
Abstract
Background:
Continuous subcutaneous insulin infusion (CSII) mimics physiologic insulin release better than multiple daily injection (MDI) therapy and allows for greater flexibility in food intake and physical activity. Given these benefits, it raises the question “Is it required to wait to offer CSII to patients with type 1 diabetes (T1D) only after MDI therapy has failed”? This study sought to determine if starting CSII in patients with T1D within 1 year of diagnosis results in better long-term glycemic control than starting it later.
Methods:
This retrospective observational study was conducted in a tertiary-care medical center. The charts of 488 patients with T1D (273 females) 2.6–39 years old (mean, 19.9±7.7 years) who started CSII in 1998–2008 and used it for at least 1 year were reviewed for background, disease-related, and treatment-related variables. Study end points were glycosylated hemoglobin (HbA1c) level, rate of severe hypoglycemia, and diabetic ketoacidosis events during CSII use. Findings were compared between patients who started CSII within 1 year of diagnosis (Group 1, n=93) or later (Group 2, n=395).
Results:
Compared with Group 2, Group 1 patients were characterized by a significantly younger age at CSII initiation (10.7±5.7 vs. 16.4±7.0 years, P<0.001), more frequent blood glucose monitoring (5.4±1.8 vs. 3.9±1.5 times per day, P<0.001), and shorter total duration of diabetes (4.3±2.1 vs. 11.9±6.4 years, P<0.001) and of CSII therapy (3.6±2.1 vs. 4.7±2.5 years, P<0.001). There were no significant between-group differences in patient gender or ethnicity, indications for initiating CSII, mean HbA1c level, attainment of target HbA1c, or rates of severe hypoglycemia or ketoacidosis events after CSII initiation.
Conclusions:
Starting pump therapy at an early disease stage has no added benefit for glycemic control over time than starting later. The timing of CSII initiation should be tailored to the individual patient by the diabetes care team.
Introduction
Over the past decade, continuous subcutaneous insulin infusion (CSII) has become a standard treatment option for patients with type 1 diabetes (T1D). CSII mimics physiologic insulin release better than multiple daily injection (MDI) therapy and allows for greater flexibility in food intake and physical activity. Given these benefits, it raises the question “Is it required to wait to offer CSII to patients with T1D only after MDI therapy has failed?” Several studies have sought to identify factors that predict glycemic control in patients treated with CSII. 6 –8 However, data on initiating CSII shortly after diabetes diagnosis are still sparse, and no study has comprehensively followed metabolic parameters over the long term in these patients.
Our previous study 9 found that achievement of the target glycosylated hemoglobin (HbA1c) was significantly associated with shorter diabetes duration at pump initiation. Therefore, the aim of the present study was to determine if initiation of CSII during the first year after diagnosis of T1D results in better metabolic control over time than later initiation.
Research Design and Methods
This retrospective observational study included 488 patients (273 females) with T1D attending the Jesse Z. and Lea Shafer Institute of Endocrinology and Diabetes, National Center for Childhood Diabetes, Schneider Children's Medical Center of Israel, Petach Tikva, Israel, a major tertiary-care university hospital. Inclusion criteria were age less than 40 years, initiation of CSII treatment during the period from January 1998 to December 2008, use of CSII for at least 1 year, and follow-up for at least 1 year after CSII initiation. The medical charts were reviewed for background, disease-related, and treatment-related data. The cohort comprised part of the patients that were included in our previous study. 9
The study was approved by the local Institutional Review Board.
End points
Study end points were mean HbA1c value and rates of severe hypoglycemia and diabetic ketoacidosis (DKA) events during use of CSII among patients who started CSII within 1 year of diagnosis (Group 1) and patients who started later (Group 2).
Definitions
Good metabolic control was defined according to the recommendation of the International Society for Pediatric and Adolescent Diabetes: HbA1c<7.5% for patients younger than 19 years and HbA1c<7.0% for patients older than 19 years. 10 The HbA1c targets at the patients' actual age at every year of pump use were used to determine whether patients were in or out of target.
