
Abstract
Aim:
This study evaluated the incidence and factors responsible for plasmid-mediated extended-spectrum β-lactamase (ESBL) infection among patients with diabetic foot ulcer (DFU).
Subjects and Methods:
A prospective study was conducted on 162 DFU inpatients treated in a multidisciplinary-based diabetes and endocrinology center at Jawaharlal Nehru Medical College of Aligarh Muslim University, Aligarh, India, during the period of December 2008–March 2011. Detailed history and patient's profile, grade of DFU, co-morbidities and complications, laboratory data, and final outcome were collected. Standard methods were used for culture identification, sensitivity testing, and ESBL detection. Polymerase chain reaction for bla genes was performed, and the risk factors for bla gene positivity were determined by univariate analysis with 95% confidence interval.
Results:
In total, 127 (78.3%) Enterobacteriaceae members were isolated. The most common isolate was Escherichia coli (71; 55.9%), followed by Klebsiella sp. (33; 25.9%) and Proteus sp. (13; 10.2%). By phenotypic methods, 67.8% were ESBL producers. In the molecular detection of ESBLs, 81.9% were found to be positive for the bla gene, of which bla CTX–M showed 81.8% positivity, followed by bla TEM (50%) and bla SHV (46.9%). In a univariate analysis, bla gene–positive status was associated with low-density lipoprotein-cholesterol (>100 mg/dL) (P<0.004, odds ratio 13.4, relative risk 8.65) and triglycerides (>200 mg/dL) (P<0.003, odds ratio 6.5, relative risk 4.11).
Conclusion:
ESBL constitutes a major threat to currently available β-lactam therapy, leading to complications in DFUs. Aminoglycosides, cephalosporin, and β-lactam inhibitor drugs would probably be more appropriate empirical agents after establishing the patient's history of previous antibiotic use. The detection of ESBL should be done on a routine basis.
Introduction
Extended-spectrum β-lactamases (ESBLs) capable of degrading the extended-spectrum cephalosporins and monobactams are the most relevant determinants of resistance emerging worldwide in the Enterobacteriaceae. 10 ESBL strains exhibit multidrug resistance, which includes resistance to the aminoglycoside and fluoroquinolone groups, and the therapeutic options associated with these strains are fairly limited. In addition to this, increased morbidity, mortality, and cost of health care are also associated. 11 ESBLs are derived through one or more amino acid substitutions from the parental enzymes TEM-1, TEM-2, and SHV-1, and other enzymes, including CTX-M and PER, have reportedly been detected with increasing frequency in many regions. 10 In India, the choice of empirical antimicrobials is extrapolated from available data for Western countries, which may or may not be appropriate for Indian patients. 8 Because long-term studies from India on ESBL-producing organisms isolated from foot infections in diabetes are scarce, we planned to study the prevalence of plasmid-mediated ESBL-producing strains of Enterobacteriaceae and antimicrobial resistance with regard to bacterial species and specimens isolated from foot infections in a North Indian multidisciplinary tertiary-care hospital.
Materials and Methods
Study design
This was a prospective cohort hospital-based study. In total, 162 diabetes patients who were admitted in the Centre for Diabetes and Endocrinology, Jawaharlal Nehru Medical College Hospital, Aligarh Muslim University, Aligarh, India, and had an ulcer or ulcers in their foot during the period December 2008–March 2011 were included in this study. Infection in patients with a cefotaxime-resistant Enterobacteriaceae member (E. coli and Klebsiella sp.) was selected for the genotypic study. The number of patients included for univariate analysis was 58. Multiple ulcers during one hospitalization were considered as one ulcer episode, and the worst outcome of various ulcers was recorded as the final outcome. All the subjects gave informed consent, and clearance was obtained from the Institutional Ethics Committee.
