
Abstract
Background:
Liraglutide was examined for its effects on 24-h glucose fluctuations in Japanese type 2 diabetes patients as well as for its differential effects depending on glucose tolerance status after favorable glycemic control was obtained in these patients.
Patients and Methods:
In this prospective open-label pilot study, a total of 20 type 2 diabetes patients hospitalized for glycemic control were given liraglutide 0.3 mg, followed by liraglutide 0.6 mg and 0.9 mg, with each given at 1-week intervals. The patients were continuously monitored for their 24-h glucose levels before treatment and during the course of treatment with liraglutide 0.3 mg, 0.6 mg, and 0.9 mg, respectively, using continuous glucose monitoring (CGM). At the start of treatment with liraglutide, 12 patients were on diet therapy alone, of which six were drug-naive, and eight were being treated with glimepiride.
Results:
Liraglutide not only significantly reduced 24-h mean glucose levels but also significantly improved all the indices for glycemic variation evaluated, which included SDs of 24-h glucose levels, mean amplitude of glycemic excursions (MAGE), and total area under the glucose fluctuation curve (AUC) for 24 h. The study showed a significant negative correlation for mean glucose levels, SD, and AUC immediately before treatment versus their changes with liraglutide. A 75-g oral glucose tolerance test (OGTT) was given in 11 patients treated with liraglutide monotherapy once favorable glycemic control was achieved. The OGTT revealed that of these, six were found to have normal glucose tolerance, four had impaired glucose tolerance, and one had diabetes, and that of the six drug-naive patients, five patients were found to have normal glucose tolerance, and one had impaired glucose tolerance.
Conclusions:
Study results showed that liraglutide is expected not only to reduce mean glucose levels but also to improve 24-h glucose fluctuations, including postprandial glucose excursions, with its effects being particularly conspicuous in patients with early-stage type 2 diabetes.
Background
Against this background, there are mounting expectations for incretin-based drugs, which are known to stimulate glucose-dependent insulin secretion, unlike conventional antidiabetes agents. Of these, the human glucagon-like peptide-1 (GLP-1) analog liraglutide is drawing particular attention as a novel agent of interest, which has been shown not only to stimulate insulin secretion in a glucose-dependent manner but also to reduce body weight in humans and increase numbers of pancreatic β cells in animal models. Indeed, liraglutide has been shown to be highly efficacious in clinical trials conducted in Japan. 1,2 However, liraglutide has primarily been evaluated for its hypoglycemic efficacy with hemoglobin A1c (HbA1c) measurements or meal tolerance test 3 but not in relation to 24-h glycemic variations.
In this study, liraglutide was monitored for its effects on 24-h glucose variability in type 2 diabetes patients as well as for its differential effects depending on glucose tolerance status after favorable glycemic control was obtained with liraglutide in these patients.
Patients and Methods
Patients
This was a prospective, open-label pilot study conducted with the approval of the Ethics Committee of Shinyamanote Hospital (Higashimurayama city, Tokyo, Japan). Prior to the start of the study, all participants in the study were fully informed about the study and gave informed consent in writing to participate in the study.
Of the type 2 diabetes patients hospitalized in Shinyamanote Hospital for glycemic control, those who met the following criteria were included in the study: (1) age, 20–75 years; and (2) HbA1c (Japanese Diabetes Society) value at admission, 6.5%–10.0%. Patients were excluded if they had type 1 diabetes (glutamic acid decarboxylase antibody–positive, urinary C-peptide ≤10 μg/day), had a history of severe infection in the past 3 months, or had received steroid therapy as part of antirheumatic therapy in the past 3 months.