A severe hypoglycemic episode was defined as coma or seizures or need for glucagon injections or intravenous glucose infusion. DKA events were defined as blood pH<7.3 with bicarbonate<15 mEq/L and need for intravenous fluid and insulin infusion. Episode frequency was calculated per patient per year during CSII treatment. Episodes of severe hypoglycemia and DKA are documented in the patient's medical file at each clinic visit and after each hospitalization or referral to the emergency room for these indications.
CSII procedure
At our center, patients at any age are recommended for CSII treatment by the multidisciplinary diabetes team (diabetologist, diabetes nurse, and dietician). The decision to initiate pump therapy is individualized and guided by the recommended indications for CSII therapy. 11 If the patient or parents have a preference for CSII treatment, the issue is discussed with the diabetes team of the individual patient, and if there is no contraindication for it, he or she can start CSII therapy.
Before initiation of CSII, patients and, if younger than 18 years, their parents take part in a 3-day education session conducted by a diabetes nurse educator and a dietician who explain insulin adjustments, carbohydrate counting, and pump operation. During the first month of therapy, patients are asked to check blood glucose levels at least eight times per day: before meals, 2 h after meals, at bedtime, and at 2–3 a.m. Thereafter, the frequency is reduced to six times per day (without a regular night measurement). Insulin basal rates and correction boluses are adjusted as required at each follow-up visit, scheduled every 2–3 months. Patients are instructed to change infusion sets at least every 3 days. The team is available 24 h a day for calls and faxes. The same practitioners care for children, adolescents, and young adults.
The frequency of self-monitoring of blood glucose (SMBG) is measured by counting downloads from the patient's glucose meters. Capillary HbA1c is measured by an automated immunochemical technique (DCA 2000; Bayer Diagnostics Inc., Tarrytown, NY) (reference range, 4.3–5.8%). For the present study, the mean annual HbA1c values were used to calculate the mean HbA1c level for the total diabetes duration treated with CSII. The HbA1c level at diabetes onset was excluded from the calculation.
Statistical analysis
The present study was powered to detect a mean difference of 0.5% in HbA1c between the two groups. Assuming a two-tail analysis, α=0.05, and within-group SD of 1.5, with the proposed sample size of 100 and 250 for the two groups, the study will have power of 80.2% to yield a statistically significant result. This effect was selected as the smallest effect that would be important to detect and would be of clinical significance.
Data were analyzed using BMDP software. 12 Data are expressed as mean±SD values. Pearson's χ 2 test or Fisher's exact test was used as appropriate for analysis of between-group differences in discrete variables; analysis of variance was used for continuous variables with a normal distribution and the Kruskal–Wallis test for variables with a non-Gaussian distribution. Changes in HbA1c over time were compared across age groups using analysis of variance with repeated measures, with Bonferroni's correction for multiple comparisons. Correlations between continuous variables were analyzed with Spearman's test. Stepwise logistic regression analysis was used to define the best predictor for HbA1c targets during therapy. A P value of < 0.05 was considered significant. Odds ratios were used to quantify predictors of metabolic control. The receiver operating characteristics curve was used to represent the sensitivity/specificity corresponding to prediction to achieve the HbA1c target in the years after pump initiation.
Results
Background characteristics
The cohort included 215 male and 273 female patients 2.6–39 years old (mean, 19.9±7.7 years; median, 19.5 years) at the time of data collection. Concomitant illness was documented in 89 patients (18.3%): thyroid disease (n=53, 10.9%), celiac disease (n=31, 6.4%), and eating disorders (n=5, 1%). Other background, disease-related, and treatment-related characteristics of the cohort are presented in Table 1.
Data are mean±SD values. P values refer to comparison between Group 1 and Group 2.
Number of events per patient per year of continuous subcutaneous insulin infusion (CSII) therapy.
In Group 2, data on Tanner pubertal stage were missing for 14 patients at CSII initiation and for 12 patients at the last visit.
BMI SDS, body mass index SD score; DKA, diabetic ketoacidosis; F, female; HbA1c, glycosylated hemoglobin; M, male; NS, not significant; SMBG, self-monitoring of blood glucose.
