
Abstract
Background:
The purpose of this study was to evaluate the effect of the duodenal–jejunal bypass liner (DJBL), a 60-cm, impermeable fluoropolymer liner anchored in the duodenum to create a duodenal–jejunal bypass, on metabolic parameters in obese subjects with type 2 diabetes.
Methods:
Twenty-two subjects (mean age, 46.2±10.5 years) with type 2 diabetes and a body mass index between 40 and 60 kg/m2 (mean body mass index, 44.8±7.4 kg/m2) were enrolled in this 52-week, prospective, open-label clinical trial. Endoscopic device implantation was performed with the patient under general anesthesia, and the subjects were examined periodically during the next 52 weeks. Primary end points included changes in fasting blood glucose and insulin levels and changes in hemoglobin A1c (HbA1c). The DJBL was removed endoscopically at the end of the study.
Results:
Thirteen subjects completed the 52-week study, and the mean duration of the implant period for all subjects was 41.9±3.2 weeks. Reasons for early removal of the device included device migration (n=3), gastrointestinal bleeding (n=1), abdominal pain (n=2), principal investigator request (n=2), and discovery of an unrelated malignancy (n=1). Using last observation carried forward, statistically significant reductions in fasting blood glucose (−30.3±10.2 mg/dL), fasting insulin (−7.3±2.6 μU/mL), and HbA1c (−2.1±0.3%) were observed. At the end of the study, 16 of the 22 subjects had an HbA1c<7% compared with only one of 22 at baseline. Upper abdominal pain (n=11), back pain (n=5), nausea (n=7), and vomiting (n=7) were the most common device-related adverse events.
Conclusions:
The DJBL improves glycemic status in obese subjects with diabetes and therefore represents a nonsurgical, reversible alternative to bariatric surgery.
Introduction
Treatment of diabetes is focused on glycemic control and typically proceeds in a stepwise fashion when target glycemic goals are not reached or maintained. 7,8 The initial steps are lifestyle changes aimed at controlling diet and increasing activity with the goal of reducing body weight, followed by the addition of orally active pharmacologic agents (sulfonylureas, metformin) and insulin to the treatment regimen. 7,8
Of interest is the observation that obese patients with diabetes who undergo certain gastric bypass procedures demonstrate improvement in glycemia, often within days of surgery and before significant weight loss. 9,10 The mechanism responsible for this improvement is not fully understood; however, the surgical rearrangement of the anatomy of the gastrointestinal (GI) tract changes the location where partially digested nutrients first contact the intestine, suggesting that correction of dysfunctional homeostatic mechanisms may contribute to the glycemic improvement. 11
A nonsurgical method of altering the location of the initial contact of partially digested nutrients with the intestine is by use of the duodenal–jejunal bypass liner (DJBL). 12,13 The DJBL consists of a 60-cm, impermeable fluoropolymer liner and a nitinol anchor, which reversibly fixes the device to the wall of the duodenum. The DJBL is open at both ends and functions to prevent the partially digested food from contacting the proximal intestine. A pilot study of the DJBL in obese subjects with type 2 diabetes resulted in a mean reduction of 50 mg/dL in fasting plasma glucose (FPG) after 1 week that was sustained through 24 weeks. 14 Here we describe a 52-week study that was designed to investigate the effect of the DJBL on metabolic parameters in obese subjects with type 2 diabetes.
Subjects and Methods
Ethics
This study was conducted in compliance with international guidelines and local country regulations. The study protocol and subject informed consent forms were reviewed and approved by the Ethics and Research Committee of the University of São Paulo, São Paulo, Brazil. All subjects or their legal guardians provided written informed consent prior to participation in the study.
