
Abstract
Background:
This study aimed to compare glycemic variations seen among Japanese patients with type 1 diabetes treated with insulin glargine versus insulin detemir using continuous glucose monitoring (CGM) in a crossover design.
Subjects and Methods:
Twenty-three patients with type 1 diabetes were enrolled in this study. The subjects were on either insulin glargine followed by insulin detemir twice daily, or vice versa, with no change in the timing of injections. The glycemic variations during 4-day hospitalizations were monitored by CGM while the patients were on either regimen, with a second hospitalization scheduled more than 1 month after the change of the long-acting insulin analogs. CGM data obtained on Day 3 of both hospitalizations were compared.
Results:
The subjects had a median age of 44.0 years, a median body mass index of 22.2 kg/m2, and a median glycosylated hemoglobin of 7.3%. There was no significant difference between the two treatments with a mean glucose level of 156 mg/dL with the insulin glargine treatment versus 150 mg/dL with the insulin detemir treatment; their SD values were 60 versus 51 mg/dL, their mean amplitude of glycemic excursions values were 121 versus 105 mg/dL, and their mean of daily differences values were 45.7 versus 41.4 mg/dL, respectively. In addition, the insulin detemir treatment was associated with a narrower range of postprandial glucose increases after lunch (80 vs. 59 mg/dL; P=0.007).
Conclusions:
A comparison of the long-acting insulin analogs administered twice daily in type 1 diabetes demonstrated that insulin detemir may potentially offer better glycemic control after lunch than insulin glargine.
Background
Some patients with type 1 diabetes exhibit pronounced glycemic fluctuations to such an extent that it is difficult to keep track of their glycemic variations with only self-monitoring of blood glucose performed several times per day. In this regard, continuous glucose monitoring (CGM) appears to represent an extremely useful modality that assists in optimizing insulin therapy based on a firm grasp of the characteristics of such glycemic variability in each patient.
We have previously reported on glycemic variability as assessed by CGM in 12 patients with type 1 diabetes receiving intensive insulin therapy. 7 This study demonstrated that the magnitude of glucose increases and the time to peak glucose value were the greatest after breakfast (when comparing all meals), which suggested that controlling erratic glycemic excursions after breakfast has important implications for insulin management for patients with type 1 diabetes. Additionally, it was shown that the median time in hypoglycemia (<70 mg/dL) during the daytime (8 AM–9 PM) was 46.5 min (interquartile range, 0–101.3 min), compared with that during the nighttime (9 PM–8 AM), which was significantly longer at 73.0 min (interquartile range, 10.0–242.3 min). Therefore, marked glucose increases observed from dawn through the post-breakfast period may be accounted for by the “dawn phenomenon” or the “Somogyi effect” associated with asymptomatic hypoglycemia during the nighttime.
Insulin analogs, altered forms of human insulin in which the amino acid side chains have been chemically modified, include rapid-acting insulin analogs intended to replace bolus insulin and long-acting insulin analogs intended to replace basal insulin.
As a basal replacement, the use of long-acting insulin analogs is expected to offer more stable glycemic control than intermediate-acting insulin preparation. 8 However, consistent glucose lowering over a 24-h period cannot be ensured even with long-acting insulin analogs, with peaks noted for their glucose-lowering potency. 9 In basal-bolus insulin therapy intended for type 1 diabetes patients with endogenous insulin depletion, therefore, the use of twice-daily subcutaneous long-acting insulin analog injections is recommended to provide a flatter basal insulin profile. 10 In recent years, two kinds of long-acting insulin analog preparations have been used for treatment; however, there have been no reports comparing the effect of these long-acting insulin analogs on glycemic variability when used in a twice-daily regimen in type 1 diabetes patients.
Therefore, in this study, we compared glycemic variations in type 1 diabetes patients receiving basal-bolus insulin therapy using CGM when they were given twice-daily long-acting insulin analog glargine or detemir as a basal replacement.