The insulin injection regimen (three or four injections per day) before CSII consisted of neutral protamine Hagedorn+human regular insulin in 415 patients (85%), neutral protamine Hagedorn+rapid-acting insulin analogs (lispro/aspart) in 49 patients (10%), long-acting analog (glargine/detemir)+rapid-acting insulin analogs (lispro/aspart) in 21 (4.3%), and long-acting analog (glargine/detemir)+human regular insulin in three patients (0.7%).
Figure 1 presents the total number of CSII-treated patients who met the study criteria and the number of patients who initiated CSII during the first year after diagnosis for each of the 11 years of the study.
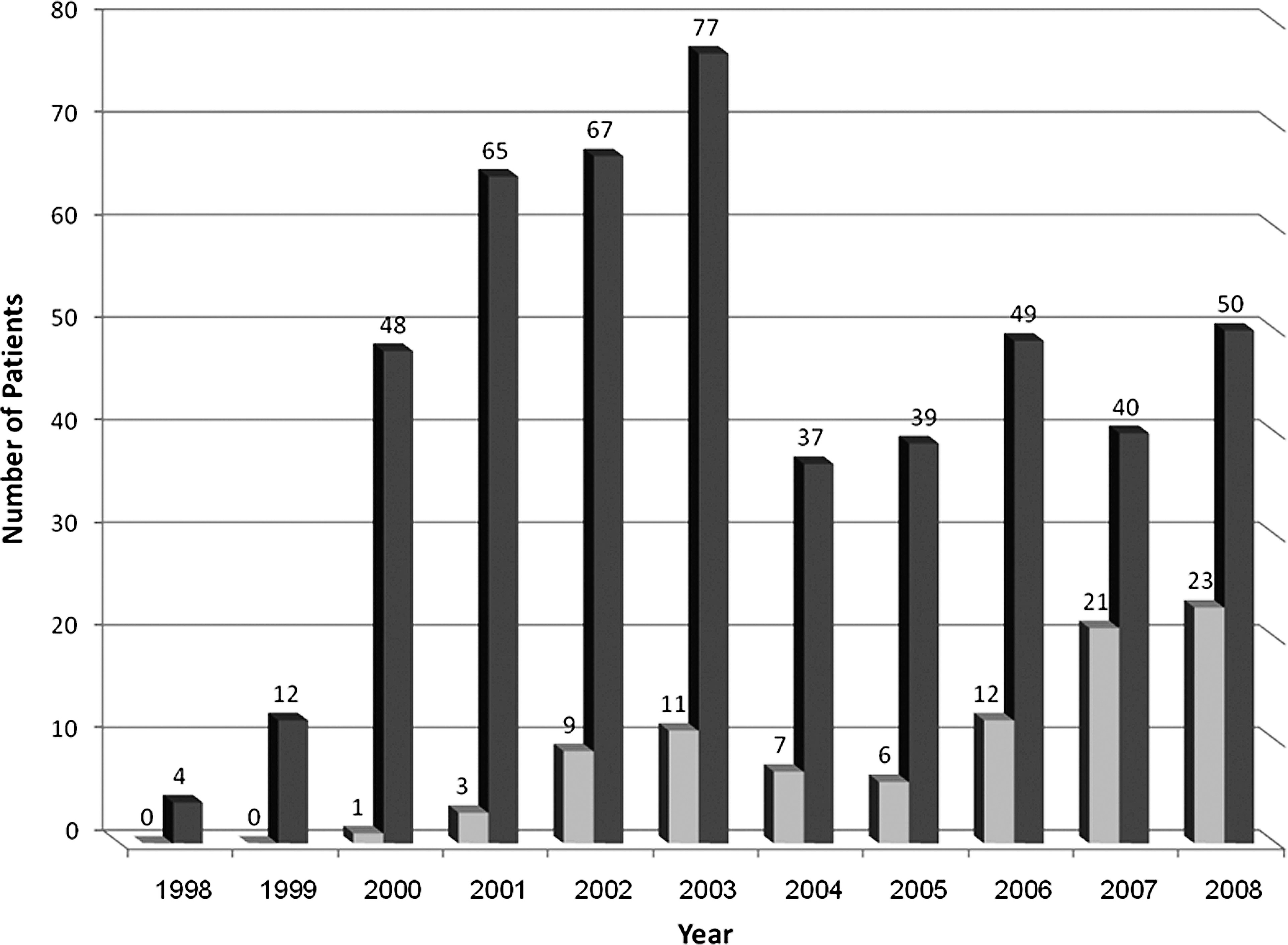
Total number of patients treated with continuous subcutaneous insulin infusion (dark gray columns) and number of patients who started continuous subcutaneous insulin infusion during the first year after diagnosis (light gray columns) in each of the 11 years of the study. The numbers above the columns indicate the number of patients included at each year in each group.
