
Abstract
Iatrogenic hypoglycemia is one of the chief barriers to optimal glycemic control in people with type 1 diabetes (T1D). As a common contributor to morbidity and mortality in T1D, severe hypoglycemia (SH) is also a major fear for people with T1D and their families. Consequently, fear of hypoglycemia and hypoglycemia-avoidant behaviors are predominant limiting factors in achieving euglycemia in people with T1D. Nocturnal SH and hypoglycemia unawareness are prevalent obstacles in the detection of hypoglycemia which further impair the prevention and treatment of SH. Various strategies and technologies have already been developed to help detect and prevent hypoglycemia, including improved patient education, frequent self-monitoring of blood glucose levels, the use of rapid-acting and basal insulin analogs, continuous subcutaneous insulin infusion therapy, exercise-related insulin modifications, and continuous glucose monitors. The efficacy of these methods is well established, but further advances are still needed. The purpose of this review is to describe these currently available methods and to emphasize recent progress related to the prevention of hypoglycemia in T1D.
Introduction
Definition
The American Diabetes Association (ADA) has defined hypoglycemia as a blood glucose level below 70 mg/dL (<3.9 mmol/L). 6 This is a level below which most people secrete counterregulatory hormones and have symptoms of hypoglycemia. A report in the past year noted that people who do not have T1D spend an average of 20 min/day with CGM values between 60 and 70 mg/dL (3.3–3.9 mmol/L). 7 We have thus used the term “true hypoglycemia” to further distinguish glucose levels below 60 mg/dL (<3.3 mmol/L). 8
SH
A confounding factor in determining the actual rate of SH is variation in the definition of SH used in different reports. The ADA defines SH as “an event requiring assistance of another person to administer carbohydrate, glucagon, or other resuscitative actions.” 6 Using this definition, all hypoglycemic events in young children assisted by parents or others would be considered SH. In the intensively treated adolescent (13–17 years old) cohort of the Diabetes Control and Complication Trial, there were 26.7 episodes of coma or seizure per 100 patient-years. This was threefold greater than in the conventionally treated subjects. The mean hemoglobin A1c (HbA1c) level of the intensively treated subjects was 8.06%. 9 Over the next decade, SH leading to loss of consciousness, seizure, or hospital emergency department admission occurred in a specialty center for children with diabetes at a rate of approximately 19 cases per 100 patient-years; 10 common predictors of SH were lower HbA1c values, younger age, underinsurance (defined as a “lack of insurance, receiving Medicaid, participating in the Colorado Resident Discount Program, or having Child Health Plus insurance”), and higher insulin dose. In essence, SH continues to be common.
Approximately 75% of all SH episodes in children occur as nocturnal SH. 11 A recent report of CGM use in children and adults with T1D during 36,000 nights (2.4 million readings) documented chemical hypoglycemia (<70 mg/dL or <3.9 mmol/L) for 20 consecutive min during 18% of nights and values <60 mg/dL (<3.3 mmol/L) for at least 20 consecutive min in 9.6% of nights. 12 In this study, two predictors of hypoglycemia (P<0.001) were an initial low HbA1c value (<7.0% vs. ≥8.0%) and hypoglycemia on the initial blinded CGM tracing.
Etiology
Frequent mechanistic causes of hypoglycemia (adapted in part from Cryer
13
) are: • Increased glucose utilization (e.g., after exercise) • Increased insulin sensitivity (e.g., due to weight loss, after exercise, etc.) • Increased insulin levels during exercise (resulting in impaired glucose release)
14,15
• Impaired counterregulatory hormone responses (especially during sleep)
16
• Inhibition of hepatic glucose output (e.g., after consuming alcohol)
17
• Antecedent hypoglycemia (hypoglycemia begets hypoglycemia)
12
The two major etiological factors for hypoglycemia in people with diabetes have been identified as either insulin excess alone or the combination of insulin excess plus compromised glucose counterregulation. 18 With the technology already potentially available (discussed below), it may be possible to reduce the current incidence of SH by at least half.
