
Abstract
Background:
The hemoglobin A1c (HbA1c) assay is considered the gold standard for assessing glycemic control in children and adolescents with type 1 diabetes mellitus (T1DM). In recent years, point-of-care (POC) testing has been more commonly used in the outpatient clinic. However, despite its popularity, little is known about the accuracy of the POC methods in children.
Patients and Methods:
In this case series, we describe seven children—six with T1DM and one with type 2 diabetes mellitus—who had major discrepancies between measured POC HbA1c via A1cNow+® (Bayer Healthcare Metrika, Sunnyvale, CA) and self-monitored blood glucose records.
Results:
In six subjects, the discrepancy was explained by the presence of the hemoglobin S trait, and an additional subject had the hemoglobin C trait.
Conclusions:
This report demonstrates that as with all laboratory tests, the HbA1c test is subject to limitations, particularly in children with hemoglobin variants. Increased awareness regarding these limitations among healthcare professionals is paramount, especially with the increased use of the HbA1c POC method in the medical community. Failure to recognize these limitations can lead to unnecessary medical, financial, and social interventions that could have profound impact on the patient–doctor relationship.
Introduction
Several methods are available to measure HbA1c. However, in recent years, point-of-care (POC) testing has gained popularity as it has the benefits of providing results within minutes, being less painful because of the small blood volume required, and results in improved patient–clinician communication in children and improved glycemic control in adults. 4 –6 It is well established that laboratory HbA1c testing has its limitations in individuals with conditions that affect erythrocyte turnover and in those with hemoglobin variants, 7,8 but little is known about the accuracy of the POC methods in children with diabetes. We have used the A1cNow+® (Bayer Healthcare Metrika, Sunnyvale, CA) test since 2007 to measure POC HbA1c values in our outpatient pediatric diabetes clinics. Here, we report a case series of seven children (Table 1) with diabetes who had major discrepancies between measured POC HbA1c using the A1cNow+ method and reported SMBG from home blood sugar records, and the clinical implications of such findings are discussed.
Hb, hemoglobin; HbA1c, hemoglobin A1c; HPLC, high-pressure liquid chromatography; NA, not available; POC, point-of-care; SMBG, self-monitored blood glucose.
Case Series
Case 1 is a 13-year-old African-American girl diagnosed with T1DM at 9.1 years. At 12.6 years, her POC HbA1c was 9.9%, and average SMBG was 184 mg/dL. At 13.1 years, her POC HbA1c was 9.7% with an average SMBG of 169 mg/dL. HbA1c by high-pressure liquid chromatography (HPLC) was 7.2%. Hemoglobin electrophoresis revealed the hemoglobin C (Hb C) trait (55.7% hemoglobin A [Hb A] and 44.3% Hb C).
Case 2 is a 15-year-old African-American male diagnosed with T1DM at 12.6 years. At 13.8 years, his POC HbA1c was 9.9%, and average SMBG was 113 mg/dL. His diabetologist recommended close parental supervision of his diabetes care. Three months later, POC HbA1c was 12.1%, and average SMBG was 176 mg/dL. The family was adamant that his blood sugars were truthful. HbA1c by HPLC was obtained, which came back at 8.0%. Hemoglobin electrophoresis revealed sickle trait (56.8% Hb A, 40.4% hemoglobin S [Hb S], and 2.8% Hb A2).
Case 3 is an 11-year-old African-American male diagnosed with T1DM at 14 months. At 10 years, his POC HbA1c was >13%. This prompted a social work evaluation and intervention. One month later, his HbA1c continued to be >13%. However, his home SMBG records revealed an average blood sugar of 230 mg/dL. Falsification of blood sugar records was considered as a possibility. Two months later, his average SMBG was 200 mg/dL with frequent lunchtime hypoglycemia. His POC HbA1c was 12.6%. HbA1c by HPLC was then performed and was 8.4%. Hemoglobin electrophoresis revealed sickle trait (54.4% Hb A, 42.5% Hb S, and 3.1% Hb A2).