Table 1 describes the comparison of the total group of patients who initiated CSII therapy within 1 year of diagnosis (n=93, Group 1) with those who started after 1 year (n=395, Group 2). Group 1 was significantly younger at initiation of CSII and at the last follow-up visit (P<0.001). In addition, a significantly higher percentage of Group 1 patients was prepubertal at both time points (P<0.001). Specifically, at pump initiation, 20 (21.5%) patients in Group 1 were younger than 6 years (10 younger than 3 years) compared with 21 (5.3%) (three younger than 3 years) in Group 2, and four (4.2%) patients in Group 1 were older than 19 years compared with 117 (29.6%) in Group 2 (P<0.001). The total durations of both diabetes and CSII therapy were significantly shorter in Group 1 than in Group 2 (P<0.001). Group 1 patients also performed significantly more frequent daily SMBG than Group 2 patients at CSII initiation (SMBG frequency more than four times per day, 61.3% vs. 20.2%, P<0.001) and also thereafter (SMBG frequency more than four times per day, 62.8% vs. 48.9%, P=0.03).
There were no significant differences between the groups in gender, ethnic distribution, or the indication for CSII initiation.
Sixty-seven (13.7%) patients discontinued CSII therapy after more than 1 year of pump use, without a significant difference between the groups.
Outcome
The mean HbA1c levels of the study cohort compared with our overall clinic population in the different age subgroups were as follows: in patients younger than 6 years, 8.3±0.8% vs. 7.8±0.9%; in patients 6–10 years old, 7.8±0.7% vs. 8.1±1.2%; in patients 10–19 years old, 8.0±0.9% vs. 7.9±1.3%; and in patients older than 19 years, 7.8±1.1% vs. 7.7±1.2%, respectively.
There were no significant differences between the groups either in HbA1c levels for each year after initiation of CSII or in mean HbA1c level for the entire period of CSII therapy.
Figure 2 shows the longitudinal changes in HbA1c levels of patients in Group 1 (n=29) and in Group 2 (n=181) from initiation of CSII therapy and up to the fourth year of CSII therapy. As seen in both groups there was a slight nonsignificant decrease in HbA1c during the first 2 years of CSII therapy, without a further change.

Longitudinal changes in mean glycosylated hemoglobin (HbA1c) levels in Group 1 (initiation of continuous subcutaneous insulin infusion [CSII] during the first year after diagnosis, n=29; light gray line) and Group 2 (initiation of CSII more than 1 year after diagnosis, n=181; black line) from initiation of CSII therapy and up to the fourth year of CSII therapy. Data are mean±SD values.
For each year after initiation of CSII, the levels of HbA1c in Group 1 were lower than those in Group 2, but not significantly.
Because of the large age variation of our cohort, we have tried to address this limitation by comparing groups by age subgroups and pubertal stage. Although HbA1c levels in Group 1 were lower than those in Group 2, no significant between-group difference in mean HbA1c was found by age subgroups, by pubertal stages, by duration of diabetes, or by duration of pump use (Table 2).
Data are mean±SD values. P values refer to the comparison between Group 1 and Group 2.
Number of events per patient per year of continuous subcutaneous insulin infusion (CSII) therapy.
DKA, diabetic ketoacidosis; HbA1c, glycosylated hemoglobin.
Thirty-one patients in Group 1 (33%) and 114 patients in Group 2 (29%) achieved a mean HbA1c level within the target. This difference was not statistically significant. Further analysis of this parameter by gender also yielded no significant between-group differences.
A significant negative correlation was found between the age of the patients and the daily number of SMBG (r=−0.109, P=0.02) and between the mean daily number of SMBG and the mean HbA1c levels in the total cohort (r=−0.16, P<0.001).