Hypoglycemia Unawareness
Hypoglycemia-associated autonomic failure has been extensively studied and described and is frequently stated to be the number one factor associated with SH in adults. 19 Although the exact mechanisms are still unknown, hypoglycemia-associated autonomic failure occurs when recent hypoglycemia impairs autonomic responses to subsequent hypoglycemic episodes, leading to reduced epinephrine secretion as well as reduced neurogenic symptoms of hypoglycemia. Bhatia and Wolfsdorf 20 found a threefold increase in the prevalence of “asymptomatic hypoglycemia” in youth with T1D who experienced SH. It is surprising that when a clinical tool such as the Hypoglycemia Awareness Questionnaire 21 was administered by two pediatric groups, 22,23 the mean occurrence of hypoglycemia unawareness (HUN) was 25% of all interviewed families. This was very similar to the incidence of 23% described in adults. 24 In all three reports, the incidence of SH was higher in the subjects with HUN. Reduced counterregulatory hormone secretion has long been recognized in adults with T1D. 1,18,19 The Diabetes Research in Children Network (DirecNet) group described greatly reduced epinephrine and glucagon responses in children, 4–17 years old, when blood glucose levels were systematically decreased to below 60 mg/dL (<3.3 mmol/L). 25 HUN can usually be reversed, and the epinephrine response to hypoglycemia improved, with careful avoidance of hypoglycemia for at least 2–3 weeks. 26 –28 Unfortunately, hypoglycemia avoidance for as long as 6 months did not result in full restoration of plasma epinephrine responses in TID. 29 Additional features of autonomic neuropathy and postural hypotension predicted even poorer plasma epinephrine responses to hypoglycemia. It is important for both pediatric and adult diabetes care-providers to be alert to the possibility of HUN and any causes of recurrent hypoglycemia in order to avoid hypoglycemia-associated autonomic failure and subsequent SH episodes.
Prevention of Hypoglycemia Now
Mainstays of hypoglycemia prevention have been: 1. Education 2. Frequent self-monitoring of blood glucose (SMBG) levels 3. Use of rapid-acting and basal insulin analogs 4. Use of continuous subcutaneous insulin infusion (CSII) 5. Insulin modifications to prevent exercise-related hypoglycemia 6. Use of CGM
The first three items are essential tools for effective diabetes management and prevention of hypoglycemia and are standards for medical care in T1D. The latter three are still advancing rapidly and becoming increasingly more common in the clinical care of T1D.
1. Education, education, education
The importance of education should never be underestimated. A major reason for quarterly diabetes clinic visits, in addition to monitoring HbA1c levels, is to monitor the frequency of low glucose levels and educate patients and families on possible ways to reduce the frequency of low values.
2. Frequent SMBG levels
Frequent SMBG is necessary to detect hypoglycemia and to make insulin management changes. The ADA recommends SMBG at least three times daily for patients using multiple daily injections (MDI) of insulin or CSII. 30 According to the 1994 ADA Consensus Statement on SMBG, “appropriately timed SMBG is the only practical means of detecting asymptomatic hypoglycemia in the outpatient setting,” and “permits therapy to be modified so as to prevent hypoglycemia.” 31 The Food and Drug Administration currently requires SMBG levels (even in people using CGM) prior to making changes in insulin dosage. Therefore, it can be expected that more frequent SMBG can help prevent future hypoglycemia. This is difficult to document, however, because more frequent SMBG will improve detection of unrecognized hypoglycemia and thus appear to associate SMBG with higher rates of hypoglycemia. 32 –34
3. Use of rapid-acting and basal insulin analogs
The use of insulin analogs has been shown to be a major factor in the decline of SH events while encouraging patients to achieve improved glycemic control. This was found in longitudinal data after the introduction of insulin lispro. 35 A crossover trial comparing human regular insulin with insulin aspart showed a 72% reduction in nocturnal SH using insulin aspart. 36 Similarly, the use of basal insulins (insulin glargine and insulin detemir) has helped to reduce SH, particularly during the night. This has been particularly true for young children, who are less adept at recognizing hypoglycemia. 37
4. Use of CSII
The ADA 38 and the National Institute for Health and Clinical Excellence 39 recommend CSII for patients who fail to achieve euglycemia with MDI of insulin due to prevalence of hypoglycemia. A meta-analysis of 22 randomized controlled trials and before/after studies confirmed that both HbA1c level and the rate of SH were significantly lower during CSII compared with MDI. 40 The greatest improvements from CSII on preventing SH were seen in patients with the highest initial rates of SH when beginning MDI therapy. Predictors of success with using CSII to safely achieve target HbA1c levels were lower HbA1c value, younger age, shorter duration of diabetes, and more frequent daily SMBG measurements at initiation of CSII therapy. In summary, CSII can be indicated as a safer intensive insulin regimen than MDI because of the reduced risk for resultant hypoglycemia, especially SH, as HbA1c levels are decreased.