Subjects
Male and female subjects with type 2 diabetes between the ages of 18 and 65 years who had a BMI of ≥40 and <60 kg/m2 were eligible for inclusion in the study. Exclusion criteria included use of prescription anticoagulation therapy, iron deficiency or iron deficiency anemia, inflammatory bowel disease or other GI disease, pancreatitis, symptomatic coronary artery disease or pulmonary dysfunction, known gallstones, severe coagulopathy, upper GI bleeding conditions (e.g., esophageal or gastric varices, congenital or acquired intestinal telangiectasia), congenital or acquired anomalies of the GI tract (e.g., atresias or stenoses), inability to discontinue nonsteroidal anti-inflammatory drugs during the study, previous GI surgery that could interfere with placement of the device, or family or patient history of a known diagnosis or symptoms of systemic lupus erythematosus, scleroderma, or other autoimmune connective tissue disorder.
Study design
The study was a 52-week, prospective, open-label, single-center clinical trial intended to assess the safety and efficacy of the DJBL in obese subjects with type 2 diabetes. Following screening and up to 30 days prior to implanting the DJBL, baseline demographics and medical history were obtained. Excess body weight was calculated as the amount of body weight that exceeded a BMI of 25 kg/m2. In addition, a physical examination, electrocardiogram, chest x-ray, liver, biliary duct, and pancreas ultrasound, upper GI endoscopy, and fasting blood tests were conducted. A schedule of study assessments and activities is presented in Figure 1. In accordance with the protocol, all subjects received nutritional counseling at the baseline visit and at all monthly follow-up visits. Baseline counseling consisted of a 30-min visit with a study nurse to discuss nutritional, behavioral, and lifestyle modifications recommended throughout the study. At follow-up visits, subjects were only asked if they were following their diet, and results were recorded. Therefore, nutritional counseling was minimal at the post-implant follow-up visits. During the period starting 3 days prior to device implantation and ending 2 weeks after explantation of the device, subjects were instructed to take an over-the-counter proton pump inhibitor (40 mg twice a day). Daily multivitamin and iron supplements were also recommended throughout the study. Subjects were instructed to follow a liquid diet during the first 2 weeks following implantation and to gradually transition to a normal diet over the next 10 days. Follow-up examinations were to be conducted 1, 3, and 6 months after the explantation of the device.

Schedule of study assessments. BL, baseline; BMI, body mass index; GI, gastrointestinal.
Device implantation and explantation
All device implantations were performed with the patient under general anesthesia using a minimally invasive endoscopic procedure. 13 At the end of the study period (or earlier if indicated by an adverse event), the DJBL was removed endoscopically using a custom grasper passed through the working channel of a standard endoscope with the patient under conscious sedation for 21 of 22 subjects; one subject required general anesthesia.
The DJBL (EndoBarrier Gastrointestinal Liner®) and the implantation and removal devices were manufactured by GI Dynamics, Inc. (Lexington, MA).
Statistical analyses
Several subject populations were included in the analyses. The safety analysis population included all subjects in whom an implant procedure was attempted. The full efficacy analysis population included all enrolled subjects in whom an implantation was successful. The completer population included all subjects who completed the 52-week implantation period.
The study had two primary efficacy end points: percentage change in excess body weight and change in type 2 diabetes status, including hemoglobin A1c (HbA1c) and fasting blood glucose and insulin levels. Secondary efficacy end points included changes in blood lipid levels and blood pressure.
All statistical analyses were performed using SAS® version 9.2 or later (SAS Institute, Cary, NC). Efficacy variables were evaluated as a change from baseline. Missing values were not imputed. However, last observation carried forward (LOCF) on or before explantation was also used when calculating change from baseline. A P value (calculated using Student's t test) of ≤0.05 was considered statistically significant.
Results
Twenty-two subjects were screened, and all were enrolled in the study. The baseline characteristics of the study subjects are presented in Table 1. At baseline, 17 of 22 subjects were receiving drugs to control their diabetes, including 11 receiving metformin alone, two receiving glibenclamide alone, two receiving chlorpropamide alone, one receiving metformin plus glibenclamide, and one receiving metformin plus acarbose. A DJBL was successfully implanted in all subjects, with the procedure taking an average of 26.7±11.0 min (range, 13–52 min).