Methods
After hospitalization, once glucose levels before breakfast were shown to be <200 mg/dL with glycemic variations remaining stable with diet therapy alone or SU medications, the patients were monitored by using continuous glucose monitoring (CGM) (CGMS® System Gold™, Medtronic Inc., Northridge, CA). Liraglutide was given to the patients, starting with the 0.3 mg dose followed by liraglutide 0.6 mg and 0.9 mg, with each dose given at 1-week intervals, and the patients were monitored for 24-h (8 a.m.–8 a.m.) glucose levels immediately before the start of treatment as well as during treatment with liraglutide 0.3 mg, 0.6 mg, and 0.9 mg, respectively, for three consecutive days (Fig. 1). Antidiabetes treatments at baseline (at the start of treatment with liraglutide) included diet therapy alone in 12 patients, of which six were drug-naive, and glimepride in eight patients. CGM data obtained immediately before the start of treatment with liraglutide and during treatment with liraglutide 0.3 mg/day, 0.6 mg/day, and 0.9 mg/day were used to calculate the 24-h mean glucose levels and their SD, the mean amplitude of glycemic excursions (MAGE), 4 the total area under the glucose fluctuation curve (AUC) (total area between the 24-h mean glucose levels and glucose curve), the proportion of time in hyperglycemia (>180 mg/dL), and the proportion of time in hypoglycemia (<70 mg/dL). Additionally, once stable and favorable glycemic control was obtained with liraglutide 0.9 mg, a 75-g oral glucose tolerance test (OGTT) was conducted in 11 patients who were receiving liraglutide monotherapy to evaluate the differential effect of liraglutide by glucose tolerance status.
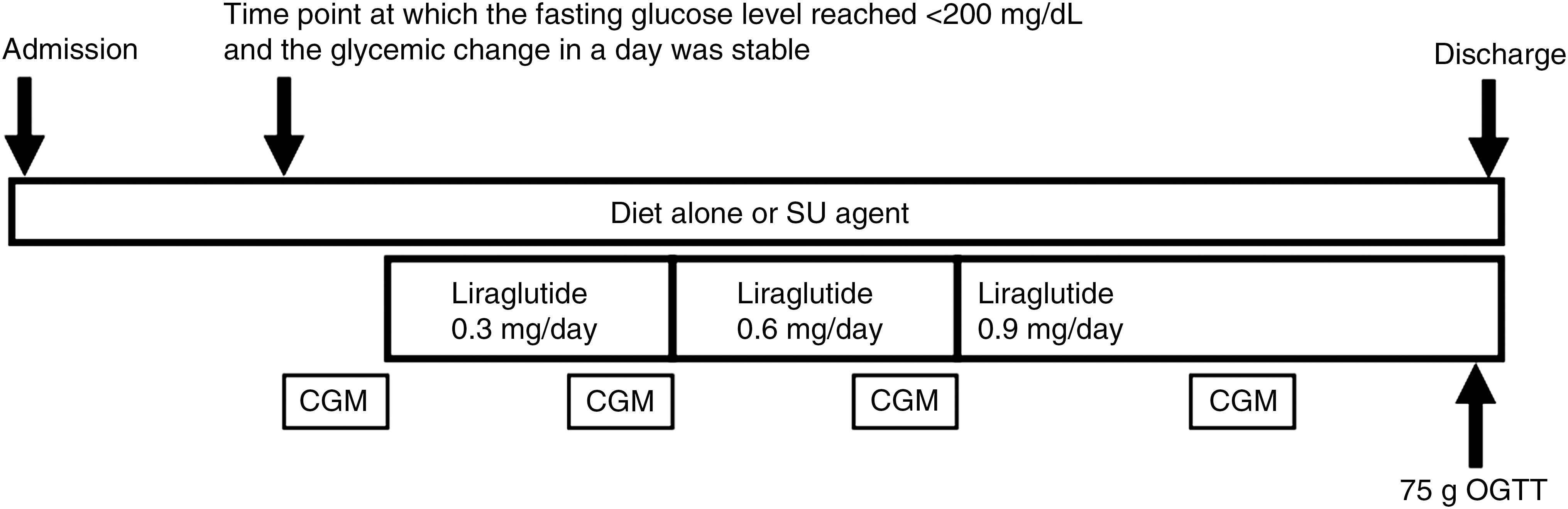
Outline of the study. Continuous glucose monitoring (CGM) was performed when the premeal glucose level became stable after dietary therapy alone or combination therapy with diet and sulfonylurea (SU). Liraglutide was given to the patients, starting with the 0.3 mg dose, followed by liraglutide 0.6 mg and 0.9 mg, with each dose given at 1-week intervals, and the patients were monitored for 24-h (8 a.m.–8 a.m.) glucose levels immediately before the start of treatment and during treatment with liraglutide 0.3 mg, 0.6 mg, and 0.9 mg, respectively, for three consecutive days. OGTT, oral glucose tolerance test.