The rates of severe hypoglycemic events or DKA episodes were not significantly different between the two groups, either in total or on subanalysis by age groups or pubertal stages, diabetes duration, or CSII treatment duration (Table 2).
Predictors of glycemic control
The indication for initiating CSII therapy was significantly associated with achievement of good glycemic control. Specifically, the percentage of patients who achieved good glycemic control was higher among those offered CSII because of recurrent hypoglycemic episodes than those offered CSII because of an above-target HbA1c level, with no difference between Group 1 and Group 2. On multiple logistic regression analysis, the factor that most significantly predicted achievement of the HbA1c target was the mean daily number of SMBG with CSII therapy (odds ratio=1.22; 95% confidence interval, 1.09–1.32; P=0.002). The area under the receiver operating characteristics curve for this parameter was 0.62.
Discussion
This study shows that initiation of CSII pump therapy during the first year after onset of T1D is more common among younger patients with newly diagnosed disease. We did not find significant differences in mean HbA1c level between the patients who started CSII therapy within 1 year of diagnosis and those who did so later. This was true for each year after initiation of CSII and for the whole diabetes duration treated with CSII. Additionally, there was no difference between the groups in the rate of patients who achieved the HbA1c target, as defined by the International Society for Pediatric and Adolescent Diabetes, 10 or in the rate of severe hypoglycemia or DKA episodes after pump initiation.
In earlier studies, Pinhas-Hamiel et al. 13 reported that among patients with T1D started on pump therapy, those diagnosed up to 1 year before had significantly lower mean HbA1c levels during the entire follow-up period than those who had had the disease for a longer time. In a comparative study of the effect of starting CSII or MDI at diagnosis in children, de Beaufort et al. 14 found that after 2 months, the CSII group had significantly lower HbA1c levels, but there was no evidence that endogenous insulin production was prolonged. Both Ramchandani et al. 15 and Thrailkill et al. 16 noted that CSII instituted within 1 month of diagnosis of T1D in young patients led to improved metabolic outcome and apparently better preserved β-cell function than MDI. A recently published meta-analysis of 11 randomized clinical trials 17 comparing CSII and MDI in patients with T1D reported that CSII was associated with a significant improvement of HbA1c compared with MDI; the reduction of HbA1c with CSII was evident in trials enrolling patients with mean age older than 10 years, but not in younger children.
Possible reasons for the difference between our results and the HbA1c outcome reported by others 14,15,17 may be differences in the study design (the previous studies compared outcome of CSII with MDI) and in the duration between diabetes onset and initiation of pump therapy (a few weeks in the previous studies as opposed to up to 1 year, with a mean of 0.7 years, in ours). Thus, the influence of CSII therapy on the prolongation of endogenous insulin production might be diminished in patients with disease duration of a few months, especially in the young age group (when the remission period is usually shorter). However, a 63-center analysis of 104 German and Austrian toddlers (<5 years old) with T1D 18 who started CSII therapy within 4 weeks of presentation of diabetes found no significant difference in HbA1c values compared with treatment with MDI. Sulmont et al. 19 observed better HbA1c levels in young patients using CSII from diagnosis than in similar patients who were started on MDI during the following 6 years. However, during the years of CSII therapy the glycemic control was not significantly different between young patients who started CSII at diabetes onset and those switched from MDI to CSII.
In our cohort, the number of patients who started CSII during the first year after diagnosis increased over the last few years of the study, probably as a result of a change in our clinic policy and the health maintenance organization's reimbursement policy over time. Thus, their duration of CSII therapy was shorter.
Imperfect adherence to many aspects of diabetes management has long been recognized as an obstacle to successful intensive treatment, specifically in adolescents. 20,21 The decline in glucose control in adolescents may be attributable to the changing hormonal milieu combined with the opportunity for nonadherence. As demonstrated by the changes in HbA1c levels in our overall clinic at the different age subgroups, it can be seen that after the age of 6 years there is an increase in HbA1c that decreases again after the age of 19 years. It is interesting that in our cohort the group of patients younger than 6 years who initiated CSII earlier had the highest HbA1c, although we have to consider that it was a small group.