Clinical examination
A detailed history and physical examination was carried out for every subject. Age, sex, anthropometric measurements (body mass index), duration of diabetes, glycemic control prior to and during the hospital stay, lipid profile, presence of retinopathy, nephropathy (creatinine >1.5 mg/100 mL or presence of micro- or macroalbuminuria), neuropathy (absence of perception of the Semmes–Weinstein monofilament at two of 10 standard plantar sites on either foot), peripheral vascular disease (ischemic symptoms and intermittent claudication of rest pain, with or without absence of pedal pulses or posterior tibial pulses), hypertension, duration, site, and size of ulcer, history of smoking, history of previous amputation, and clinical outcome were noted in every patient. Clinical assessment for signs of infection (swelling, exudates, surrounding cellulitis, odor, tissue necrosis, crepitation, and pyrexia) was done by one researcher classifying the ulcers and determining the presence of clinical signs of infection. Ulcer size was determined by multiplying the longest and the widest diameters and expressed in centimeters squared. The wound was graded and staged at the time of hospitalization according to the University of Texas Wound Classification System as grade 1 (superficial wound, not involving, tendon, capsule, or bone), grade 2 (wound penetrating to tendon or capsule), and grade 3 (wound penetrating bone or joint). Grade 0 patients (pre- or postulcerative site that had healed) were excluded from the study. Diagnosis of extension to the bone was made in the majority of patients by probing with a sterile steel probe. In the absence of sinus tract or an exposed bone, a standard radiograph showing signs of osteomyelitis in the bone was considered definitive, and later on magnetic resonance imaging was done to confirm the osteomyelitis in suspected patients. Amputation was defined as the complete loss in the transverse anatomical plane of any part of the lower limb. 9
Microbiological methods
Culture specimens were obtained at the time of admission, after the surface of the wound had been washed vigorously by normal saline, followed by debridement of superficial exudates. Specimens were then obtained by scraping the base of the ulcer or the deep portion of the wound edge with a sterile curette after cleaning the base of the ulcer with a sterile swab stick. 5,6 The specimens were promptly sent to the Microbiology Department and processed for aerobic and anaerobic bacteria. Standard methods for isolation and identification of aerobic 12,13 and anaerobic 14,15 bacteria were used.
Susceptibility testing of aerobic and anaerobic isolates was performed using the disc diffusion method as described by the Clinical and Laboratory Standards Institute. 16 Antimicrobial disk used were imepenem (10 μg), aztreonam (30 μg), amoxyclav (30 μg), cefpodoxime (10 μg), metronidazole (5 μg), ofloxacin (5 μg), cefotaxime (30 μg), cefepime (30 μg), cefixime (5 μg), cefoperazone (75 μg), cefoperazone/sulbactam (75/10 μg), oxacillin (1 μg), piperacillin (100 μg), piperacillin/tazobactum (100/10 μg), ceftazidime (30 μg), ceftazidime/clavulanic acid (30/10 μg), amikacin (30 μg), amoxicillin (20 μg), cefotaxime/clavulanic acid (30/10 μg), ceftriaxone (30 μg), cefoxitin (30 μg), chloramphenicol (30 μg), gentamicin (10 μg), gatifloxacin (5 μg), levofloxacin (5 μg), sparfloxacin (5 μg), streptomycin (10 μg), vancomycin (30 μg), clindamycin (2 μg), tobramycin (10 μg), azithromycin (15 μg), erythromycin (15 μg), and bacitracin (10 units). All discs were obtained from Hi-Media Labs, Mumbai, India. Interpretative criteria for each antimicrobial tested were those recommended by the manufacturer's guidelines.
Phenotypic methods for ESBL detection
Gram-negative bacilli were first screened for the production of ESBL by the disc diffusion method (screening test) using cefotaxime, ceftriaxone, aztreonam, cefepime, cefoxitin, and ceftazidime and later on confirmed by the cephalosporin/clavulanate combination disk (confirmatory test) (disk potential) method using ceftazidime, ceftazidime+clavulanic acid, cefotaxime, cefotaxime+clavulanic acid, piperacillin, cefoperazone+sulbactam, cefoperazone, and piperacillin+tazobactum. 17 E. coli ATCC 25922 (non-ESBL producer) and Klebsiella pneumoniae 700603 (ESBL producer) were used as control strains, respectively.
Molecular methods for β-lactamase detection
Preparation of DNA template
Template DNA was prepared from freshly cultured bacterial isolates by suspending three to five colonies in 50 μL of molecular-grade water and then heating at 95°C for 5 min and immediately chilling at 4°C. Positive controls harboring bla CTX-M, bla TEM, and bla SHV and the negative control (E. coli ATCC 25922) were processed in the same way for DNA extraction.