Case 4 is a 7-year-old African-American female who was diagnosed with T1DM at age 5 years. Two months after diagnosis, her POC HbA1c was >13% with a reported average SMBG of 181 mg/dL. At 5.75 years of age, POC HbA1c was 11.2% with an average SMBG of 147 mg/dL. HbA1c by HPLC was 8.6%. An atypical hemoglobin was noted on the chromatogram; however, hemoglobin electrophoresis has yet not been performed.
Case 5 is a 15-year-old African-American male who was diagnosed with T1DM at 10 years. At 13.8 years, POC HbA1c was >13% with a reported average blood sugar of 208 mg/dL. At 15 years, his average SMBG was 184 mg/dL, and POC HbA1c was >13%, but his HbA1c by HPLC was 9.2%. When these discrepancies were discussed with the family, they reported that the patient has sickle trait, but they had failed to mention this to the medical team.
Case 6 is a 14.3-year-old African-American female with T1DM since 11 years of age. Six months after diagnosis, her POC HbA1c was 10.2% with an average SMBG of 150 mg/dL. The patient was accused of falsifying her SMBG readings. Three months later, POC HbA1c was 11.3%, but her average SMBG was 169 mg/dL, with significant hypoglycemia at lunch. At the next visit, her POC HbA1c was 10.4% with an average SMBG of 174 mg/dL. HbA1c by HPLC was 7.4%. Hemoglobin electrophoresis revealed sickle trait (54.2% Hb A, 43.4% Hb S, and 2.4% Hb A2) (Fig. 1).
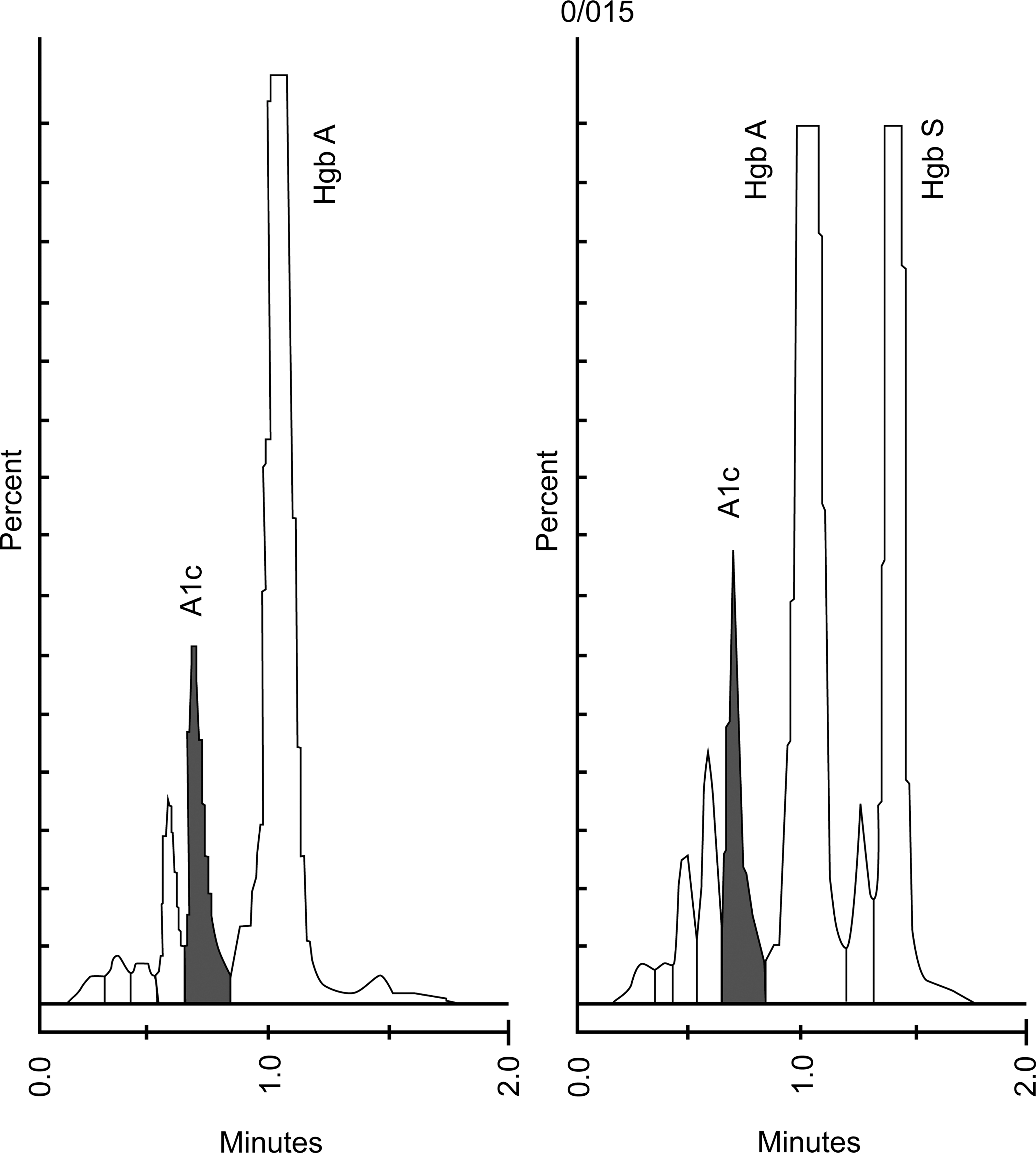
Summary of high-performance liquid chromatography separations of hemoglobins seen in blood.
Case 7 is a 17.6-year-old African-American female with T2DM since 14 years of age. At 17.25 years, POC HbA1c was >13%, but she did not bring any SMBG readings to review. Social work established a contract with expectations. At the next clinic visit, her POC HbA1c was >13% with an average SMBG of 220 mg/dL. She was admitted to the hospital for uncontrolled diabetes. HbA1c by HPLC was 9.3%. Hemoglobin electrophoresis revealed sickle trait (55.3% Hb A, 42.5% Hb S, and 2.1% Hb A2). Upon further discussions, it was learned that the mother knew that her daughter had sickle trait but did not think that it was important.