Statistical analysis
All statistical analyses were performed by using SAS version 9.1 (SAS Institute, Cary, NC). Wilcoxon signed-rank test was used to compare the CGM data obtained immediately before the start of treatment with liraglutide and those obtained during the course of treatment with liraglutide 0.9 mg. Additionally, Pearson's simple correlation coefficients were calculated for correlation between the data obtained for indices of glycemic variation immediately before the start of treatment with liraglutide and the changes in these indices during treatment with liraglutide 0.9 mg.
Results
The study participants (n=20) had a mean age of 60.7±13.1 years, a mean body mass index of 28.2±4.8 kg/m2, a mean HbA1c (Japanese Diabetes Society) value at admission of 8.1±1.2%, a mean 1,5-anhydroglucitol value of 7.7±5.9 μg/mL, and a mean urinary C-peptide level of 79.9±41.3 μg/day. The antidiabetes treatments given were liraglutide monotherapy in 12 patients and combination therapy with liraglutide and SU in eight patients (Table 1).
Criteria of the Japanese Diabetes Society.
1,5-AG, 1,5-anhydroglucitol; HbA1c, hemoglobin A1c.
The 24-h mean glucose levels as assessed by CGM immediately before the start of treatment with liraglutide and during treatment with liraglutide 0.3 mg, 0.6 mg, and 0.9 mg are shown in Figure 2. The hyperglycemia noted after each meal at baseline was markedly improved by treatment with liraglutide, which led to