Subjects and Methods
The study participants comprised a total of 23 patients with type 1 diabetes 20 to less than 80 years of age who were receiving basal-bolus insulin therapy. After written informed consent was obtained from all participants, they were randomly assigned to receive twice-daily subcutaneous injections of insulin glargine or insulin detemir, irrespective of their insulin regimens prior to informed consent. When stable glucose levels were obtained in the patients after more than 1 month of treatment with either regimen with the insulin dosage adjusted as required, the patients were hospitalized for 4 days to evaluate their glycemic variations using a CGMS® Gold™ (Medtronic, Inc., Northridge, CA). At discharge, the patients were started on the other insulin preparation (from insulin glargine to insulin detemir, or vice versa) with no change in the number of daily injections or their timings. When stable glucose levels were obtained in these patients after more than 1 month of treatment with the other regimen with the dosage adjusted as required, the patients were hospitalized again for a 4-day period to evaluate their glucose variations using CGM. Insulin aspart or insulin lispro was used as bolus insulin with no change of preparation during the study. The dosage of bolus insulin given before each meal was adjusted to target the 2-h postprandial glucose goal of ≤140 mg/dL, while that of morning/evening basal insulin was adjusted to target the pre-dinner/pre-breakfast glucose goal of≤110 mg/dL. CGM data obtained on Day 3 of their two hospitalizations were subjected to analysis (Fig. 1).
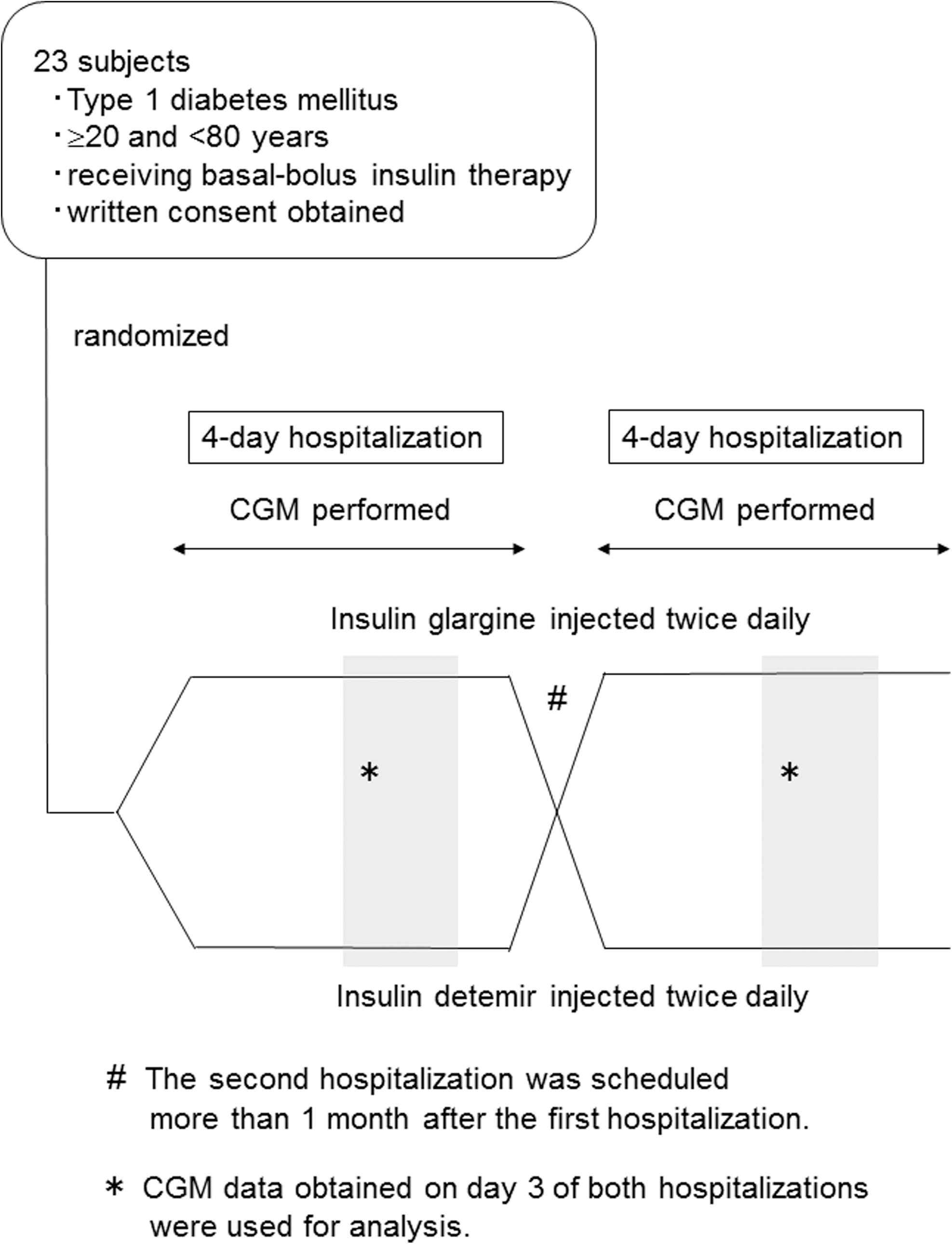
Study design. CGM, continuous glucose monitoring.
During both periods of hospitalization, the study patients were given one of the following hospital diets: (1) 1,440 kcal/day, (2) 1,600 kcal/day, or (3) 1,840 kcal/day, set up according to the criteria of 30–35 kcal/kg (standard weight). The nutritive components of the respective hospital diets on a 1-month average consisted of the following: for breakfast, (1) 435 kcal total calories (50.3% carbohydrates, 14.8% protein, and 35.0% fats), (2) 