Discussion
The HbA1c assay has been considered the gold standard for assessing glycemic control in patients with diabetes for decades. 1 However, concerns remain regarding the standardization and accuracy of the various methods used in practice. To date, more than 30 assays are commercially available that measure glycated hemoglobin based on its physical, chemical, or antibody-recognized characteristics. The National Glycohemoglobin Standardization Program was developed in the early 1990s with the goal to standardize these methods based on the reference assay used in the Diabetes Control and Complications Trial. 3,9 However, significant biases between POC and simultaneous clinical laboratory measurements still exist as clearly illustrated by this case series. At our institution, HbA1c measurements with the DCA 2000 (Siemens Diagnostics, Tarrytown, NY) were performed until October 2007. Because of technical support problems and increasing cost, the hospital switched to the Bayer A1cNow+ in October 2007. Prior to implementing the A1cNow+ test in our diabetes clinics, we obtained data to support the reliability and validity of this method. Comparative data for HbA1c among the A1cNow+, the DCA 2000, the hospital's reference system (Tosoh Bioscience, South San Francisco, CA), and a certified National Glycohemoglobin Standardization Program reference laboratory (in Sunnyvale) was obtained for 40 diabetes and control patients without hemoglobinopathies. The correlation coefficient of each method compared with the A1cNow+ was 0.9521 (vs. DCA 2000), 0.9726 (vs. Tosoh), and 0.9653 (vs. the National Glycohemoglobin Standardization Program laboratory), reflecting strong correlation among all four methods. In our series, all seven patients had HbA1c values that correlated well with reported SMBG values prior to switching to the A1cNow+ kit, which indicates that the accuracy of the HbA1c measurement is highly dependent on the assay used.