significant improvements in 24-h mean glucose levels and their SD, MAGE, and total 24-h AUC compared with baseline (Table 2). Furthermore, treatment with liraglutide led to a significant decrease in the proportion of time in hyperglycemia (>180 mg/dL) without causing an increase in the proportion of time in hypoglycemia (<140 mg/dL) (Table 2).
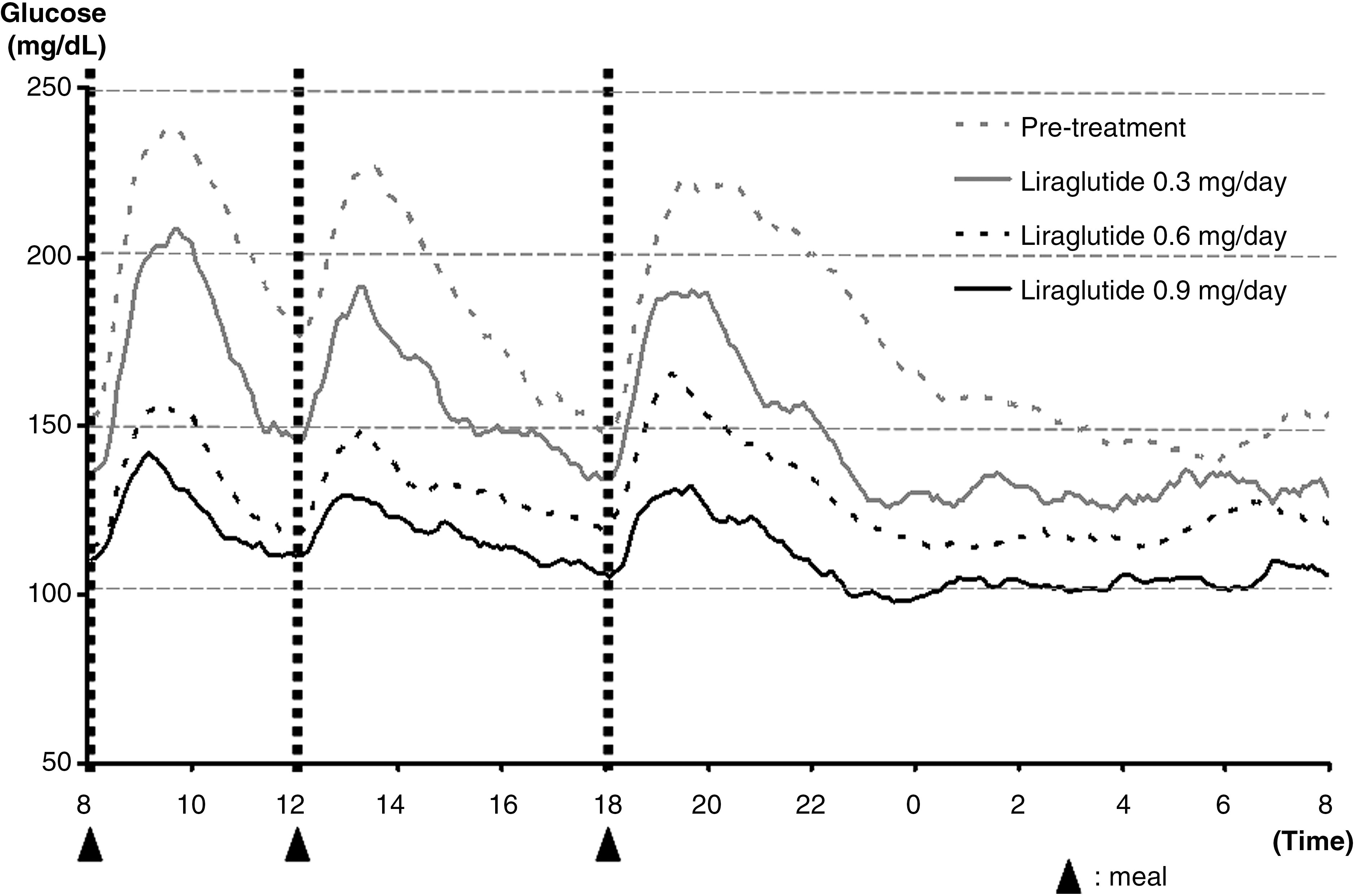
Changes in 24-h glucose levels before and after treatment with liraglutide in a total of 20 patients. Data are mean values.
P<0.001 versus pretreatment.
MAGE, mean amplitude of glycemic excursions.
In addition, the change in 24-h mean glucose levels in drug-naive patients from immediately before the start of treatment to during the course of treatment with liraglutide 0.3 mg/day, 0.6 mg/day, and finally 0.9 mg/day showed that treatment with liraglutide 0.9 mg/day led to the 24-h glucose fluctuations being nearly flattened (Fig. 3). As a consequence, a significant decrease was noted in 24-h mean glucose levels and their SD, MAGE, and total 24-h AUC compared with baseline, which also clearly showed that treatment with liraglutide 0.9 mg/day led to a marked narrowing of the range of glycemic variations in drug-naive patients (Table 3). When the patients were stratified by treatment (liraglutide monotherapy and combination therapy with SU), treatment with liraglutide consistently exhibited a similar trend to improve the range of glucose fluctuations in the patients.