508 kcal total calories (51.8% carbohydrates, 14.5% protein, and 33.8% fats), or (3) 539 kcal total calories (48.5% carbohydrates, 14.5% protein, and 37.0% fats); for lunch, (1) 491 kcal total calories (61.6% carbohydrates, 19.4% protein, and 19.1% fats), (2) 545 kcal total calories (63.3% carbohydrates, 18.0% protein, and 18.6% fats), or (3) 654 kcal total calories (60.7% carbohydrates, 17.6% protein, and 21.7% fats); and for supper, (1) 513 kcal total calories (62.2% carbohydrates, 19.0% protein, and 18.9% fats), (2) 548 kcal total calories (64.4% carbohydrates, 18.4% protein, and 17.2% fats), or (3) 647 kcal total calories (61.4% carbohydrates, 17.1% protein, and 21.5% fats).
The patients were asked to avoid excessive exercise and snacking. The minimum glucose intake at the time of the symptomatic hypoglycemia was allowed.
A 5–10-min delay occurs with CGMS Gold in the glucose measurement as it involves the use of interstitial fluid, compared with methods involving the use of venous whole blood. It is also reported to be less accurate in glucose measurement during hypoglycemia. 11 However, the interstitial glucose values obtained with CGMS Gold were adjusted for self-monitoring of blood glucose values measured more than four times daily; therefore, these values indicated by CGMS Gold were nearly equal to the venous values. 12
Parameters evaluated included 24-h mean glucose levels, 24-h area under the glucose curve (AUC), SD values of 24-h glucose levels, M-values, mean amplitude of glycemic excursions (MAGE) values, mean of daily difference (MODD) values between Day 2 data and Day 3 data, time in hypoglycemia (<70 mg/dL) during a 24-h period, time in hyperglycemia (>200 mg/dL) during a 24-h period, range of glucose increase, and time to peak glucose levels after each meal, all of which were compared between those receiving insulin glargine treatment and those receiving insulin detemir treatment by using the Wilcoxon signed-rank test. All statistical analyses were performed by using SPSS version 17.0 (
The present study was conducted with the approval of the Institutional Review Board at the Jikei University School of Medicine.
