
Abstract
Background:
Hypoglycemia can be a symptom in patients with Addison's disease. The common regimen of replacement therapy with oral glucocorticoids results in unphysiological low cortisol levels in the early morning, the time of highest insulin sensitivity. Therefore patients with Addison's disease are at risk for unrecognized and potentially severe nocturnal hypoglycemia also because of a disturbed counterregulatory function. Use of a continuous glucose monitoring system (CGMS) could help to adjust hydrocortisone treatment and to avoid nocturnal hypoglycemia in these patients.
Methods:
Thirteen patients with Addison's disease were screened for hypoglycemia wearing a CGMS for 3–5 days.
Results:
In one patient we identified a hypoglycemic episode at 3:45 a.m. with a blood glucose level of 46 mg/dL, clearly beneath the 95% tolerance interval of minimal glucose levels between 2 and 4 a.m. (53.84 mg/dL). After the hydrocortisone replacement scheme was changed, the minimum blood glucose level between 2 and 4 a.m. normalized to 87 mg/dL.
Conclusions:
Continuous glucose monitoring can detect nocturnal hypoglycemia in patients with primary adrenal insufficiency and hence prevent in these patients an impaired quality of life and even serious adverse effects.
Background
Common glucocorticoid replacement is oral hydrocortisone split into two to three daily doses, with the highest dose administered in the morning. 3,4 Whereas cortisol in healthy individuals rises abruptly in the early morning between 3 and 6 a.m., this physiological biorhythm cannot be achieved with the oral glucocorticoids currently available.
Due to the physiological biorhythm of other hormones involved in glucose metabolism—growth hormone in particular—insulin sensitivity is normally highest in the early morning hours between 2 and 4 a.m. Patients with diabetes receiving insulin treatment are at risk particularly for nocturnal hypoglycemia at exactly that time.
Patients with adrenal insufficiency receiving common oral treatment with hydrocortisone experience unphysiological low cortisol levels in this susceptible period of time. Therefore these patients are at risk for nocturnal hypoglycemia. Potentially, hypoglycemia episodes are more severe and of higher risk in patients with Addison's disease because of the deficient counterregulatory excretion of cortisol. Symptoms of hypoglycemia can be lessened, and so hypoglycemia unawareness can be a problem in these patients.
Continuous glucose monitoring systems (CGMSs) are improved instruments of blood glucose control developed for patients with insulin-dependent diabetes mellitus with often-unrecognized hypoglycemia episodes. 5 –8
In patients with Addison's disease, a CGMS could aid to adjust hydrocortisone treatment and to avoid—potentially severe—nocturnal hypoglycemia.
Patients and Methods
Thirteen patients with Addison's disease (diagnosed as spontaneous primary adrenal insufficiency by low basal cortisol and after tetracosactide [Synacthen®, Novartis, Bagsvaerd, Denmark] stimulation as well as elevated aderenocorticotropin level) from our outpatient clinic were recruited for this study during routine clinical visits or by written information between October 2008 and April 2011. All patients living in the nearer catchment area of our hospital were invited to take part. Diagnosis of diabetes mellitus type 1 or type 2 and known impaired glucose tolerance were exclusion criteria. There were five male and eight female subjects. The mean age of the patients was 46 years (range, 21–71 years). The patients had a mean duration of Addison's disease of 13 years (range, 0.25–52 years).
The subjects were screened for hypoglycemia wearing a CGMS for 3–5 days. The system used was the Minimed® (Medtronic, Northridge, CA) subcutaneous CGMS® System Gold™. This system continuously measures subcutaneous tissue interstitial glucose levels, recording values on average every 5 min within a range of 40–400 mg/dL. It allows 288 measurements of glucose in a 24-h period. A monitor collects and stores the glucose data until they are downloaded into the com-station, where glucose values are displayed.
Sensors were applied by a certified diabetes nurse in our outpatient clinic. Patients were educated in using the sensor and calibration with blood glucose self-measurements three to four times per day. Calibration of the sensor was performed according to the protocol established. At the completion of the measuring period, the system was returned, and the data were downloaded to determine glucose patterns.
Normal distribution of minimum blood glucose values between 2 and 4 a.m. was proved by the Kolmogoroff–Smirnoff test, and the 95% parametric tolerance interval was determined.
Results
In one of the 13 patients we identified an hypoglycemia episode, defined by a blood glucose level of ≤50 mg/dL. The affected patient was a 42-year-old man with a history of Addison's disease for 33 years. Hypoglycemia was recorded at 3:45 a.m. with a blood glucose level of 46 mg/dL (Fig. 1). This value clearly falls below the lower limit of 95% tolerance interval of minimal glucose levels between 2 and 4 a.m. in the other patients, which was 53.84 mg/dL. The patient had been reported to wake up frequently at night for several months, but he had no typical signs of hypoglycemia. After his hydrocortisone replacement scheme was changed—he delayed the last hydrocortisone dose to the late evening—a second CGMS measurement was performed. No hypoglycemia was recorded, the minimum blood glucose level between 2 and 4 a.m. normalized to 87 mg/dL, and the patient has been observed to sleep better since that time.