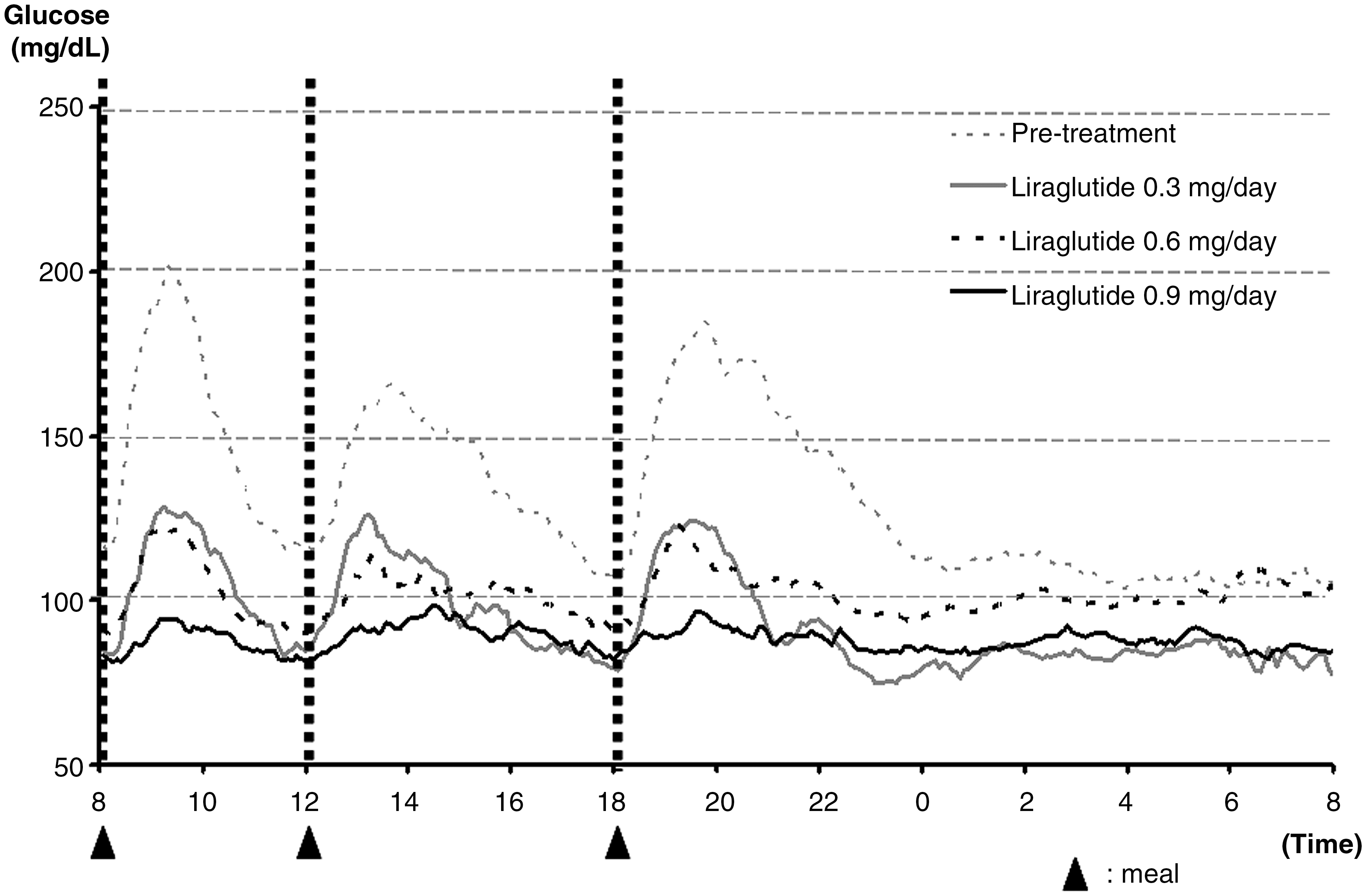
Changes in 24-h glucose levels before and after treatment with liraglutide in six drug-naive patients. Data are mean values.
P<0.05 versus pretreatment.
MAGE, mean amplitude of glycemic excursions.
There was a significant negative correlation between the baseline 24-h mean glucose levels and their changes with liraglutide (y=−0.5988x+41.096, R 2=0.7573, P=0.00004) (Fig. 4), between the baseline SDs of 24-h glucose levels and their changes with liraglutide (y=−0.4968x−2.1606, R 2=0.3192, P=0.00943), and between the baseline total AUC and their changes with liraglutide (y=−0.5563x−9.8325, R 2=0.3891, P=0.00328), respectively.