Recent reports of non-randomized clinic experiences have demonstrated that improved glycemic control can be achieved without an increased risk for SH as patients are transitioned from MDI to CSII therapy. In a retrospective analysis of glycemic outcomes for 291 youth (13.3±3.7 years old) after 1 year of using CSII, an improvement in mean HbA1c levels (from 8.7±1.3% to 8.2±0.9% [P<0.0001]) was found. 41 The mean number of SH events decreased from 0.54±1.09 events per subject per year prior to CSII to 0.30±0.80 events per year after CSII (P=0.0003). For patients continuing CSII therapy for greater than 1 year, a significant reduction in HbA1c values was sustained for each additional year of CSII use up to 8 years. A similar retrospective study in 421 adults and youth with T1D showed a sustained decrease in HbA1c levels with CSII without increased rates of hypoglycemia. 42
Improvement in HUN has also been reported as a result of the use of CSII. In a recent prospective pilot study in T1D patients with repeated non-SH or SH, CSII use was associated with reduced SH and non-SH, improvement in HUN, reduced mean amplitude of glycemic excursions, and better quality of life. 43
5. Insulin modifications to prevent exercise-related hypoglycemia
The main known identified factor associated with nocturnal SH in youth is previous daytime exercise. 11,20 No one questions the importance of daily exercise in youth—for the prevention both of obesity and of cardiovascular disease. How then can insulin dosages be modified in subjects with T1D to prevent exercise-induced hypoglycemia? Three recent exercise studies using the DirecNet exercise protocol have pointed to helpful prevention methods for youth using an insulin pump. 44 –46 In the first DirecNet study, 44 50 youth were randomized to have one exercise admission in a clinical research center and one sedentary admission. Nocturnal glucose values fell below 60 mg/dL (<3.3 mmol/L) during 48% of the exercise admissions and during 28% of the sedentary admissions. Thus, nocturnal hypoglycemia was clearly shown to be more frequent as a result of 1 h of afternoon (4 p.m.) standardized exercise.
In the second study, 45 the randomized discontinuation of insulin during the exercise resulted in a lower likelihood of hypoglycemia during the exercise (16%) compared with when the same 49 youth on another visit received their usual basal insulin during the exercise (43%). The prevention effect would likely have been greater had the basal insulin been decreased starting 30 min prior to the exercise. Individual subjects have varying needs and may need slightly different alterations. Thus, a simple insulin reduction or pump suspension during exercise can significantly reduce the risk for hypoglycemia during exercise. Unfortunately, blood glucose levels were not measured during the night in the second study to determine the effect on nocturnal hypoglycemia.
A similar study by Admon et al. 47 randomized 10 youth (10–19 years old) to have either the pump on at 50% basal insulin or the pump off with total basal insulin suspension during 40–45 min of exercise. Based on CGM tracings during exercise and for the following 24 h, there was not a significant difference in acute or late hypoglycemia between the two groups. Late hypoglycemia was more common than hypoglycemia during exercise, and pump on was associated with an elevated (although not statistically significant) risk for late hypoglycemia compared with pump off.