Detection of bla genes by polymerase chain reaction
Molecular detection of bla CTX-M, bla TEM, and bla SHV was performed in cefotaxime-resistant E. coli and Klebsiella sp. isolates by using polymerase chain reaction (PCR) according to methods described previously with minor modifications. 18,19 The primers and cycling conditions for detection of bla genes were the same as those described by Shahid et al. 19
Antibiotic treatment
Initially, the antibiotic regimen was selected according to published recommendations. 9 The treatment was modified in accordance with the culture results. The duration of the treatment was at least 4–6 weeks and was prolonged in cases of osteomyelitis. All patients also received an intensive insulin treatment.
Statistical analysis
Cefotaxime-resistant patients were divided into two groups: bla gene positive and bla gene negative. Quantitative variables were expressed as mean±SD values. The odds ratio (OR) (strength of association) and risk ratio (RR) (probability of association) with 95% confidence interval were reported for independent variables associated with the outcome variables of bla gene positive and negative. All analyses were performed using SPSS version 19.0 software (SPSS, Inc., Chicago, IL). A P value of <0.05 were considered significant.
Results
Men were predominant (105 patients, 64.8%) in the study subjects compared with women (57 patients, 35.1%) (Table 1). All patients had ulcers graded 1–3 in the University of Texas Wound Classification System. Type 2 diabetes mellitus occurred in 134 (82.7%) patients, whereas only 28 (17.2%) had type 1 diabetes mellitus. The mean age of the subjects was 51.1±11.4 years. The mean duration of diabetes was 13.5±4.6 years, and nearly 111 (68.5%) had had the condition for ≤10 years. Eighty-two patients (50.6%) had neuropathy, 72 (54.4%) nephropathy, 82 (50.6%) retinopathy, and 92 (56.7%) hypertension. Osteomyelitis was present in 20 (12.3%) subjects. Nearly one-third (60 patients, 37%) had had the ulcer for >1 month before presentation at the hospital. The bacterial infection in the ulcer was superficial in 48 (29.6%) cases, subcutaneous in 94 (58%), and osteomyelitic in 20 (12.3%). Glycemic control was poor in 123 patients (69.7%) during the first 5 days of the hospital stay. The majority of the subjects (147, 90.7%) had poor glycemic control (glycated hemoglobin >7%) at the time of hospital admission. Sixty-three (38.8%) received surgical treatment, mainly in the form of debridement. Forty-six (28.4%) patients were subject to amputation, and 18 (11.1%) died during the hospital stay (mean hospital stay, 22.9±15.5 days). Most ulcers were found on interdigits (43.2%), followed by the plantar surface (28.4%), heel (29.5%), margins (12.6%), malleoli (16.7%), and leg (3.6%) and on multiple areas (two or more sites) (31.4%). The size of the ulcer being ≤4 cm2 was observed in 38 (23.4%) patients, compared with >4 cm2 in 124 (76.5%), of which the majority of the patients were males. Grade 1 ulcer was found in 48 (29.6%), Grade 2 in 94 (58%), and Grade 3 in 20 (12.3%) patients.
Data are mean±SD values or n (%) unless otherwise indicated.
CI, confidence interval; Hb, hemogloblin; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; OR, odds ratio; RR, relative risk; SGOT/AST, serum glutamic oxaloacetic transaminase/aspartate transaminase; SGPT/AST, serum glutamate-pyruvate transaminase/aspartate transaminase; WBC, white blood cells.
Microbiological observations
In total, 272 (aerobic+anaerobic) bacteria were isolated, averaging 1.67 (1.57 aerobic, 0.10 anaerobic) species per patient. Thirty-five percent patients had monomicrobial infection, whereas polymicrobial etiology was observed in 65%.