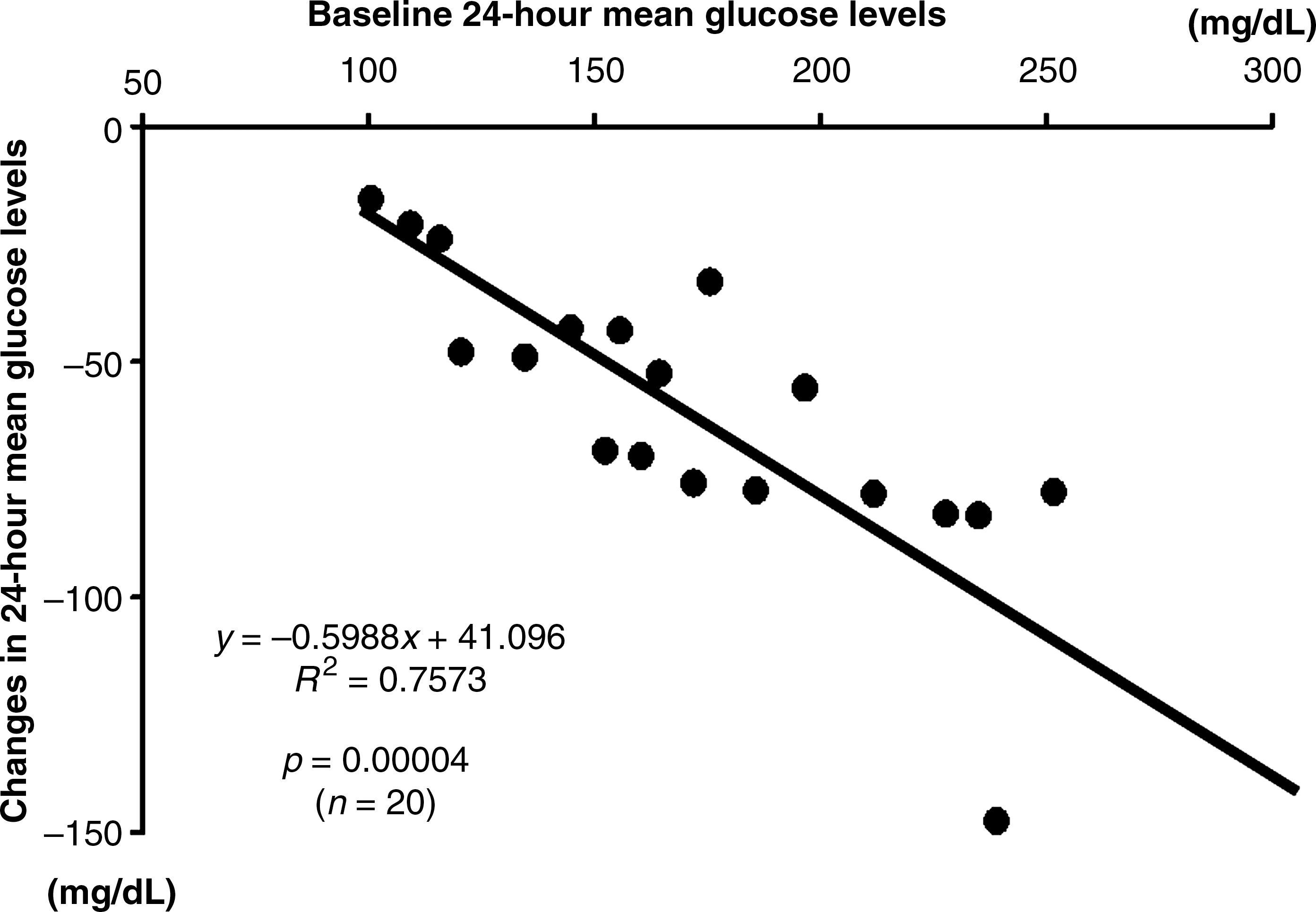
Correlation between 24-h mean glucose levels before treatment with liraglutide and the decrease in 24-h mean glucose levels after treatment.