A third study using the DirecNet exercise protocol 47 was done to evaluate methods to reduce the 48% incidence of nocturnal glucose levels below 60 mg/dL (<3.3 mmol/L) by either (1) discontinuing insulin during the exercise (group A) or (2) discontinuing the insulin during the exercise plus use of a 20% basal insulin reduction from 9 p.m. to 3 a.m. (group B). In treatment group A, there were five episodes with glucose levels <70 mg/dL (<3.9 mmol/L). In treatment group B, there was only one episode with a glucose value <70 mg/dL (<3.9 mmol/L). In both groups, no subjects had values below 60 mg/dL (<3.3 mmol/L) during the night. Thus, methods are now available to reduce the incidence of hypoglycemia during exercise as well as the exercise-associated nocturnal hypoglycemia (often referred to as “delayed hypoglycemia”). Reduction of hypoglycemia in both instances should also help to reduce the likelihood of SH. The ease of insulin modifications with exercise should now be considered one of the main advantages of insulin pump therapy in youth. Similar modifications are possible with injection therapy, but they are more difficult to implement.
6. Use of CGM
Since the Diabetes Control and Complication Trial report, 48 physicians have encouraged patients to attain tighter glycemic control to prevent the micro- and macrovascular complications of diabetes. There are now multiple reports of short-term 49,50 and long-term 51 –57 randomized clinical trials of CGM use that have included adult and/or pediatric subjects. In an early short-term trial, Garg et al. 49 showed that time spent in hypoglycemia decreased by 21% in subjects using CGM with real-time values displayed on the device compared with control subjects not using CGM. Nocturnal hypoglycemia was also significantly reduced for glucose values <55 mg/dL (3.1 mmol/L; 38% reduction; P<0.001) and between 55 to 80 mg/dL (3.1–4.4 mmol/L; 33% reduction; P<0.001).
A major barrier in using CGM to reduce nocturnal hypoglycemia is the lack of patient responsiveness to alarms at night. Using an infrared camera to videotape 20 subjects (4–17 years old) using a real-time CGM device at night (9 p.m. to 7 a.m.), Buckingham et al. 58 found that subjects awoke to only 29% of individual alarms and to 66% of alarm events. Small children (4–11 years old) responded to 17–20% of alarms, whereas adolescents and parents responded to 53% and 37% of alarms, respectively. Of the 11 events when the glucose was confirmed to be ≤70 mg/dL, however, each subject awoke.
The long-term trials were primarily aimed to reduce HbA1c levels or time spent in hypoglycemia. A common finding from these studies was that more frequent use of the CGM devices was associated with a greater decline in HbA1c levels. An additional finding was that, with the exception of one study, 54 the incidence of SH did not increase with the reduction in HbA1c levels. This is in contrast to the Diabetes Control and Complications Trial, when SH increased threefold as HbA1c levels declined. 9 It is surprising that in the Juvenile Diabetes Research Foundation cohort of children and adults with HbA1c levels <7.0%, the introduction of CGM resulted in significantly less time spent in hypoglycemia as well as lower HbA1c levels. 53 The overall incidence of SH in subjects using CGM (with CSII or MDI) in the primary Juvenile Diabetes Research Foundation cohort was 17.9 per 100 patient-years compared with 24 per 100 patient-years in the control group monitoring BG levels with a home glucose meter (P=0.64). 52 In the STAR-3 study, with significant (P<0.001) reductions in HbA1c levels in all subjects, the overall incidence of SH when an insulin pump and CGM were used was 13.31 per 100 patient-years compared with 13.48 per 100 patient-years in the injection therapy/SMBG group (P=0.84). 56 Subjects having more than one SH episode in the previous year were not included in the study. In summary, the use of CGM (with and without CSII) may result in a “relative” reduction in hypoglycemia as glycemic control improves.
