
Abstract
Background and Aims:
Data on the influence of calibration on accuracy of continuous glucose monitoring (CGM) are scarce. The aim of the present study was to investigate whether the time point of calibration has an influence on sensor accuracy and whether this effect differs according to glycemic level.
Subjects and Methods:
Two CGM sensors were inserted simultaneously in the abdomen on either side of 20 individuals with type 1 diabetes. One sensor was calibrated predominantly using preprandial glucose (calibrationPRE). The other sensor was calibrated predominantly using postprandial glucose (calibrationPOST). At minimum three additional glucose values per day were obtained for analysis of accuracy. Sensor readings were divided into four categories according to the glycemic range of the reference values (low, ≤4 mmol/L; euglycemic, 4.1–7 mmol/L; hyperglycemic I, 7.1–14 mmol/L; and hyperglycemic II, >14 mmol/L).
Results:
The overall mean±SEM absolute relative difference (MARD) between capillary reference values and sensor readings was 18.3±0.8% for calibrationPRE and 21.9±1.2% for calibrationPOST (P<0.001). MARD according to glycemic range was 47.4±6.5% (low), 17.4±1.3% (euglycemic), 15.0±0.8% (hyperglycemic I), and 17.7±1.9% (hyperglycemic II) for calibrationPRE and 67.5±9.5% (low), 24.2±1.8% (euglycemic), 15.5±0.9% (hyperglycemic I), and 15.3±1.9% (hyperglycemic II) for calibrationPOST. In the low and euglycemic ranges MARD was significantly lower in calibrationPRE compared with calibrationPOST (P=0.007 and P<0.001, respectively).
Conclusions:
Sensor calibration predominantly based on preprandial glucose resulted in a significantly higher overall sensor accuracy compared with a predominantly postprandial calibration. The difference was most pronounced in the hypo- and euglycemic reference range, whereas both calibration patterns were comparable in the hyperglycemic range.
Background
These comparably strict calibration guidelines are somehow opposed to the needs of patients with type 1 diabetes, in whom more flexible calibration modes (allowing also for postprandial SMBG) may improve adherence. Although it can be speculated that calibration modes including glucose values measured during less stable phases may deteriorate the precision of CGM, this has not been formally assessed prospectively. The aim of the present study was to investigate whether the pattern of calibration has an influence on sensor accuracy in a clinical routine setting and whether this effect differs according to the glycemic level. Therefore we prospectively compared a predominately preprandial with a predominately postprandial calibration pattern.
Subjects and Methods
Participants
Twenty-six patients (23 male, three female) with type 1 diabetes mellitus were recruited at the outpatient clinic of the University Hospital of Bern, Bern, Switzerland. Inclusion criteria were type 1 diabetes mellitus with a minimal duration of at least 1 year, treated either by continuous subcutaneous insulin infusion or multiple daily insulin injections, and age greater than 18 years. Exclusion criteria were pregnancy, treatment with oral anticoagulants, or hemorrhagic disorders.
Study design
This was a prospective open-label study. Two Guardian-RT CGMS® (Medtronic MiniMed, Northridge, CA) were randomly and simultaneously applied in the lower left and right abdomen of every single individual. The sensors were in use for 3 days and were only included in data analysis if fully functional for at least 24 h. Insulin applications had to be performed with a minimum distance of 5 cm to the CGM sensor for both continuous subcutaneous insulin infusion and multiple daily insulin injections.
Detailed step-by-step instructions on how to use the CGMS were individually given to each participant by a medical doctor experienced in the application of the device and were technically based on the official instruction manual. Two different calibration patterns were applied. In the predominantly preprandial pattern (calibrationPRE) the device was calibrated using the fasting glucose value (before breakfast) and the preprandial value before lunch. Because the CGM system under investigation has a prespecified maximum time window of 12 h between two calibrations, the third calibration time point was chosen in the evening after dinner to avoid calibrations throughout the night. The predominately postprandial calibration pattern (calibrationPOST) encompassed calibrations 2 h after breakfast and 2 h after dinner. In addition, the fasting glucose value of the following day was included to answer the technical requirements. Taken together, calibrationPRE consisted of two pre- and a single postprandial value, whereas calibrationPOST consisted of two postprandial and one single preprandial value. The calibration were performed by SMBG using the subject's own devices to reflect daily clinical routine. At least three additional SMBG values were taken every day. These values as well as the values retrieved for calibration were used as reference values for accuracy analysis.