Results
The study participants comprised a total of 23 patients (seven males, 16 females). Patient baseline data were as follows (all values are shown as medians followed by the interquartile range): age, 44.0 (35.0–59.0) years; duration of disease, 20.0 (11.5–34.5) years; glycosylated hemoglobin (HbA1c) (National Glycohemoglobin Standardization Program), 7.3% (7.0–8.4%); urinary C-reactive protein, 1.1 (0.7–3.2) μg/day; and body mass index, 22.2 (19.8–23.4) kg/m2.
The insulin units used for insulin glargine and insulin detemir were shown to be similar at five time points when they were given (Table 1).
Data are median (interquartile range) values.
By Wilcoxon signed-rank test.
Although there was no significant difference among the patients when given either insulin preparation with regard to 24-h mean glucose levels (insulin glargine treatment vs. insulin detemir treatment, 156 [132–186] vs. 150 [127–182] mg/dL; P=0.871) and AUC (224,740 [190,120–267,330] vs. 215,600 [183,475–262,030] mg/dL·min; P=0.903), the insulin detemir treatment was associated with lower median values for these parameters than the insulin glargine treatment (Table 2).
Data are median (interquartile range) values.
By Wilcoxon signed-rank test.
Again, although there was no significant difference among the patients when given either insulin preparation with regard to the indices for glycemic variability—SD of 24-h glucose levels (insulin glargine treatment vs. insulin detemir treatment, 60 [46–75] vs. 51 [39–64] mg/dL; P=0.280), M-values (38 [29–70] vs. 38 [19–67]; P=0.456), MAGE (121 [94–136] vs. 105 [76–129] mg/dL; P=0.140), and MODD (45.7 [37.2–64.3] vs. 41.4 [33.4–59.2] mg/dL; P=0.135)—the insulin detemir treatment was associated with lower median values for SD, MAGE, and MODD (Table 2).
No significant difference was seen among the patients when given either insulin preparation in time in hypoglycemia (<70 mg/dL) or time in hyperglycemia (>200 mg/dL) (Table 2).
With regard to the range of glucose increase from pre-meal levels to postprandial peak levels, however, the insulin detemir treatment was associated with a significantly narrower range of glucose increase after lunch than the insulin glargine treatment (insulin glargine treatment vs. insulin detemir treatment, 80 [45–139] vs. 59 [13–85] mg/dL; P=0.007), whereas there was no difference between the insulin glargine treatment and the insulin detemir treatment in the range of glucose increase after breakfast and dinner. Additionally, there was no difference among the patients given either insulin preparation in time to peak glucose levels after each meal (Table 2).
Indeed, the median glucose levels (interquartile range) in the 23 patients plotted every 5 min (Fig. 2) show that after lunch the insulin detemir treatment was associated with better glycemic control than the insulin glargine treatment. Figure 3 shows the 24-h glucose variations in two divided groups of patients with a median HbA1c≥7.3% and those with less than the median HbA1c under each of the insulin glargine and insulin detemir treatments. This illustrates that postprandial glycemic control is better after lunch in the patients with lower HbA1c levels than in those with higher HbA1c levels under treatment of either insulin preparation.