A recent study in youth 59 demonstrated that CGM can be an effective tool for reducing hypoglycemia frequency and thus helping to reverse HUN. Many health insurance companies now ask for information related to SH as the basis for approving CGM. As HUN has been a major reason given for considering islet/pancreas transplantation, 60 the use of CGM should now be appropriately tried first.
A drawback of current CGM systems is noted by Zucchini et al, 61 in which 55 youth with T1D wore a CGM system for three consecutive days with only 27 of 68 low SMBG values detected by the sensor (sensitivity 44%). Therefore, continued improvement in the accuracy of sensor systems will be essential to its utility as a tool for hypoglycemia detection and prevention. Meanwhile, additional methods of measuring glycemic control are being developed. As postprandial glucose levels relate most closely to HbA1c values in people with well-controlled T1D, new techniques to evaluate postprandial glucose excursions may be helpful. 62
Prevention of Hypoglycemia in the Future
Several methods of preventing hypoglycemia currently under investigation are likely to be important in the prevention of hypoglycemia in the future.
Discontinuation of insulin for 2 h when a set low glucose value has been reached
This feature is already being used in Europe as a function of the Medtronic MiniMed (Minneapolis, MN) Paradigm® Veo™ insulin pump (Fig. 1). 63 Numerous studies have shown that it is safe to discontinue insulin therapy for 2 h without significant ketosis or acidosis. 64 –71 Suspension of CSII in eight subjects resulted in an increase in the mean serum β-hydroxybutyrate level from 0.13±0.07 mmol/L at baseline to 0.36±0.27 mmol/L after 2 h and of 0.63±0.36 mmol/L after 3 h of pump suspension (with an increase in the plasma glucose of 51 mg/dL [2.8 mmol/L]). 67 In a study by Castillo et al., 69 the mean serum β-hydroxybutyrate level increased by approximately 0.3 mmol/L after 2 h and by approximately 0.5 mmol/L after 3 h of pump suspension in five subjects who were hypoglycemic (approximately 35 mg/dL [1.94 mmol/L]) at the time of pump suspension. None of these increases in β-hydroxybutyrate levels was of clinical significance.

Continuous glucose monitoring tracing of a patient using the Medtronic Paradigm Veo insulin pump with the Low Glucose Suspend feature activated. On two occasions, the Low Glucose Suspend was activated when threshold sensor glucose values were reached. Severe hypoglycemia was avoided, without any resultant ketosis from the 2-h insulin suspension. BG, blood glucose; Hypo, hypoglycemia. This figure was provided by Dr. Barry Keenan from Keenan et al.
63
and is reproduced with permission of Pediatric Endocrinology Review. Color images available online at
Discontinuation of insulin for 2 h when a low glucose value is predicted
Recent research has shown that 84% of nocturnal hypoglycemic episodes can be prevented using a low-glucose prediction algorithm. 65 Figure 2 shows two randomized admissions for the same person in which a temporary insulin pump suspension was triggered by predicted hypoglycemia through a combination of hypoglycemia prediction algorithms. It is likely that SH will be greatly reduced in the future as a result of insulin discontinuation with a predicted low glucose level and, if that fails, the use of a low glucose threshold to discontinue insulin administration. Initial data from 338 patients with T1D showed that the use of a combination of a “predictive” and a “low glucose suspend” algorithm resulted in a 36.6% reduction in time spent <70 mg/dL (<3.9 mmol/L) and a 43.4% reduction in time spent <60 mg/dL (<3.3 mmol/L). 72 Using the combination of these two algorithms could save lives and improve the quality of life for children and adults who have previously experienced nocturnal SH. Lessening the fear of SH and consequent hypoglycemia avoidance behaviors may then result in improved glycemic control and lower risk for diabetes complications.