Gram-positive cocci made up 34.5% of infections, compared with Gram-negative bacilli in 65.4%; the Gram-positive to Gram-negative ratio was 1:1.8. The frequency of bacterial isolates from DFUs is shown in Table 2. E. coli was the most common isolate, accounting for 27.8%, followed by S. aureus (23.5%), Pseudomonas aeruginosa (15.6%), Klebsiella oxytoca (7%), K. pneumoniae (5.8%), Proteus vulgaris and Enterococcus faecalis (3.5% each), Acinetobacter sp. (3.1%), coryneform sp. (2.7%), β-hemolytic Streptococcus spp. and coagulase-negative staphylococcal spp. (2.3% each), Proteus mirabilis (1.5%), and Morganella morganii (0.7%). Among the anaerobic bacteria isolated, Gram-positive cocci made up 58.8% of infections, Gram-positive bacilli 29.4%, and Gram-negative bacilli for 11.7%. Peptostreptococcus sp. was the most common isolate, accounting for 35.2%, followed by Peptostreptococcus anaerobius (23.5%), Propionibacterium sp. (17.6%), Bacteroides ureolyticus (11.7%), Clostridium perfringens (5.8%), and Eggerthella lenta (5.8%) (Table 2).
Data are number (%).
CONS, coagulase-negative staphylococcal spp.
Antibiotic resistance profile
A higher percentage of antibiotic resistance (67.1%) was shown by coagulase-negative staphylococcal spp., followed by P. aeruginosa (63.7%), P. mirabilis (57.5%), M. morganii (57.5%), E. faecalis (55.2%), Acinetobacter sp. (51.9%), P. vulgaris (50.3%), β-hemolytic Streptococcus (47.6%), E. coli (45.9%), K. pneumoniae (44.8%), S. aureus (44.3%), K. oxytoca (42.9%), and coryneform sp. (37.1%). All the anaerobes were susceptible to metronidazole, amoxicillin+clavulanate, and imepenem. The detailed antibiotic resistance for each bacterium is summarized in Table 3.
Ps, P. aeruginosa; Ec, E. coli; Pv, P. vulgaris; Pm, P. mirabilis; Mm, M. morganii; Ko, K. oxytoca; Kp, K. pneumoniae; Ac, Acinetobacter sp; Sa, S. aureus; Bhs, β-hemolytic Streptococcus; CONS, coagulase-negative staphylococcal sp.; Cr, Coryneform sp. En, E. faecalis.
NT, not tested.
Phenotypic ESBL detection
On average, 74.2% of Gram-negative DFU isolates were positive in the screening of ESBL by the disc diffusion method: 142 (85.0%) isolates were positive using cefotaxime, followed by 127 (76.0%) for cefpodoxime, 117 (70.0%) for aztreonam, and 116 (69.4%) for ceftriaxone and ceftazidime each. In the confirmatory ESBL test, 67.8% were found to be positive by the disc potential method: 132 (79%) using cefoperazone/cefoperazone+sulbactam, followed by 126 (75.4%) by piperacillin/piperacillin+tazobactum, and 114 (68.2%) by cefotaxime/cefotaxime+clavulanic, whereas ceftazidime/ceftazidime+clavulanic acid showed only 81 (48.5%) produced ESBL (Table 4).
ESBL, extended-spectrum β-lactamase.
Occurrence of bla genes
The frequency of bla genes in DFU isolates is shown in Table 4. Only the E. coli and Klebsiella sp. resistant to cefotaxime were subjected to Class A (CTX-M, TEM, and SHV) ESBL study. On average, 89.3% cefotaxime-resistant isolates were found positive for bla genes, of which CTX-M was found to be the most prevalent ESBL noted in 54 (81.8%), followed by TEM in 33 (50%) isolates and SHV β-lactamases in 31 (46.9%) isolates. Twenty-three (37.2%) strains had all three genes (CTX-M+TEM+SHV), nine (15.2%) strains had CTX-M+SHV, four (6.7%) strains had CTX-M+TEM, two (3.3%) strains had TEM+SHV, 19 (32.2%) strains had CTX-M only, one (1.6%) strain had SHV only, and two (3.3%) strains had TEM only (Fig. 1a, b, and c).