Data are mean±SD values.
BMI, body mass index; GERD, gastroesophageal reflux disease; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Thirteen subjects completed the 52-week period, and 18 subjects completed at least 24 weeks. The mean duration of the implant period for all subjects was 41.9±3.2 weeks. The reasons for early removal of the device were migration or rotation of the device (n=3; 36, 36, and 48 weeks post-implantation), GI bleeding (n=1; 4 weeks post-implantation), abdominal pain (n=2; 21 and 30 weeks post-implantation), and principal investigator request due to subject's noncompliance with study visits (n=2; 20 and 32 weeks post-implantation). The device was removed from one subject who presented with fever and mild abdominal symptoms 17 weeks after implantation. Subsequent computed tomography scan revealed a 30-cm abdominal tumor that was identified as metastatic ovarian cancer. This event was considered not related to the device.
Baseline FPG, fasting plasma insulin, and HbA1c levels are presented in Table 1, and changes in these parameters are shown in Table 2. Reductions in FPG were seen as early as week 1 and reached statistical significance at week 24. At week 52, the completer population demonstrated a decrease in plasma glucose of −37.1±11.8 mg/dL (mean±SEM, P<0.01). A similar reduction was seen in the full analysis population using LOCF analysis (Table 2). Mean HbA1c was statistically significantly decreased by week 24 and remained statistically significantly decreased thereafter (Table 2). The decrease in HbA1c was evident in subgroups of subjects with baseline HbA1c<8%, 8% to<10%, and ≥10% (Fig. 2). The progressive improvement in HbA1c is illustrated in Figure 3. At baseline, only one subject (4.5%) had an HbA1c level below 7%. For final HbA1c measurement, 16 of 22 subjects (73%) had an HbA1c below 7%. In the nine subjects who experienced an early device explantation, HbA1c decreased from 8.9±0.5% at baseline to 7.2±0.4% at final measurement (median, 28 weeks).
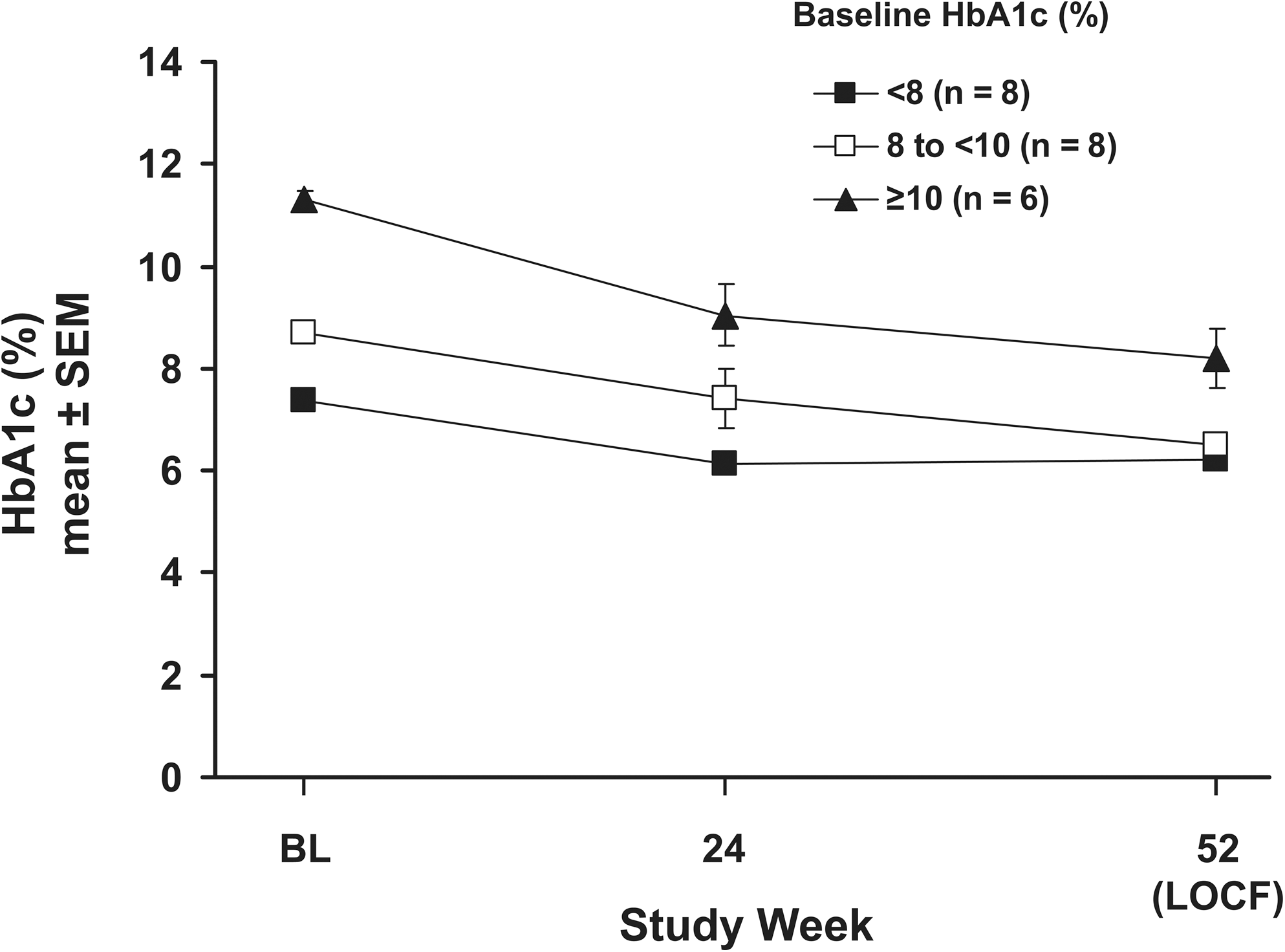
Change in hemoglobin A1c (HbA1c) in subgroups of subjects. No statistical analysis was performed on these data. SE bars are hidden within symbols at some time points. BL, baseline; LOCF, last observation carried forward.
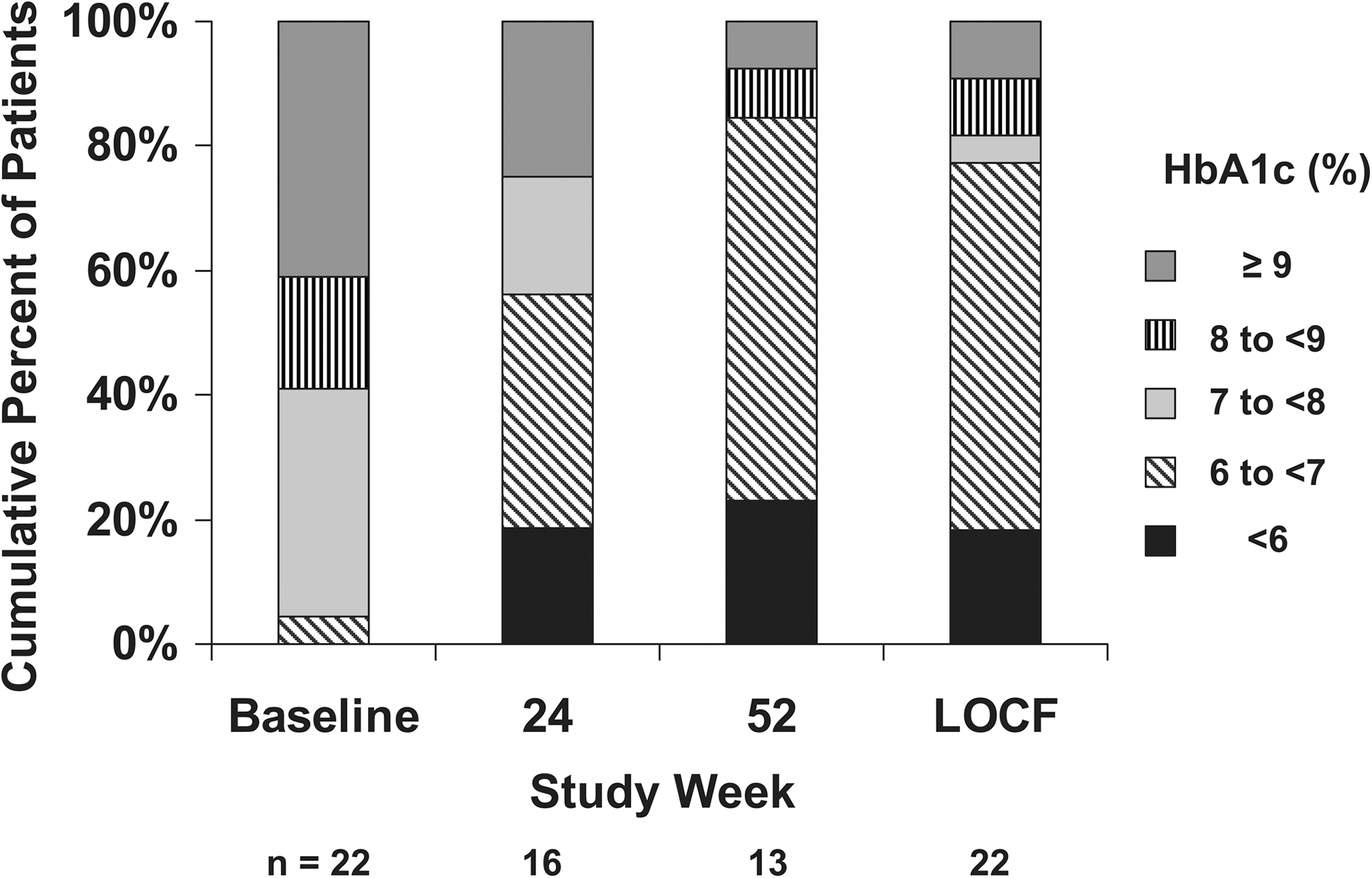
Distribution of hemoglobin A1c (HbA1c) levels during the study. LOCF, last observation carried forward.
Data are mean±SEM values (number of patients).
P<0.01, b P<0.001, c P<0.0001, d P<0.05 for change from baseline.
HbA1c, hemoglobin A1c; LOCF, last observation carried forward.
During the study, nine subjects experienced no change in their diabetes medications, three subjects reduced their dose of metformin, and one subject stopped other diabetes medication. One subject who was previously untreated began treatment with metformin, five subjects increased their dose of metformin, and three subjects added an additional drug to their treatment regimen.
Figure 4 shows the percentage change in excess body weight observed during the study. The 13 subjects who completed the study weighed 121.8±7.6 kg (mean± SE) at baseline and 101.6±5.7 kg at week 52. This change represented a mean loss of excess body weight (percentage excess weight loss) of 39.0±3.9% (P<0.0001). In the full analysis population using LOCF, the mean percentage excess weight loss was 35.5±3.1% (P<0.0001). The reduction in excess body weight (LOCF) was reflected by reductions in BMI and waist circumference of −6.7±0.7 kg/m2 and−13.0±1.7 cm, respectively.
