,25,42 and even the response to global heating is affected by diabetes. 9,55,56 Furthermore, sweating is impaired in diabetes because of damage to the nitric oxide pathway that activates the sweat glands in the body. 13,48,57 Thus, all methods of maintaining thermoregulatory stress in the body—that is radiation, conduction, convection, and evaporation—are reduced in diabetes, making this population more susceptible to thermal damage and overheating of the whole body. 13,48,57
Studies of the affect of local heat on the skin have included studies using both dry heat and heat with 100% humidity. 31,40,43,57 Heat with 100% humidity is usually achieved by heating the skin or body in a water bath such as in a contrast bath 34,58 or using hydrocollator heat packs 40 or by devices that produce 100% humidity in the air. 40 However, most of the time, a person with diabetes is exposed not to water baths but during daily activities to air—air with varying humidity. The moisture in the air varies from 0% to 100% humidity depending on atmospheric weather conditions. No study has examined the response of the skin in people with diabetes to air with various humidities to see how the skin responds. This is particularly important in light of the fact that osmoreceptors in vascular endothelial cells alter blood flow based on skin moisture content. 9,37,39,40 Because people with diabetes inherently have damage to the dermal layer of the skin and exhibit a reduced response to both moist and dry heat, 7,14,36 it was interesting to examine the effect of air moisture on the dynamics of the blood flow response of the skin.
A principal finding in the present investigation is that with air at high humidity, the skin warms faster, and the blood flow response is greater than with air at lower humidities. For air temperatures of 38°C, for control subjects, it made no difference what the humidity of the air was: the skin would warm a little bit more, but the blood flow response was essentially the same at all humidities. In contrast, with air at 40°C, although the control subjects had the same blood flow response irrespective of humidity, the subjects with diabetes began to show a dichotomy in response, with air at 75% and 100% humidity causing a progressively greater increase in skin moisture and skin blood flow in response to heat. At 42°C this was also seen in the subjects with diabetes, but in addition control subjects also showed a greater blood flow response in skin moisturizing with the 100% humidity air.
For the age-matched control subjects, what this means is that the humidity of the air is really unimportant until humidity reaches 100% in terms of the ability of the skin to maintain temperature in the face of a thermal load from air. The higher blood flows and the higher skin temperatures seen with air at 42°C are probably related to the fact that sweating becomes ineffective. At lower air humidities, the skin is able to sweat and thus lose temperature (dissipate heat). Evaporation of sweat is a major mechanism for keeping the skin cool. However, for control subjects, at 42°C with 100% humidity air, the skin was not capable of losing heat by sweat because sweat will not evaporate in air that has a 100% humidity. Thus, in the control subjects, under the harshest conditions—that is, 42°C—skin temperature and blood flow rose much higher, whereas up to 100% humidity the skin was not able to properly control the temperature of the skin by sweat so blood flow would increase disproportionately. In the subjects with diabetes, there was a tendency at 38°C air for the skin to begin overloading at 100% humidity; however, at 40°C and 42°C (seen clearly from Figs. 2 and 3), in the subjects with diabetes either 100% humidity air or 75% humidity air caused an increase in skin temperature and skin blood flow, and the skin was not able to accommodate these higher temperatures and humidities. Part of this may be due to sweat gland damage as is found in people with diabetes and circulatory damage as well. Both probably contribute to this lack of ability of the skin to tolerate warm air even at 75% humidity.
For the controls, additional evidence of a difference compared with the patients with diabetes is the fact that for the controls, skin blood flow rose with heat exposure and then, toward the end of exposure, fell slightly. This is commonly seen with prolonged heat exposure in that the endothelial nitric oxide synthetase pathway accommodates to prolonged heat. 7 The fact that it did not happen in the people with diabetes may be related to the high levels of free radicals commonly seen in this population. 7,9 If high free radicals reduced the productions of nitric oxide, it may also impair accommodation and result in a sustained blood flow response. Further investigation is needed. The faster rate of rise of blood flow in the diabetes patients in Figures 2 and 3 with air at 100% humidity compared with the controls may be related to a faster rate of rise of skin temperature in the diabetes subjects triggering a greater blood flow response, whereas the total maximum response to heat was lower than that seen in the controls.
In practical terms, whereas older control subjects can properly maintain thermoregulation in hot and humid weather (e.g., in the Midwest or South in the middle of the summer), a lot of the reserves in terms of increase in blood flow and the ability to sweat in response to heat are so diminished in people with diabetes that they are very much more at risk in a humid hot environment.
Because sweat glands and neuropathies are lost first in the feet and then in other areas of the body, 48 future studies may include other areas to see if the same phenomena occur. Future studies may also examine different rates of air flow because the rate of flow was controlled here at just one velocity. Changing air flow may alter the dynamics of the response of the skin.
Footnotes
Author Disclosure Statement
No competing financial interests exist.