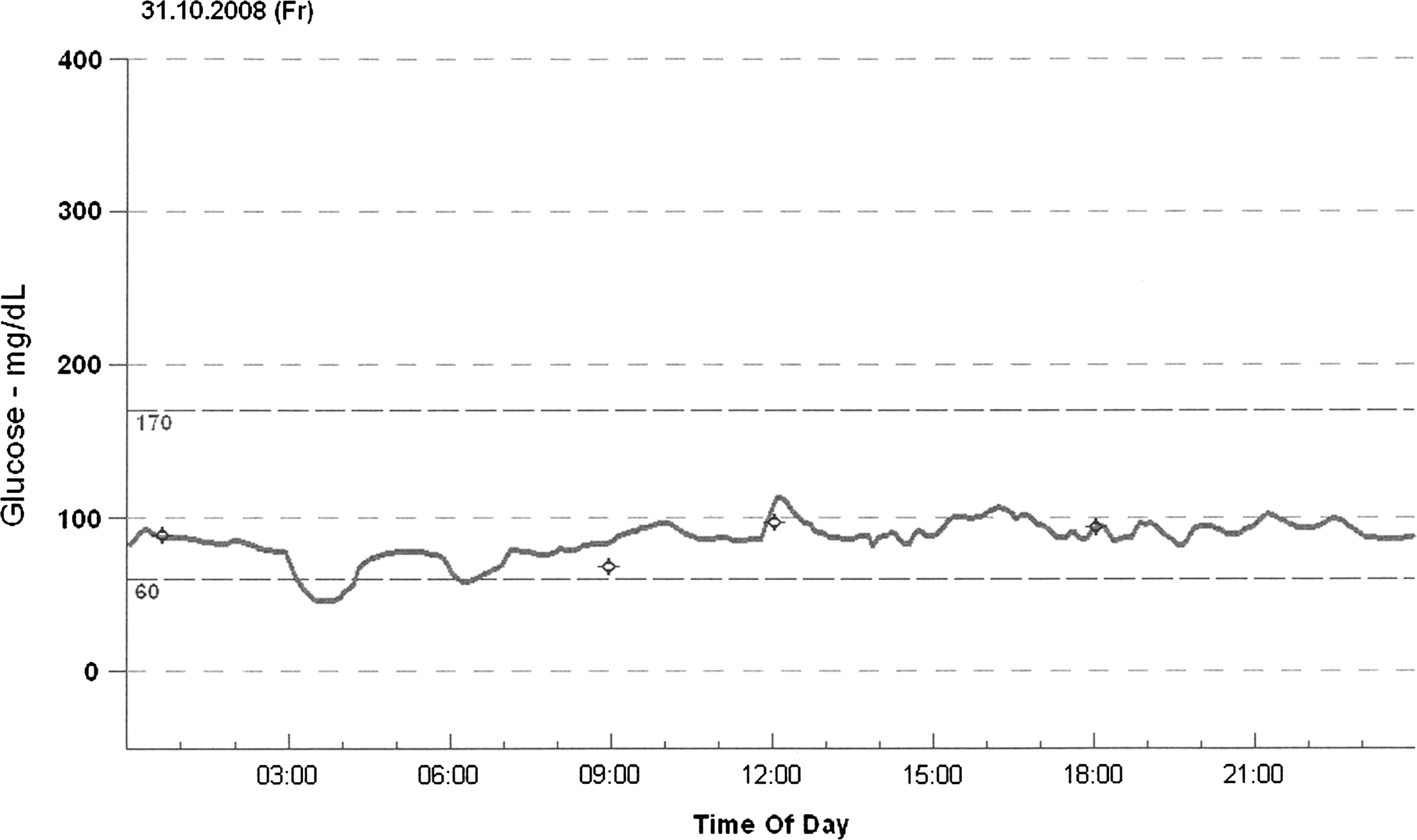
Course of blood glucose levels in one patient with nocturnal hypoglycemia.
With regard to the whole measuring period, this patient showed lower glucose levels with a mean glucose level of 85 mg/dL compared with 99±12 mg/dL in the other patients and more (seven vs. one) and longer (9% vs. 0.5% of the measuring period) episodes with rather low glucose levels <70 mg/dL (Table 1).
Conclusions
Despite the substitution with synthetic gluco- and mineralocorticoids, premature mortality is still documented in Addison's disease. 9,10 The absence of any valid laboratory parameter to assess adequate substitution effects continues to be one of the biggest challenges in the therapy of adrenal-insufficient patients. 3,11 Herein an important problem is the unphysiological dosing with orally available glucocorticoids, particularly in the early morning hours when patients have a window of low cortisol levels—a fact that can lead to hypoglycemia at this time.
The mean glucose level in our patients with primary adrenal insufficiency was 99±12 mg/dL and therefore without any difference from the mean glucose level that has been seen in healthy controls using a CGMS. 12 So, data of this small study do not allow us to conclude about glucose metabolism in adrenal-insufficient patients who are receiving chronic replacement—either for hypoglycemia episodes due to chronic cortisol deficiency or for hyperglycemia episodes due to chronic overtreatment.
However, in one individual with Addison's disease we could detect nocturnal hypoglycemia using the CGMS. Shifting the last hydrocortisone dose to the late evening normalized nocturnal blood glucose levels and improved his sleep.
Therefore continuous glucose monitoring can detect nocturnal hypoglycemia in patients with primary adrenal insufficiency and hence prevent impaired quality of life and potentially even serious adverse effects.
Further research on larger groups of patients is necessary to evaluate the risk of nocturnal hypoglycemia in primary adrenal insufficiency. New therapeutic approaches have been developed like continuous hydrocortisone infusion with hourly adjustable infusion rate via a subcutaneous pump 13 or retarded hydrocortisone formulations given in the late evening. 14 It will be of interest to learn whether these concepts affect nocturnal blood glucose levels.
Footnotes
Acknowledgments
This research was supported by grants from the EU FP7 (grant number 201167, Euradrenal).
Author Disclosure Statement
The authors have no competitive financial interests to disclose.