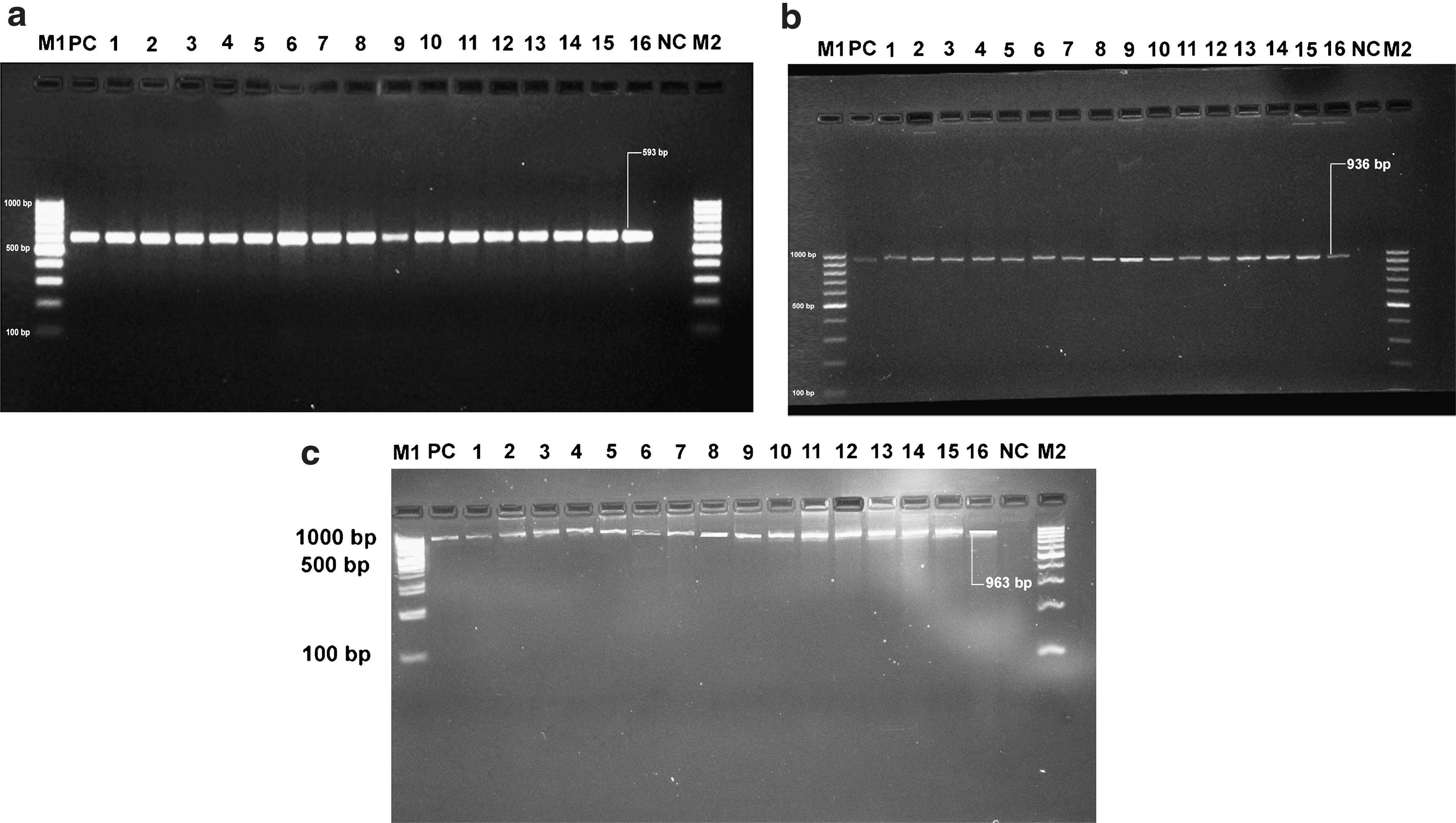
Molecular detection of (
In a univariate analysis (Table 1), OR and RR were calculated between the two groups of patients in which bla tests were performed. The predictive factors that were associated with the bla gene (CTX-M, TEM, and SHV) positivity in cefotaxime-resistant Enterobacteriaceae members (E. coli and Klebsiella sp.) isolated from DFU patients are summarized in Table 1. The significant factors that were more likely to have an association for bla gene positivity were hospital stay (>1 month) (P=0.047, OR 6.9, RR 4.67), low-density lipoprotein-cholesterol (>100 mg/dL) (P<0.004, OR 13.4, RR 8.65), triglycerides (>200 mg/dL) (P<0.003, OR 6.5, RR 4.11), duration of infection >1 month (P=0.58, OR 1.25, RR 1.21), nature of ulcer (necrotic) (P=0.127, OR 5.33, RR 4.54), type 2 diabetes mellitus (P=0.591, OR 2.15, RR 1.92), history of previous antibiotic use (P=0.100, OR 6.75, RR 5.60), smoking history (P=0.618, OR 1.098, RR 1.08), high-density lipoprotein-cholesterol (<40 mg/dL) (P=0.233, OR 3.29, RR 2.80), total cholesterol (>150 mg/dL) (P=0.187, OR 3.52, RR 2.9), and serum glutamate-pyruvic transaminase/aspartate aminotransferase (P=0.04, OR 0.14, RR 0.21).