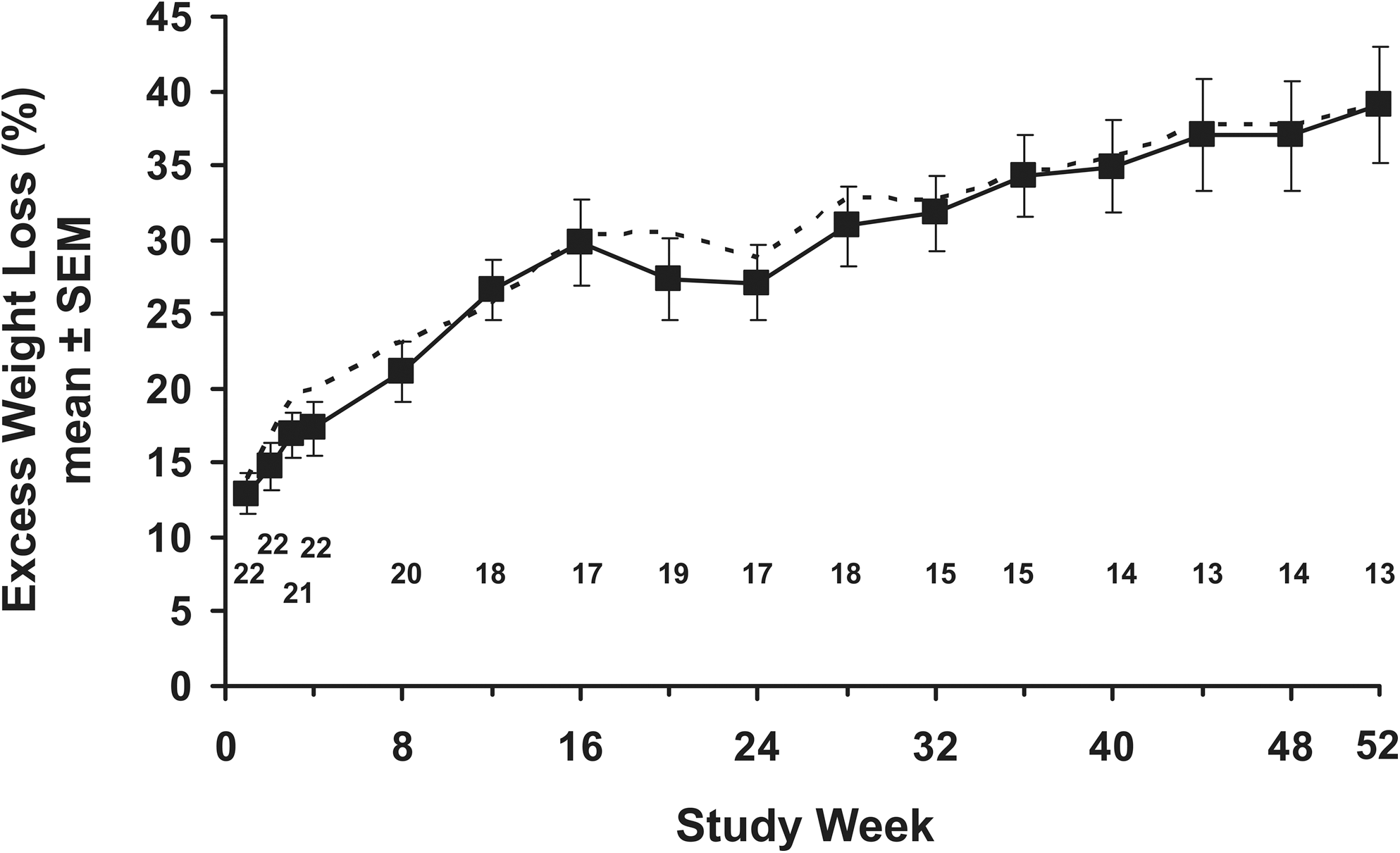
Percentage excess weight loss by visit. The number of subjects represented by each point is shown above the x-axis. The dotted line reflects the loss of excess body weight in the completer population during the study.
Blood levels of total cholesterol, low-density lipoprotein cholesterol, and triglycerides were significantly reduced during the study (Table 3). Nonsignificant decreases in mean systolic (6.6±4.4 mm Hg, P=0.15, LOCF) and diastolic (−1.6±3.5 mm Hg, P=0.65, LOCF) blood pressure were observed during the study.