We speculated that in the present study, the relatively higher percentage of Group 1 patients in pubertal Tanner stages 2–4, relative to Group 2, at both CSII initiation and the last visit, contributed to the increased HbA1c levels in Group 1, resulting in a nonsignificant between-group difference in glycemic control. However, a comparison of mean HbA1c between the different pubertal stages in both groups failed to yield significant differences as well.
There was a significant correlation between the mean daily number of SMBG and better mean HbA1c level, in agreement with previous reports. 22,23 This factor may represent how well patients are making insulin adjustments in addition to overall adherence to treatment. It is interesting that in our cohort, patients who started CSII therapy during the first year of diabetes routinely performed more frequent SMBG than those who started later. This finding might be attributed to the younger age of patients in Group 1, which we found to be correlated with more frequent daily SMBG. It also may be related to the more frequent boluses given to patients on CSII than on MDI therapy, so they need to monitor glucose more frequently in order to calculate the correction bolus dose. Perhaps the sooner these skills are learned, the better their implementation.
Previous studies have shown that patients who use CSII have a lower incidence of hypoglycemia than patients treated by MDI. 24 –26 One of the major reported benefits of CSII is the lowered rate of severe hypoglycemic events with achievement of good metabolic control, even in young children. 27 This makes CSII an appealing treatment option. In our previous report, 9 CSII therapy significantly reduced the rate of severe hypoglycemia episodes relative to MDI. However, in the present study, there were no significant differences in the rates of severe hypoglycemia or DKA episodes after pump initiation by time of CSII initiation after diagnosis. This finding suggests that CSII is advantageous in itself, regardless of the time at which it is initiated in the course of the disease. Using the present study design, we could not determine if starting CSII early after diagnosis has a better long-term effect on preventing diabetes complications.
The timing of CSII initiation did not have an impact on the daily insulin dose or the body mass index.
It is noteworthy that although insulin replacement by CSII more closely resembles the normal physiology than MDI treatment, starting CSII shortly after diabetes onset can be more time-consuming and stressful for both patient and family. In addition to teaching patients and their families about diabetes, the diabetes team also has to teach them about the pump mechanics and troubleshooting, which requires extra training hours. The patients and families are burdened not only with the need to cope with the new diagnosis but also with the need to learn new skills and techniques.
Nevertheless, it can be argued that starting with MDI may be just as complicated because of the required learning about the differences between insulin duration and how to adjust the insulin dosage to food and exercise requirements.
The strengths of our study are the inclusion of a large cohort of patients of a broad age range (2.6–39 years) from a single tertiary-care center using uniform practice guidelines and the long follow-up of up to 7 years after pump initiation. Furthermore, our cohort reflects a general diabetes clinic population and not only highly motivated patients who are usually enrolled in interventional studies.
Several limitations of our study have to be considered. First, we used a retrospective design with no randomized control group for comparison of the findings by different times of onset of CSII initiation. Second, the results might have been different had we compared patients starting CSII within 3 months from diabetes onset with those starting CSII later, but this subgroup in our center was too small for statistical analysis. Third, we lacked follow-up data on C-peptide levels, which serve as a surrogate marker of β-cell reserve, an important factor in diabetes control. Fourth, we did not evaluate the number of clinic visits that was described to be associated with better glycemic control. However, patients were routinely seen for follow-up visits at our clinic every 2–3 months, without a difference between those who initiated CSII during the first year of diabetes and those who initiated it later. Finally, we lacked data on the number of daily boluses administered in each group, which could also have an impact on glycemic control.
In conclusion, the use of CSII has increased dramatically during the last decade, especially among younger patients. Nevertheless, we found that its implementation during the first year after diagnosis did not lead to better glycemic control over time than with its initiation later in the course of the disease. However, conducting a prospective randomized controlled study with longitudinal follow-up will allow us to draw more firm conclusions about our results. Meanwhile, we suggest that the correct timing of CSII initiation should be tailored for the individual patient by the diabetes care team.
Footnotes
Acknowledgments
The authors wish to thank Pearl Lilos for the statistical data analysis and Gloria Ginzach for the editorial assistance (Rabin Campus, Petach Tikva, Israel).
Author Disclosure Statement
All authors report that they have no competing financial interests.