
Abstract
Background:
Gestational diabetes mellitus (GDM) is associated with adverse perinatal outcomes, if not treated. International guidelines recommend screening “all or high-risk women” at the initial prenatal visit, when a fasting plasma glucose (FPG) between 92 and 126 mg/dL is diagnostic for GDM. However, glucose testing may be affected by a great pre-analytical variability (usually overlooked), due to, for example, kind of sample (serum/plasma), temperature of storage, time between blood draw and centrifugation (in-tube glycolysis), and use of a glycolysis inhibitor. So GDM may be easily missed. We aimed to evaluate the potential characteristics of this important issue.
Subjects and Methods:
FPG was tested by both “routine” and “gold standard” protocols in 60 women at the first trimester of gestation, presenting for GDM screening. “Routine” blood plasma was collected in a tube with sodium fluoride, kept at room temperature, centrifuged, and tested 30–45 min after blood draw. “Gold standard” was a specimen from the same blood sample that was centrifuged within 5 min and tested together with the “routine” specimen.
Results:
In the “routine” protocol, 10 mg/dL on average was lost for each determination. Thirteen cases of GDM and two of overt diabetes (FPG >126 mg/dL) were missed in this preliminary series.
Conclusions:
The risk for GDM underdiagnosis in the first half of pregnancy appears to be actual and wide. A closer collaboration between clinicians and pathologists is critical, allowing a stricter adherence to the laboratory guidelines to be ensured.
Introduction
In fact, GDM is a common pathological condition in pregnancy, but, if not treated, maternal hyperglycemia may lead to many adverse perinatal outcomes. The occurrence of GDM is associated with an increased incidence of maternal morbidity (cesarean deliveries, postpartum type 2 diabetes, preeclampsia) and perinatal/neonatal morbidity (macrosomia, birth injury, shoulder dystocia, hypoglycemia, polycythemia, hyperbilirubinemia). 3,4 Long-term sequelae of in utero exposure to hyperglycemia may include a higher risk for obesity and diabetes later on in life. IADPSG guidelines are based on a vigorous assessment of the Hyperglycemia and Adverse Pregnancy Outcome (HAPO) results, the observational epidemiologic study from which the new diagnostic criteria derived, 3 and other studies showing that higher first-trimester fasting glucose levels within what is currently considered a nondiabetes range increase the risk of adverse pregnancy outcomes 4 and the proposal that early detection and treatment may improve pregnancy outcome. 5,6 For these reasons, risk assessment for diabetes should be undertaken at the first prenatal visit, according to the following criteria. The low-risk group is defined as <25 years old, normal body weight, no family history of diabetes, no history of abnormal glucose metabolism, no history of poor obstetric outcome, and not a member of an ethnic/racial group with a high prevalence of diabetes. The high-risk group is defined as those with marked obesity, personal history of GDM, glycosuria, or a strong family history of diabetes. Fasting plasma glucose (FPG) should be measured at the initial prenatal visit in all or high-risk women, on the basis of the background frequency of abnormal glucose metabolism in the population and on local circumstances. An FPG between 5.1 mmol/L (92 mg/dL) and 7.0 mmol/L (126 mg/dL) is diagnostic for GDM (a higher value indicates overt diabetes). More important is that at 24–28 weeks of gestation, all pregnant women should be screened for GDM, using a 2-h 75-g glucose load. A single abnormal glucose concentration at fasting (≥92 mg/dL; 5.1 mmol/L), 1 h (≥180 mg/dL; 10.0 mmol/L), or 2 h (≥153 mg/dL; 8.5 mmol/L) is sufficient for diagnosis and treatment of GDM.
Easily Missed?
GDM is managed not only by different specialists (diabetologist, endocrinologist, gynecologist), but also by primary care physicians, who make the diagnosis thanks to routine laboratory tests. However, these tests should be very accurate in order to avoid delay or missing the diagnosis. At present, this issue is even more important because, according to IADPSG, the diagnosis of GDM can be made at this initial visit with an FPG, with no need for any further confirmation test, and an oral glucose tolerance test (OGTT) should be performed in all women at 24–28 weeks of gestation, regardless of risk factors. In current clinical practice, an FPG is measured in most pregnant women at the initial visit, whereas a universal screening is not yet applied extensively. 7 Moreover, the analytical accuracy required for the diagnosis of GDM may not always be ensured. In fact, as one single test “makes” the diagnosis, its accuracy should be high. Although enzymatic methods are very precise, glucose testing is, however, affected by a great pre-analytical variability, due to kind of sample (serum/plasma), temperature of sample storage, time between blood draw and centrifugation/separation (glycolysis continues in the tube), and presence or not of a glycolysis inhibitor in the tube. Together, these factors may account for up to 20% of total imprecision for FPG around the diagnostic cutoff. 8,9 Because this pre-analytical variability, resulting from a more or less relevant grade of in-tube glycolysis, always causes an underestimation of the actual FPG, the proportion of patients with GDM who could be missed, even in the case of a universal early screening, is at least 7%, as calculated from the HAPO Study. 3 Therefore, GDM can be easily missed, in particular before the 24th week, whenever glucose testing is measured not strictly following laboratory guidelines. 8 Nowadays, in daily routine this is no longer the exception but the rule, particularly in those laboratories receiving a large amount of samples from a large territorial area and particularly for FPG (usually tested on a sample to be used again for other tests, unlike glucose measured in an OGTT). Furthermore, in the first 1–2 h after blood draw, glucose decrease in the tube is virtually the same with or without sodium fluoride (the most widely used glycolysis inhibitor) because it takes time to start working. 10 On this specific issue, perhaps other methods of glycolysis inhibition could be more effective, such as sample refrigeration or acidification. 11
Original Data
Figure 1 gives a clear example of those statements by showing the correlation between “routine” and “gold standard” FPG of 60 women in the first trimester of gestation who were referred to the San Bortolo Hospital Laboratory in Vicenza, Italy by their gynecologists for GDM screening. “Routine” blood plasma was collected in a tube containing sodium fluoride, kept at room temperature, centrifuged, and tested 30–45 min after the blood draw. “Gold standard” was a specimen from the same blood sample that was immediately (within 5 min) centrifuged and separated; then it was tested for FPG together with the “routine” specimen. In this small series, 13 patients with GDM and two with overt diabetes were missed, according to IADPSG guidelines.