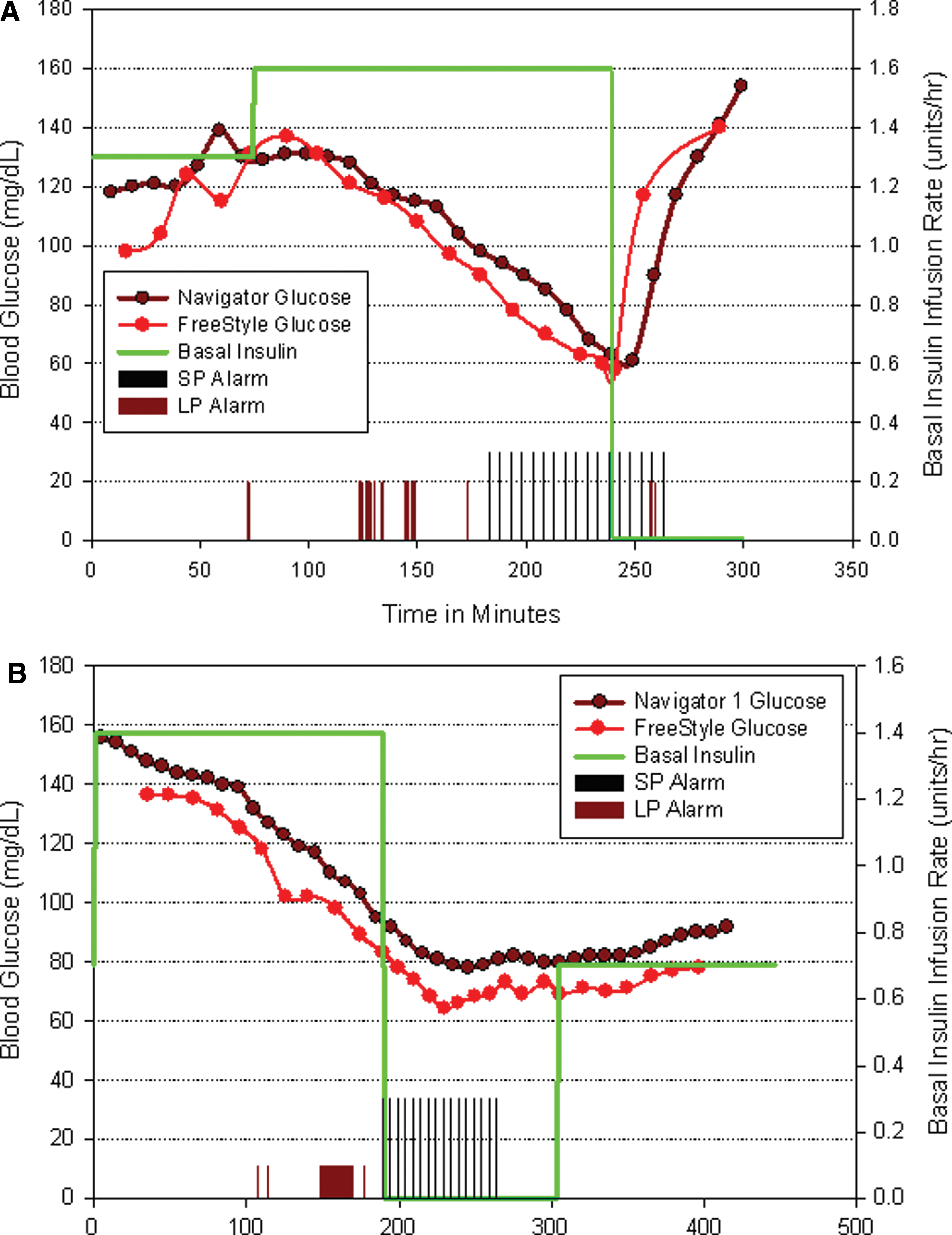
Unpublished data from two separate hospital admissions for the same subject. (
Closed-loop systems
Hypoglycemia prediction algorithms and insulin modification regimens are precursors to the eventual development of a closed-loop system that incorporates CGM and CSII technology to automatically regulate glycemic control. Recent advances in closed-loop technology have included algorithms for predicting and preventing hypoglycemia with more nuanced adjustment of insulin delivery or through bihormonal systems that infuse both glucagon and insulin.