Data are mean±SEM values (number of patients).
P<0.05, b P<0.01 for change from baseline.
HDL, high-density lipoprotein; LDL, low-density lipoprotein; LOCF, last observation carried forward; TG, triglycerides.
Sixteen subjects had HbA1c measured 3 and/or 6 months after explantation of the DJBL. These subjects demonstrated a mean decrease in HbA1c during the original 52-week study of −2.3±0.4%. Three and 6 months after removal of the device, their mean changes from baseline were −2.3±0.3% (n=15) and −1.7±0.7% (n=11), respectively.
All 22 subjects reported at least one treatment-emergent adverse event. Treatment-emergent adverse events that occurred in ≥10% of the subjects are presented in Table 4. The most common adverse events that were deemed to be possibly or probably related to the device or procedure were GI disorders, including upper abdominal pain, nausea, and vomiting. With one exception, all adverse events were mild or moderate in severity. The one exception was the 43.5-year-old white woman in whom metastatic ovarian cancer was discovered 17 weeks after device implantation (see above). No deaths occurred during the study.
HDL, high-density lipoprotein.
Discussion
The present study represents the longest evaluation of the safety and efficacy of the DJBL in obese patients with type 2 diabetes. The mean duration of the DJBL implant was 41.9 weeks; 18 subjects completed at least 24 weeks, and 13 subjects completed the entire 52-week study. During the 52-week study, substantial improvements in diabetes status were seen as shown by the decreased blood glucose and HbA1c levels in the study population (Table 2 and Figs. 2 and 3). The improvement in glycemic control is convincingly demonstrated by the results presented in Figure 3, which shows that the percentage of subjects with HbA1c <7% at baseline improved from 4.5% to 73.0% at final study assessment. It is important that the improvements in HbA1c were seen regardless of baseline value (Fig. 2).
A single previous study of the DJBL for the treatment of type 2 diabetes has been reported. 14 In that pilot study, 12 obese patients with type 2 diabetes received a DJBL, and a comparable control group of six patients underwent a sham procedure. After 1 week, FPG had declined significantly in the DJBL group (−50±18 mg/dL, mean±SE) compared with the sham group (+25±29 mg/dL, P=0.042). In addition, postprandial glucose excursions were improved in the DJBL group but not in the sham group. Of interest is the observation that at the 1-week time point, the improvement in glucose metabolism seen in the DJBL could not be explained by changes in body weight, as both groups had experienced the same median weight change from baseline (about −3.5 kg). The improvements in glucose metabolism were sustained through the end of the study (mean, 200±22 days [28.6 weeks]). At week 24, FPG had declined by 83±39 mg/dL (from a baseline of 199±71 mg/dL), and HbA1c had declined by 2.4±0.7% (from a baseline of 9.2±1.7%).
Other clinical studies provide anecdotal observations of the effect of the DJBL on type 2 diabetes. In the initial 12-week study of the DJBL, four of the 12 obese subjects had type 2 diabetes; 15 the authors reported that “all 4 diabetic patients had normal FPG levels without hypoglycemic medication for the entire 12 weeks. Of those 4 patients, 3 had decreased hemoglobin A1c of 0.5% by week 12.” A second study enrolled 40 obese subjects who were candidates for Roux-en-Y gastric bypass and randomly assigned them to either DJBL (n=26, 25 implanted) or low-calorie diet alone (n=14) with the objective of weight loss before surgery. 16 Three subjects with type 2 diabetes were included in the DJBL group, and one was included in the diet group. After 12 weeks, two of the three DJBL subjects demonstrated decreases in HbA1c, and the third, who had a baseline HbA1c of 5.5%, was able to discontinue diabetes medications within 1 week of implantation. A similar 12-week study randomly assigned obese subjects to either DJBL (n=30) or low-calorie diet (n=11). 13 Eight subjects with type 2 diabetes were included in the DJBL group and demonstrated a reduction in mean HbA1c from 8.8±1.7% at baseline to 7.7±1.8% after 12 weeks (P reported as nonsignificant). Six of the eight subjects were able to reduce their dosage of oral diabetes medication or insulin after 1 week, and at 12 weeks, one subject had completely stopped taking antidiabetes medications.