Six of our patients were noted to have the sickle cell (Hb S) trait, and one had the Hb C trait. Hb S is the most commonly encountered hemoglobin variant in the United States, affecting 7.0% of African-Americans. 10 Hemoglobin electrophoresis is commonly performed as part of the newborn screen, but some patients and families may not be aware of the results or the potential significance. The presence of the Hb S and the Hb C trait has been shown to affect the accuracy of various POC HbA1c assays in three ways. 11,12 First, hemoglobinopathies can alter the normal process of glycation of Hb A to HbA1c. Second, they can cause an abnormal peak on chromatography, making the estimation of HbA1c unreliable. Third, they can make the red blood cells more prone to hemolysis, thereby decreasing the time for glycosylation to occur and producing a falsely low HbA1c result. 13 Thus, depending on which laboratory method used, the HbA1c value in a person with Hb S maybe either falsely high or falsely low. However, studies of the DCA 2000 showed no clinically significant bias with either the Hb S or Hb C trait, 11 which is similar to what we saw in our patient population. Marketed since the late 1990s, the DCA 2000 is one of the oldest available POC instruments, and its results correlate well with the HPLC standard methods. 14 HPLC eliminates the interference from hemoglobin variants and reports a more accurate HbA1c value (Fig. 1). Disadvantages of the DCA 2000 are that the instrument is expensive and time consuming and requires external controls as well as handling by trained personnel. The newer generations of disposable POC instruments, such as the A1cNow+, are small, easy to use, and affordable, making them appealing to primary care and specialist practices. 15 The A1cNow+ has been shown to have good performance in adults 18 years and older, especially in HbA1c ranges between 7% and 8.5%. 16 However, there are no studies evaluating this method in children or in individuals with hemoglobinopathies. Judging from our experience, one can safely assume that the A1cNow+ method performs poorly in children with hemoglobin variants.
Most of the studies available on the accuracy of HbA1c assays (both laboratory and POC assays) included blood samples for standardization purposes. 7,8,11 However, studies on the performance of these methods in clinical practice in children are scarce. After a detailed review of the literature, we identified two case reports describing inaccuracies in HbA1c results due to hemoglobinopathies in children. 17,18 The first report included two children. One was a 12-year-old African-American male with uncontrolled T1DM who had serum blood glucose concentrations consistently above 240 mg/dL. His serum HbA1c performed by ion exchange chromatography was 6.4%. He was later found to have the Hb S trait. The other case was a 17-month-old girl with Shwachman–Diamond's syndrome who had a serum HbA1c of 14.6% by ion exchange chromatography with a fasting blood glucose level of 84 mg/dL. A repeat HbA1c was 2.8% by affinity chromatography, and she was noted to have a high fetal hemoglobin (Hb F) fraction, which is a known finding in this syndrome. An additional article 18 described a 30-month-old male with sickle cell disease (homozygous Hb S) who was noted to have an undetectable HbA1c by HPLC due to elevated Hb F and absence of Hb A. Therefore, our case series reports on a larger number of children with diabetes and hemogobinopathies using a POC HbA1c assay, specifically the A1cNow+ test.
Although this brief report does not present a novel concept, it is of great value for healthcare professionals who deal with children with diabetes for multiple reasons. First, it addresses a common clinical dilemma often encountered by physicians when a discrepancy between clinical impression and laboratory data exists. This often leads to the assumption that the patient or family is not being honest about SMBG results, and the physician is left asking what to do next. In our case series, this discrepancy prompted the medical team to discuss the results with the director of the pathology laboratory at our institution, which led to the described findings. Second, laboratory HbA1c testing has recently been approved for the diagnosis of diabetes 19 in adults. Although there is controversy regarding the use of HbA1c for diagnostic purposes in children, 20 awareness regarding the effects of hemoglobinopathies on the accuracy of the POC assay needs to be increased among primary care physicians in order to avoid the incorrect diagnosis of diabetes or in certain instances missing a case of diabetes.
Conclusions
In summary, the HbA1c test is a valuable tool for assessing glycemic control in children with diabetes. However, as with any laboratory test, it is subject to limitations, particularly in children with hemoglobin variants. Increased awareness regarding these limitations among healthcare professionals is paramount, particularly with the increased use of the HbA1c POC method in the medical community. All of our observed discrepancies occurred with the A1cNow+ test, and we did not investigate other POC methods. Failure to recognize these limitations can lead to unnecessary medical, financial, and social interventions that could have profound impact of the patient–doctor relationship.
Footnotes
Author Disclosure Statement
No competing financial interests exist.