The proportional integrative derivative algorithm adjusts insulin delivery based on rate of change and the absolute value of CGM sensor glucose in relation to preset target ranges. 73 Various model predictive control algorithms have been applied to the prediction of glucodynamics and insulin analog pharmacokinetics in order to automatically adjust insulin infusion based on detected changes in blood glucose levels. 74 –78 These studies have shown model predictive control algorithms to be superior to CSII alone in reducing the time spent with nocturnal blood glucose levels <70 mg/dL (3.9 mmol/L) and in minimizing postprandial glycemic excursions. 76 In addition, bihormonal closed-loop systems that infuse glucagon as well as insulin have been shown to be effective in preventing blood glucose levels <70 mg/dL (3.9 mmol/L). 79 –81
Many challenges remain for the development of a fully automated closed-loop system. These challenges include reducing the delay between glucose sensing and insulin delivery, improvements in CGM sensor accuracy, proving the clinical accuracy of control algorithms, further research in bihormonal delivery systems, and the development of ultra-rapid-acting insulin analogs.
Preservation of C-peptide/insulin production
The Diabetes Control and Complications Trial clearly showed that SH and diabetes complications were less likely in people with T1D who were still able to produce C-peptide (as a measure of remaining insulin production). 82 It has also been shown that C-peptide production could be preserved with the use of a closed-loop Biostator (Life Science Instruments Miles Laboratories, Ventura, CA) following the diagnosis of T1D. 83 Sensor-augmented pump therapy initiated within 4 weeks of T1D diagnosis has been shown to partially preserve C-peptide secretion in 12–16-year-old patients after 12 months, compared with those treated with an insulin pump alone (P=0.033). 84 Research in progress is supported jointly by TrialNet and DirecNet (both funded by the National Institutes of Health) using the Medtronic closed-loop system for a minimum of 72 h in the first week after diagnosis of T1D. The Medtronic insulin pump and CGM (sensor-augmented pump) are then used on discharge from the clinical research center and for the next 2 years to determine if C-peptide production is preserved. Although the results will not be known for several years, initial data from a patient in this study are shown in Figure 3. It is possible that preserving C-peptide production with closed-loop technologies could contribute to a reduction in the incidence of SH. 82