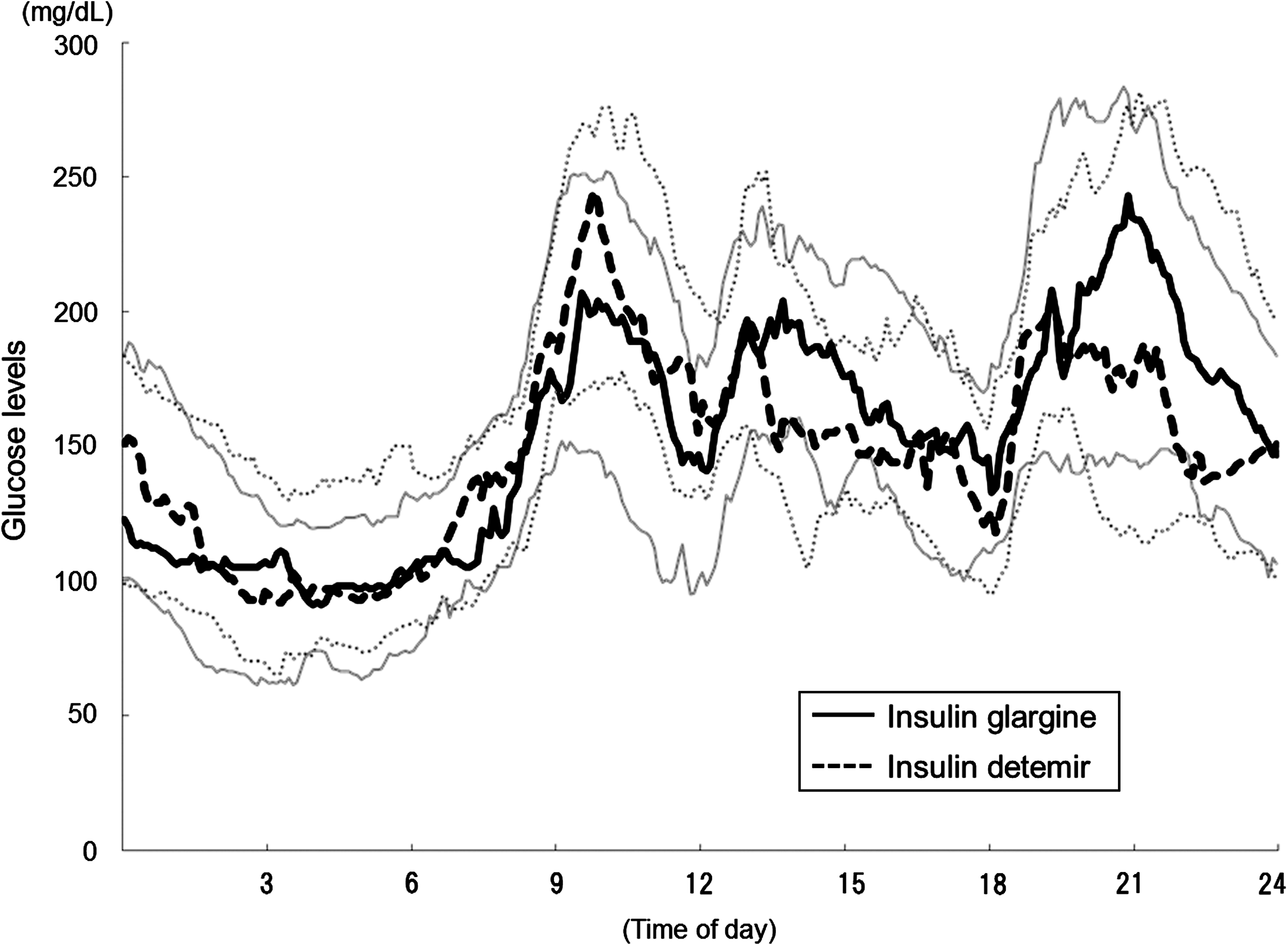
The 24-h glucose variations in patients receiving insulin glargine and insulin detemir (n=23). Curves are expressed as medians (dark lines) and interquartile quartile ranges (gray lines).