Additionally, a 75-g OGTT conducted in 11 patients treated with liraglutide monotherapy who achieved favorable glycemic control revealed that of these, six, four, and one patients were found to have normal glucose tolerance, impaired glucose tolerance and diabetes, respectively, and that of the six drug-naive patients, five patients were found to have normal glucose tolerance, and one had impaired glucose tolerance.
Last but not least, no clinically relevant adverse reactions including gastrointestinal symptoms were noted during the course of treatment with liraglutide in this study.
Discussion
GLP-1 has been shown to exert glucose-dependent insulinotropic and glucagon-inhibitory effects, thus correcting hyperglycemia. 5 Therefore, glucose lowering with the human GLP-1 analog liraglutide does not involve, unlike SUs and glinides, direct insulinotropic effects through closure of KATP channels in the pancreas 6 but relies on glucose levels in those given liraglutide. 7 In this study, treatment with liraglutide led to a decrease in 24-h mean glucose levels, and this was thought to be attributable to correction of postprandial hyperglycemia by liraglutide. Additionally, although liraglutide led to a decrease in nighttime fasting glucose levels compared with baseline, this decrease was rather moderate in extent compared with that seen in postprandial glucose levels with liraglutide, thus providing evidence that supports the view that glucose lowering with GLP-1 is glucose-dependent.
CGM-based studies demonstrate that SUs decrease 24-h mean glucose levels as equivalent to HbA1c values and produce uniform, downward shifts in both postprandial and fasting glucose levels without narrowing the range of glucose fluctuations, 8 whereas, conversely, α-glucosidase inhibitors do not affect 24-h mean glucose levels very much, although they are potent in narrowing the range of glucose fluctuations. 9
In the present study, both liraglutide monotherapy and combination therapy with SU led to decreases in 24-h mean glucose levels associated with a narrow range of glucose fluctuation, which is consistent with the results of an earlier study 10 that demonstrated that sitagliptin, which produces glucose lowering by increasing physiological levels of GLP-1, led to a similar outcome. In other words, liraglutide is expected to improve postprandial hyperglycemia and glucose spikes that cannot be estimated by HbA1c monitoring and is thus more useful for correction of postprandial hyperglycemia, with the potential benefit of preventing macrovascular complications in type 2 diabetes. Furthermore, liraglutide led to conspicuous improvements in the range of glucose fluctuation in drug-naive patients in this study, with the glucose fluctuations flattening to a similar level to that seen in healthy individuals, 11 and the majority of these patients were found to have impaired glucose tolerance or normal glucose tolerance. These results suggest that the use of liraglutide may lead to remission of disease in patients with preserved pancreatic β-cell function, particularly when introduced as early as possible in these patients. Long-term studies are required to evaluate the effect of liraglutide on glycemic control, body weight, and pancreatic β-cell function, as well as its safety, in patients with early type 2 diabetes and to evaluate changes in glucose tolerance status and glycemic control after its discontinuation.
In summary, the decreases in 24-h mean glucose levels with liraglutide showed a significant correlation with the baseline 24-h mean glucose levels. In other words, the greater the baseline mean glucose levels, the greater the reductions in mean glucose levels with liraglutide. This finding is consistent with a long-term clinical study 12 showing that the greater the baseline HbA1c values, the greater the HbA1c lowering with liraglutide, likely supporting the observation that changes in the 24-h mean glucose levels in CGM-based drug therapeutic evaluation are linked to changes in HbA1c values in long-term clinical study. Furthermore, the fact that there was a significant correlation between the decreases in the SDs of 24-h glucose levels and the total AUC with liraglutide and their baseline values appears to imply that the greater the baseline range of glucose fluctuations, the greater the reduction in the range of glucose fluctuations, suggesting that liraglutide offers potent efficacy in maintaining glucose homeostasis.
Conclusions
Results of the present study demonstrate that in addition to producing reductions in 24-h mean glucose levels, the human GLP-1 analog liraglutide not only potently improves postprandial hyperglycemia but also improves fasting hyperglycemia without causing hypoglycemic episodes. Thus, liraglutide is thought to be a unique agent capable of correcting the 24-h glucose swing and maintaining glucose homeostasis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.