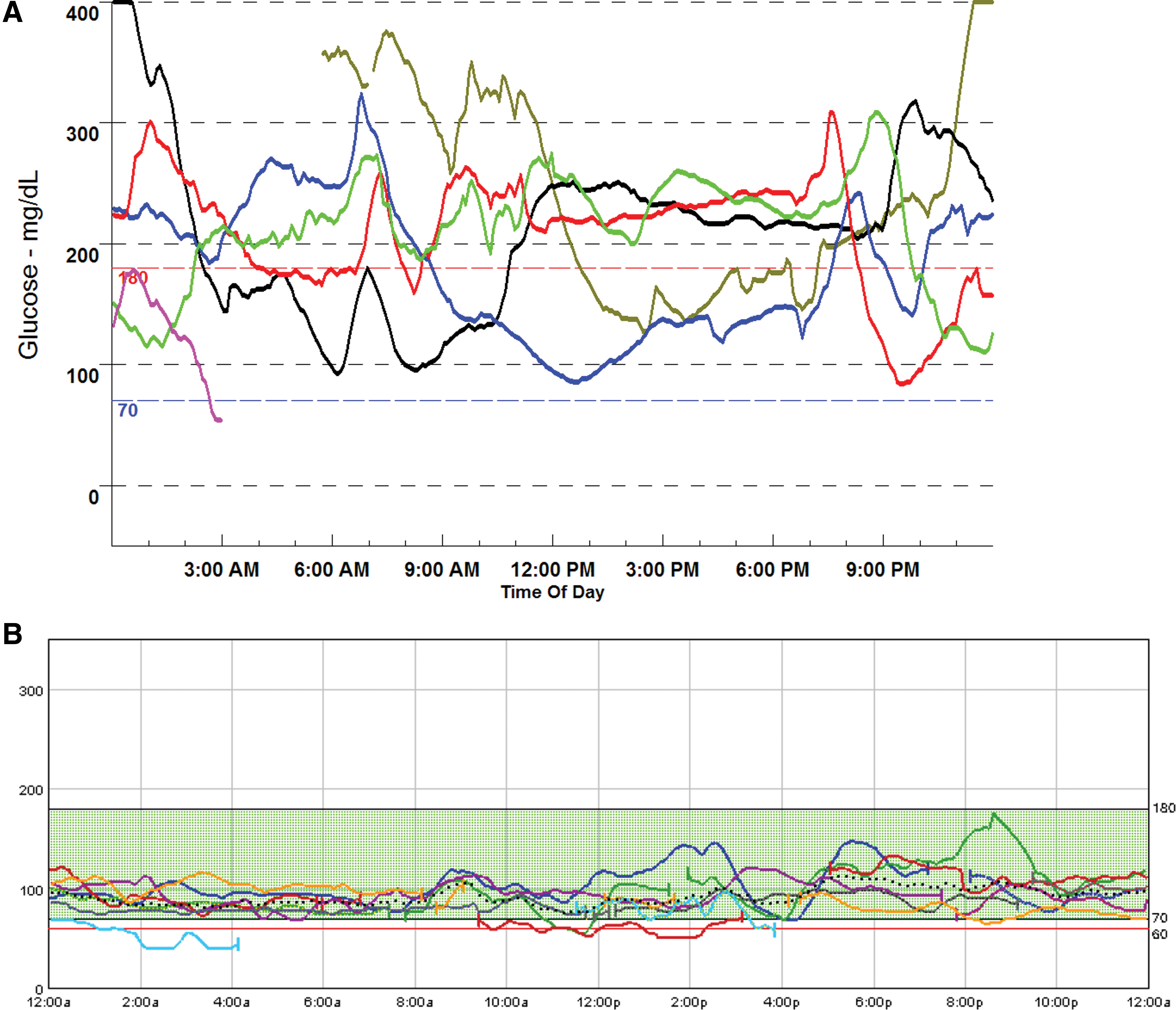
Unpublished data from Medtronic Paradigm CGM tracings of the same patient (
It may also be possible to preserve C-peptide production in newly diagnosed subjects with T1D using various immunomodulatory therapies. The rationale for the use of monoclonal antibodies is to preserve remaining β-cell function by selectively depleting the cells involved in the autoimmune attack on the pancreas. Short-term therapy with anti-CD3 antibodies (ChAglyCD3) initiated within 6 weeks of diagnosis of T1D has demonstrated partial preservation of C-peptide production for at least 18 months and a more gradual rate of loss of C-peptide secretion. 85 The use of rituximab, an anti-CD20 antibody, has also been shown to partially preserve C-peptide production for 1 year in patients with new-onset T1D. 86 Another immunomodulatory approach to preserve residual C-peptide production involves the use of major diabetes-related autoantigens such as insulin 87 or glutamic acid decarboxylase (GAD) (65-kDa subunit). 88 Ludvigsson et al. 88 found that treatment with 65-kDa GAD was effective in reducing the loss of C-peptide production for up to 30 months in newly diagnosed patients (<18 months in duration) with T1D. However, a more recent report by Wherrett et al. 89 found that treatment with two or three injections of GAD-alum in people newly diagnosed (<100 days in duration) with T1D was not effective in preserving C-peptide production after 1 year compared with the control group. Future goals for research with these agents will be to determine their efficacy in long-term preservation of C-peptide/insulin production and thus in the prevention of SH.
Summary
Recent developments have provided tools to reduce the likelihood of SH. It is also likely that future developments will result in further reductions in SH as well as in better glycemic control.
Footnotes
Acknowledgments
This work was supported in part by a research grant from the Juvenile Diabetes Research Foundation International.
Author Disclosure Statement
No competing financial interests exist.