In the present study, device-related early removal of the DJBL occurred in six of the 22 (27%) subjects after a median of 31 weeks. There were three non–device-related early removals: one after 17 weeks due to a metastatic ovarian tumor and two (weeks 20 and 32, respectively) due to principal investigator request as subjects were noncompliant with study visits. In previous studies, device-related early explantation occurred in 15–33% of subjects after a median of 21 days (range, 3–120 days, n=18). 12 –16 Although the early explantation rate of the present study was high, these subjects still derived a metabolic benefit from the DJBL; at their last measurement, HbA1c was 7.2% compared with a baseline value of 8.9%.
Based on the safety results of previous clinical studies of the DJBL, no unanticipated adverse events were observed. The primary device-related safety issues seen in the present study were GI pain, nausea, vomiting, and back pain (Table 4). All cases were mild to moderate in severity. Two subjects cited abdominal pain as the reason for requesting early explantation of the device. It is important that the rates of GI or abdominal pain adverse events appeared to be similar to those reported in previous studies, suggesting that the longer implant duration of the present study was not responsible for an increased incidence of these events.
The mechanism responsible for the improvement in type 2 diabetes in this and previous studies is not well understood. However, the rapid improvement in plasma glucose and insulin levels suggests that the reduction in body weight was not solely responsible. This rapid metabolic response has been observed in many studies of gastric bypass surgery, suggesting that rearrangement of GI anatomy plays a role. 9,10,17 Hickey et al. 18 suggested that dysregulated neuroendocrine signaling between the proximal intestine and pancreas might participate in the insulin resistance of type 2 diabetes and that bypassing a portion of the foregut may interrupt this abnormality. Incretins, like glucagon-like peptide-1 and glucose-dependent insulinotropic peptide, have been implicated in this response, 19 as has a yet-to-be-identified counterregulatory substance. 11
The results of this study leave several questions unanswered. The first is how long does the antidiabetes response last after removal of the device? The results from 11 subjects indicated that the HbA1c response continued for up to 6 months after device removal. It is tempting to speculate that the stability of the response is an indication of a “resetting” of glucose homeostasis, but no data from this study support this concept. Clearly, the weight loss may have contributed to the durability of the response. Although these results are similar to results reported for bariatric surgery, the study provides no information regarding the relative efficacy and safety compared with the surgical procedures. Finally, the study results provide no information about the biologic mechanisms that contribute to the improvement in glycemic control.
Study Limitations
The study was not randomized and did not include a control group. Therefore, it is possible that behavioral changes in the subjects may have contributed to some of the benefits observed. The pharmacologic treatment of type 2 diabetes was not specified or standardized in this study, and changes in antidiabetes drug regimens may have influenced the results. Finally, the study was small, and device-related early explantation of the DJBL was required in 27% of patients.
Conclusions
The results of this study provide clear evidence that the DJBL can improve glycemic status and cardiometabolic factors in obese subjects with type 2 diabetes and that it therefore may represent a nonsurgical and reversible alternative to bariatric surgery and an effective adjunct to pharmacotherapy in the treatment of diabetes.
Footnotes
Acknowledgments
GI Dynamics paid for professional medical writing and editorial assistance that was provided by Edward Weselcouch, Ph.D., of PharmaWrite (Princeton, NJ). The authors participated fully in the planning and drafting of this manuscript and are fully responsible for its content. GI Dynamics reviewed the final draft of this manuscript to ensure the accuracy of the data reported from this company-sponsored clinical trial. Finally, the authors would like to thank Dr. Lee Kaplan for his discussions regarding the manuscript.
Author Disclosure Statement
No competing financial interests exist.