Discussion
This study presents a comprehensive clinical and microbiological profile of infected DFUs in hospitalized patients with special reference to identifying the factors associated with the risk of bla gene–positive cefotaxime-resistant Enterobacteriaceae members (E. coli and Klebsiella sp.) isolated from DFU patients.
In the present study polymicrobial etiology was found in 65% and monomicrobial in 35% of patients with a rate of isolation of about 1.67 bacteria per patient, which is lower than in previous studies, 6,20 which showed a rate of isolation between 2.3% and 5.8%. The major infective organisms in DFUs in our patients appear to be different. We found Gram-negative aerobic bacteria were most frequently isolated, which is in accordance with our previous report. 3 Studies from Western countries show that Gram-positive aerobes are the predominant organisms isolated from DFU. 21 –25 Zubair et al., 3 in their study on 102 DFU patients, recovered 152 aerobic bacteria, of which 63.8% were Gram-negative and only 36.1% were Gram-positive. Gadepalli et al. 6 also reported Gram-negative aerobes to be the most frequently isolated pathogens (28.7%), followed by 13.8% Gram-positive aerobes. Similar results were also reported by Shankar et al. 26 Studies from Malaysia have also reported a predominance of Gram-negative bacteria (52%) in patients with DFU, with the most common pathogens isolated being Proteus sp., K. pneumoniae, E. coli, and Enterobacter cloacae. 27 The difference in observation in the prevalence of Gram-negative bacilli in DFU between diabetes patients from Eastern and Western countries remains largely unknown. Environmental factors such as sanitary habits (e.g., use of water for perianal wash [ablution] after defecation leading to contamination of hands with fecal flora) are proposed to be responsible for increased the prevalence of Gram-negative organisms in the developing world compared with the West. 8,28 In our anaerobic study, Peptostreptococcus sp. was the most predominant one, which is in accordance with the previous studies. 29,30 We recovered fewer anaerobic species compared with earlier culture reports 31,32 because most of our patients did not have chronic draining wounds, and only 12% had gangrene associated with their infections. This may be an indication of fewer anaerobic species among nonthreatening lower-extremity infections, which was also reported earlier. 33
The overall resistance in our patients was high. It is unclear why the Gram-negative isolates should manifest such high rates of resistance. One reason may include differences in the use of antimicrobial substances, in infection control practices, in different climates, and in other unrecognized factors. 34 Another possible reason could be that most of our patients received some antimicrobial treatment before presenting at our center from the referring hospitals using a combination of different antimicrobials empirically. The Enterobacteriaceae are an important group in community and hospital-acquired infections. The most serious resistance patterns now emerging among Gram-negative organisms include resistance to extended-spectrum cephalosporins and penicillins. 35 This resistance is commonly mediated by ESBLs in E. coli and Klebsiella sp. or by the hyperproduction of chromosomally mediated cephalosporinases (Bush group I ampicillin C enzymes) in Serratia and Citrobacter species. 36 The ESBL genes generally result from point mutations in the genes of broad-spectrum β-lactamase Ambler class A enzymes, such as TEM-1, TEM-2, or SHV-1. They are usually located in conjugative mega-plasmids, which often carry genes responsible for resistance to other antibacterial drugs, making it extremely difficult to treat infections caused by bacteria that produce these enzymes. 37