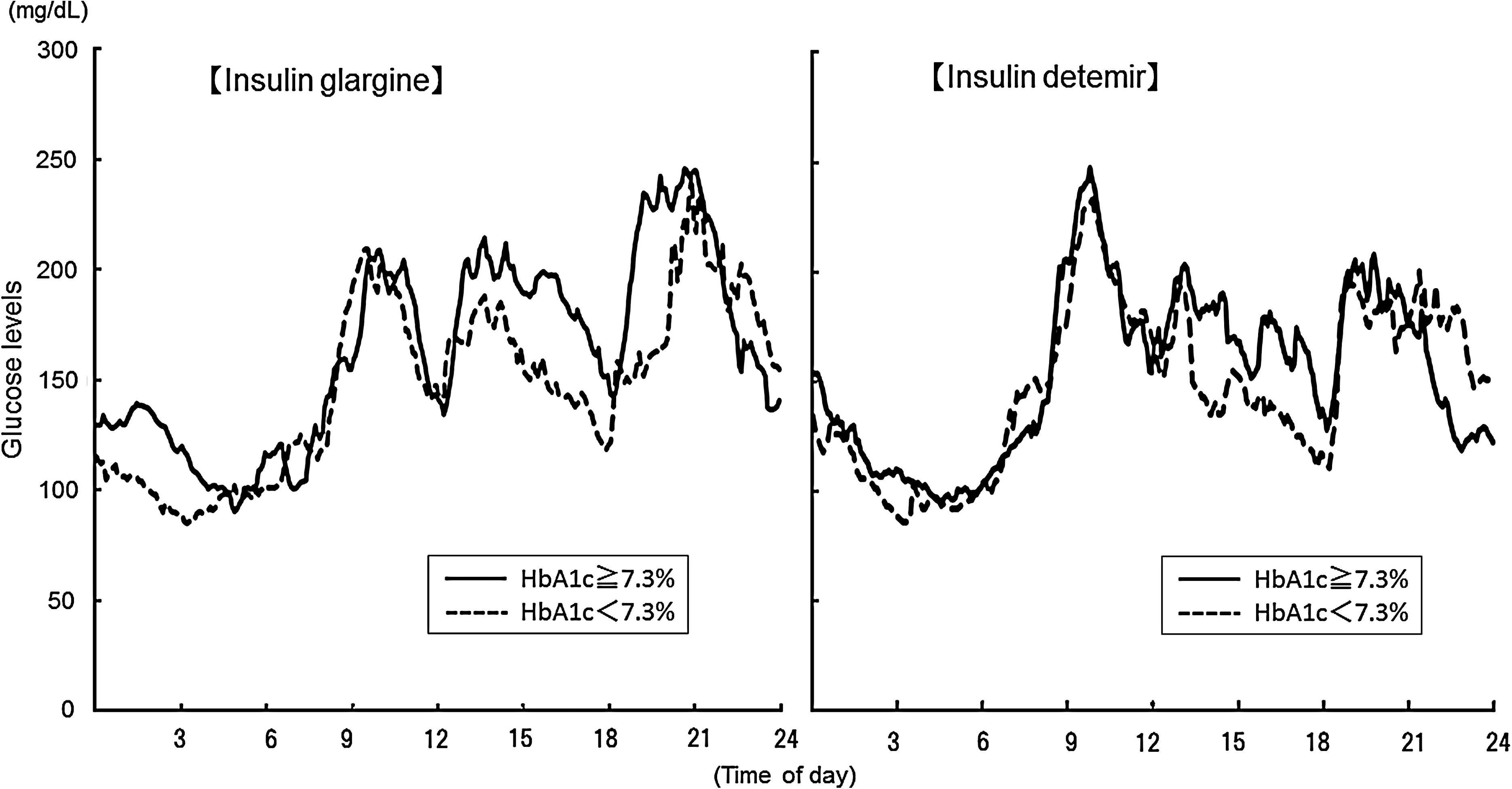
The 24-h glucose variations in two divided groups of patients with a median glycosylated hemoglobin (HbA1c) of≥7.3% and those with less than the median HbA1c under each of the insulin glargine and insulin detemir treatments. Curves are expressed as medians.
With regard to changes in body weight between the two hospitalizations, those who crossed over to insulin detemir tended to be associated with a greater weight decrease than those who crossed over to insulin glargine, although this difference failed to reach statistical significance (−0.7 kg [−1.5 to 0.2] vs.−0.1 kg [−0.95 to 0.625]; P=0.180).