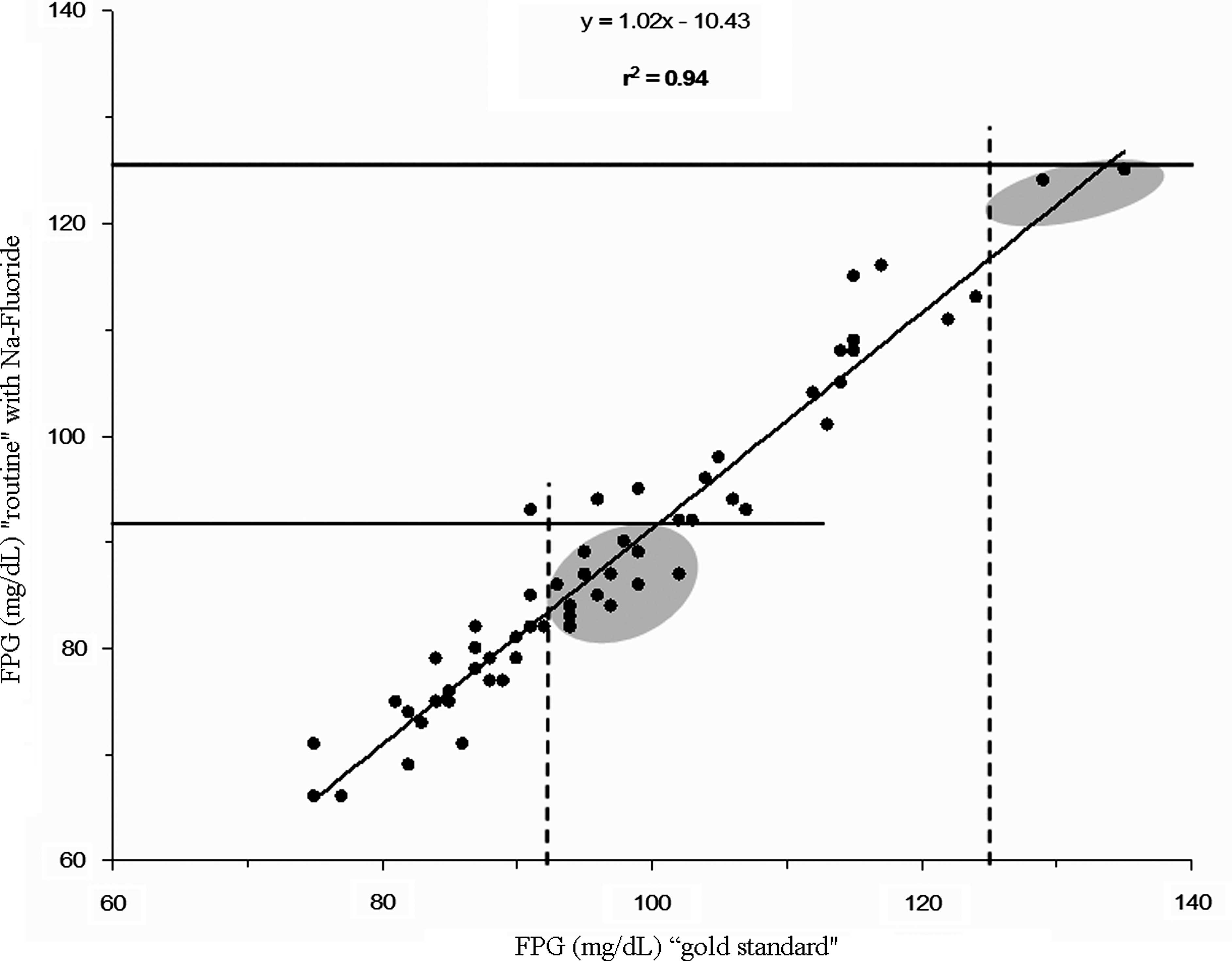
Scatter plot comparing “routine” and “gold standard” for glucose testing: in “routine” specimens 10 mg/dL on average was lost for each determination. Gray areas highlight misdiagnosed cases at the cutoff levels of 92 and 126 mg/dL. FPG, fasting plasma glucose.
Conclusions
The risk for GDM underdiagnosis in the early period of pregnancy is actual and probably greater than is commonly believed. The universal screening for GDM at 24–28 weeks of gestation with an OGTT, as proposed by the scientific community, 2,12 may allow the potential heath risks resulting from the initial misdiagnosis to be minimized. However, methodology makes a difference in glucose testing accuracy; in particular, timing is important for both FPG and OGTT. A closer collaboration between clinicians and pathologists may help to solve the problem: physicians could clearly indicate the condition of pregnancy in the request for FPG, while lab technicians should ensure in this case a strict adherence to the laboratory guidelines.
Footnotes
Author Disclosure Statement
No competing financial interests exist.