Along with ESBLs, plasmid-mediated Ambler class C cephalosporinases (or Bush group 1 cephalosporinases) have been found in clinical isolates of the Enterobacteriaceae. These enzymes can produce resistance to cephamycins, extended-spectrum cephalosporins, and aztreonam, and unlike class A ESBLs, β-lactamase inhibitors do not inhibit these bacteria. 38 The resistance pattern in our study was similar to the recent studies done in India and outside. 6,8,26,27 In the present study, Gram-negative bacilli were isolated as ESBL producers in 67.8% of isolates, similar to our previous findings 3 and also in accordance with the reports of Mathur et al. 39 from India. Babypadmini et al. 40 also showed that 40% of K. pneumoniae isolates and 41% of E. coli isolates were ESBL producers in their study cohort. Gadepalli et al. 6 have reported 54.5% of E. coli isolates to be ESBL producers in diabetic foot infections. A study in Brazil reported the prevalence of ESBL as only 6% among E. coli isolates. 41 There is a paucity of data on the prevalence of ESBLs in diabetic foot infection in Gram-negative bacteria other than E. coli and Klebsiella sp. In the screening test, 74.2% of Gram-negative DFU isolates were ESBL-positive, and 67.8% of ESBL producers tested positive with β-lactam inhibitors in a confirmatory test. In a recent study Shobha et al. 42 have reported 27.3% of K. pneumoniae, 25.2% of E. coli, 21.42% of Pseudomonas sp., 25% of Enterobacter sp., and 17% of Acinetobacter sp. to be ESBL producers.
The correct identifications of the genes involved in ESBL-mediated resistance are necessary for the surveillance and epidemiological studies of their transmission in hospitals. In the early study of ESBLs, isoelectric focusing was the better option, but it was time consuming. Recently, several molecular methods have been proposed for the identification of TEM, SHV, and CTX-M derivatives. Multiplex PCR can be used to screen bla CTX-M, bla TEM, and bla SHV. Edelstein et al. 43 detected 15.8% of E. coli and 60.8% of K. pneumoniae isolates as CTX-M ESBL positive, of which 93% were CTX-M-1- and 7% were CTX-M-2-type enzymes. In India, a variant of CTX-M-3 enzyme, designated CTX-M-15, was reported from six unrelated members of the family Enterobacteriaceae. 44 Rodríguez-Baño et al. 45 have reported that 53% of the nosocomial Gram-negative isolates were ESBL producers. In another study, 14 of 39 selected isolates were found to be positive for the bla CTX-M gene by Sekar et al. 46 The prevalence of bla CTX-M was 72 (77.4%) of the 93 E. coli isolates found to be CTX-M group-1 positive by PCR in North Indian isolates. 42 Overall, CTX-M was the commonest genotype (54.3%); 97.2% of them belonged to the CTX-M-1 cluster. On sequence analysis all 20 CTX-M-1 cluster-matched with CTXM-3 subtype. 47
In the present study, occurrence of ESBL in the bacterial isolates was substantiated by bla CTX-M, bla TEM, and bla SHV in DFU using PCR to find out true resistance to antibiotics. The bla gene positivity was 89.3%, of which bla CTX-M positivity was higher (81.8%), followed by bla TEM (50.0%) and bla SHV (46.9%). We also found higher bla CTX-M, bla TEM, and bla SHV positivity in bacteria isolated from DFU patients. The most prevalent ESBL gene was bla CTX-M (81.8%), followed by 50% bla TEM and 46.9% bla SHV, in the cefotaxime-resistant Enterobacteriaceae members (E. coli and Klebsiella sp.) isolated from DFU patients. The genotypic methods helped us to confirm the genes responsible for the production of ESBLs in a single isolate. To the best of our knowledge, no such type of study has been reported from isolates of DFUs; however, bla CTX-M as the most prevalent and widely disseminated gene in the DFU bacterial population has been reported in our previous findings. 3,7
Univariate analysis for the factors that were associated with the bla gene (CTX-M, TEM, and SHV) positivity in cefotaxime-resistant Enterobacteriaceae members (E. coli and Klebsiella sp.) isolated from DFU patients is summarized in Table 1. Duration of infection >1 month, hospital stay (>1 month), nature of ulcer (necrotic), type 2 diabetes mellitus, history of previous antibiotic use, dyslipidemia (low-density lipoprotein-cholesterol [>100 mg/dL], high-density lipoprotein-cholesterol [<40 mg/dL], triglycerides [>200 mg/dL], and total cholesterol [>150 mg/dL]) were independent predictors of bla gene positivity. To the best of our knowledge, no such type of study has been reported from isolates of DFU patients, except our one report on the correlation of CTX-M with the clinical characteristics, in which the positivity of bla CTX-M status was associated with poor glycemic control, osteomyelitis, neuropathy, and previous antibiotic use. 7