After completion of the study, when the study participants were asked to choose between insulin glargine and insulin detemir after reviewing their CGM data, 14 out of the 23 patients (60.9%) opted for insulin detemir (binominal test, P=0.405).
Discussion
In this study, patients with type 1 diabetes given insulin glargine and insulin detemir twice daily were compared for glucose variability using CGM. Under either insulin treatment, the basal insulin dosage was greater in the morning than in the evening. As there have been no reports of basal insulin dosages injected twice daily in patients with type 1 diabetes, we will need to conduct a further study regarding the appropriate allocation of basal insulin dosages in the future. There is a report that when insulin glargine was administered to patients with type 1 diabetes once daily, either in the morning or in the evening, the dosage in the morning was inclined to be greater. 13 This is similar to our findings.
Study results demonstrate that the insulin detemir treatment was associated with a significantly narrower range of glucose increase from pre- to postprandial peak levels after lunch than the insulin glargine treatment, suggesting that insulin detemir offers better control of glucose excursions after lunch in type 1 diabetes patients than insulin glargine. Furthermore, the insulin detemir treatment was associated with lower median values for 24-h mean glucose levels, AUC, SD, MAGE, and MODD than the insulin glargine treatment, although this difference failed to reach statistical significance.
A previous glucose clamp study of 24 type 1 diabetes patients given both insulin glargine and insulin detemir once daily showed that glucose lowering with insulin glargine had been maintained in almost all patients 24 h after injection, whereas it had declined with insulin detemir about 12 h after injection. 14 On the other hand, a 4-day glucose clamp study of 54 type 1 diabetes patients randomly allocated to treatment with insulin glargine, insulin detemir, or an intermediate-acting insulin preparation once daily showed that insulin glargine exhibited a widely variable glucose infusion rate from one injection day to another, whereas insulin detemir exhibited a nearly consistent glucose infusion rate on each injection day. 15 In our present study comparing insulin glargine and insulin detemir injected twice daily, the instability of glucose lowering with insulin glargine was highlighted as a failing rather than the shorter duration of glucose lowering with insulin detemir.
A previous report in the literature compared the effect of once-daily basal insulin glargine and insulin detemir injections in a crossover fashion in both Japanese type 1 and type 2 diabetes patients. 16 A comparison of glucose levels measured on self-monitoring of blood glucose 10 times daily demonstrated that insulin glargine was associated with significantly lower glucose levels in type 1 diabetes patients after dinner and at 10 PM compared with insulin detemir. However, no adjustment was made to the basal insulin dosage before and after the crossover, despite the fact that many studies have reported insulin detemir has been shown to require a greater insulin dosage than insulin glargine to provide similar glucose lowering. 17 Thus, the results of this crossover study could have been different if the basal insulin dosage had been adjusted appropriately as in our study. In addition, the use of data obtained 3 days after initiating the crossover treatment may be not reliable compared with those obtained later (more days) after the crossover.
In this study, glycemic variations in type 1 diabetes patients were compared when they were subcutaneously injected twice daily with either of the two long-acting insulin preparations. Study results demonstrate that insulin detemir is superior to insulin glargine in controlling glucose excursions after lunch.
A comparison of once-daily insulin glargine versus insulin degludec (which is expected to become available for clinical use as an ultra-long-acting insulin preparation) in type 1 diabetes patients showed that although there was no difference between those given insulin glargine and those given insulin degludec in HbA1c values after 16 weeks of treatment, those given insulin degludec had a 28% reduction of relative risk for hypoglycemia compared with those given insulin glargine. 18 Given these results, a future CGM-based comparison of insulin degludec versus long-acting insulin analog given twice daily using a similar design to the present study may be warranted to identify and determine optimal insulin regimens for type 1 diabetes patients.
Footnotes
Acknowledgments
This study was funded by Japan Diabetes Foundation. We thank all study participants and Kimie Shida.
Author Disclosure Statement
No competing financial interests exist.