Resistance to antibiotics is seen when they are used for a prolonged period of time. This resistance is an acquired form rather than an intrinsic one. The former develops following a mutation in the DNA of a microorganism or by acquisition of a new DNA. Acquisition of new DNA is accomplished by genetic elements such as plasmids or transposons. Resistance plasmids may have approximately 10 resistance genes for various antibiotics. Bacteria can transmit these characteristics to other bacteria. 48 Frequent or unnecessary use of antibiotics result in a selection favoring resistant bacteria. In this study history and discharge summaries showed that an overwhelming majority (12.3%) of the diabetes patients with osteomyelitis who were referred to our center had received antibiotic treatment before. However, which antibiotics and in what doses they were given were not clear; only the duration of the therapy was evident.
Presence of vascular disease characterized by disrupted micro- and macrocirculations causes a delay in wound healing in diabetes patients. 49,50 Disruption of wound healing results from a decreased blood flow into the ulceration and an aberrant expression of growth factors and cytokines as well. These factors, which delay wound healing, cause foot ulcers. Infections of these foot ulcers require a longer duration of treatment with antibiotics and the use of an appropriate antibiotic in an appropriate dosage. 51 In fact, we found that ESBL-positive bacteria were more frequently isolated in our cases. Although this increase was statistically insignificant, we believe that a multicentric study with increased number of cases could positively affect significance. Manual minimum inhibitory concentration determination was not carried out as it was time consuming and tedious for all the ESBL-producing isolates obtained in the present study. The duration of hospital stay may also depend on the management policy of the hospital. In our hospital, patients are discharged once the healing begins and are advised to come to follow-up at the outpatient clinic every week.
Summary
In conclusion, the present study in India, unlike in Western countries, concludes that Gram-negative bacteria dominated in DFU patients, suggesting thereby that all DFU patients admitted to a tertiary-care hospital in India require empirical therapy for Gram-positive as well as Gram-negative organisms. The treatment modes can be modified based on the severity of infection and on the microbiological culture report and current first-day Gram-stained smear finding. There is also a need for periodic antibiotic resistance surveys to help orient physicians and the local population on the best treatment strategies. However, chloramphenicol and carbapenems can be used as a reserve drugs in infections refractory to DFU with conventional drugs. For ESBLs, phenotypic methods are only screening methods for detection in a routine laboratory. The genotypic methods help to confirm the genes responsible for ESBL production. Sometimes multiple genes are responsible for production of ESBLs in a single isolate. Multiplex PCRs for the detection of bla TEM, bla SHV, and bla CTX-M genes in ESBL-producing bacteria provides an efficient, rapid differentiation of ESBLs in selected species of Enterobacteriaceae and can be used as a rapid tool for epidemiological studies among ESBL isolates.
Footnotes
Acknowledgments
We acknowledge Dr. Idrees Mubarak, Senior Resident, Center for Diabetes and Endocrinology, for clinical evaluation of DFU patients. The authors would also like to thank Dr. Rafat Fatima, diabetic educator, for dietary advice and monitoring the patients' diets.
Author Disclosure Statement
Z.M. researched data, wrote the manuscript, and contributed to the discussion. M.A. contributed to the discussion and reviewed/edited the manuscript. J.A. contributed to the discussion and reviewed/edited the manuscript. No competing financial interests exist.