The study was approved by the local ethical committee, and informed consent was obtained from every individual.
Statistical analysis
Mean absolute relative difference (MARD) (the absolute value of the difference between sensor readings and reference divided by the reference [expressed as a percentage]) was prespecified as the primary outcome. The mean absolute difference (MAD) (the absolute value of the difference between sensor readings and reference [expressed as mmol/L]), correlation coefficients, and the absolute difference between sensor readings and references versus their means 6 were defined as secondary outcomes. To stratify analyses according to glycemic range, sensor readings of each calibration pattern were divided into four categories according to the glycemic range of the reference values (low, ≤4 mmol/L; euglycemic, 4.1–7 mmol/L; hyperglycemic I, 7.1–14 mmol/L; and hyperglycemic II, >14 mmol/L).
Data are expressed as mean±SEM values, unless otherwise specified. Continuous variables were compared using two-tailed t tests. Analysis of variance was applied to compare the four categories within each calibration pattern. Comparison of correlation coefficients was performed using the Fisher r-to-z transformation. A value of P<0.05 was considered statistically significant. To investigate the robustness of the results in a small sample size and to avoid the problems of clustering and oversampling, we performed a sensitivity analysis using a multiple regression model adjusted for the individual. In addition, all subgroup analyses with multiple comparisons were adjusted using post hoc analysis with the Bonferroni correction. All analysis was performed using Microsoft® (Redmond, WA) Excel 2011 and Stata version 10.1 (Stata Corp., College Station, TX).
Results
Initially 26 patients were screened for the study; six had to be excluded (five because of sensor malfunction and one because of a local hematoma). Therefore, in total, 20 individuals were included into the analysis (two female, 18 male). Mean±SEM age was 35.9±2.9 years, mean diabetes duration was 17.4±2.0 years, and mean glycosylated hemoglobin was 7.3±0.25%. Table 1 gives characteristics of the study population.
Totals are mean±SEM values. Duration represents duration of diabetes, therapy represents mode of insulin therapy, and time is the application time of the sensor.
CSII, continuous subcutaneous insulin infusion; F, female; HbA1c, glycosylated hemoglobin; M, male; MDII, multiple daily insulin injections.
The average application time of the CGMS was 65.5±2.43 h (range, 30–73 h). During a total of 1,310 operating hours, 463 reference measurements (SMBG) were obtained. Adherence to the calibration protocol was high: 92.9% of all calibration values were taken within the prespecified time slots. Mean glucose values used for calibration did not differ according to the measurement time point (8.6±0.3 mmol/L for calibrationPRE and 9.2±0.3 mmol/L for calibrationPOST). The overall MARD between reference values and sensor readings was significantly lower for calibrationPRE compared with calibrationPOST (18.3±0.8% vs. 21.9±1.2%, P<0.001). This difference remained significant even if clustering was taken into account (P=0.005 in adjusted multiple regression). The difference resulted from a significantly higher accuracy of calibrationPRE in the low and euglycemic ranges: MARD according to the glycemic range was 47.4±6.5% (low), 17.4±1.3% (euglycemic), 15.0±0.8% (hyperglycemic I), and 17.7±1.9% (hyperglycemic II) for calibrationPRE and 67.5±9.5% (low), 24.2±1.8% (euglycemic), 15.5±0.9% (hyperglycemic I), and 15.3±1.9% (hyperglycemic II) for calibrationPOST (Fig. 1). This translated into a significantly lower MARD using calibrationPRE compared with calibrationPOST in the low (P=0.007) and euglycemic (P<0.001) ranges, whereas no differences were observed in the hyperglycemic ranges.
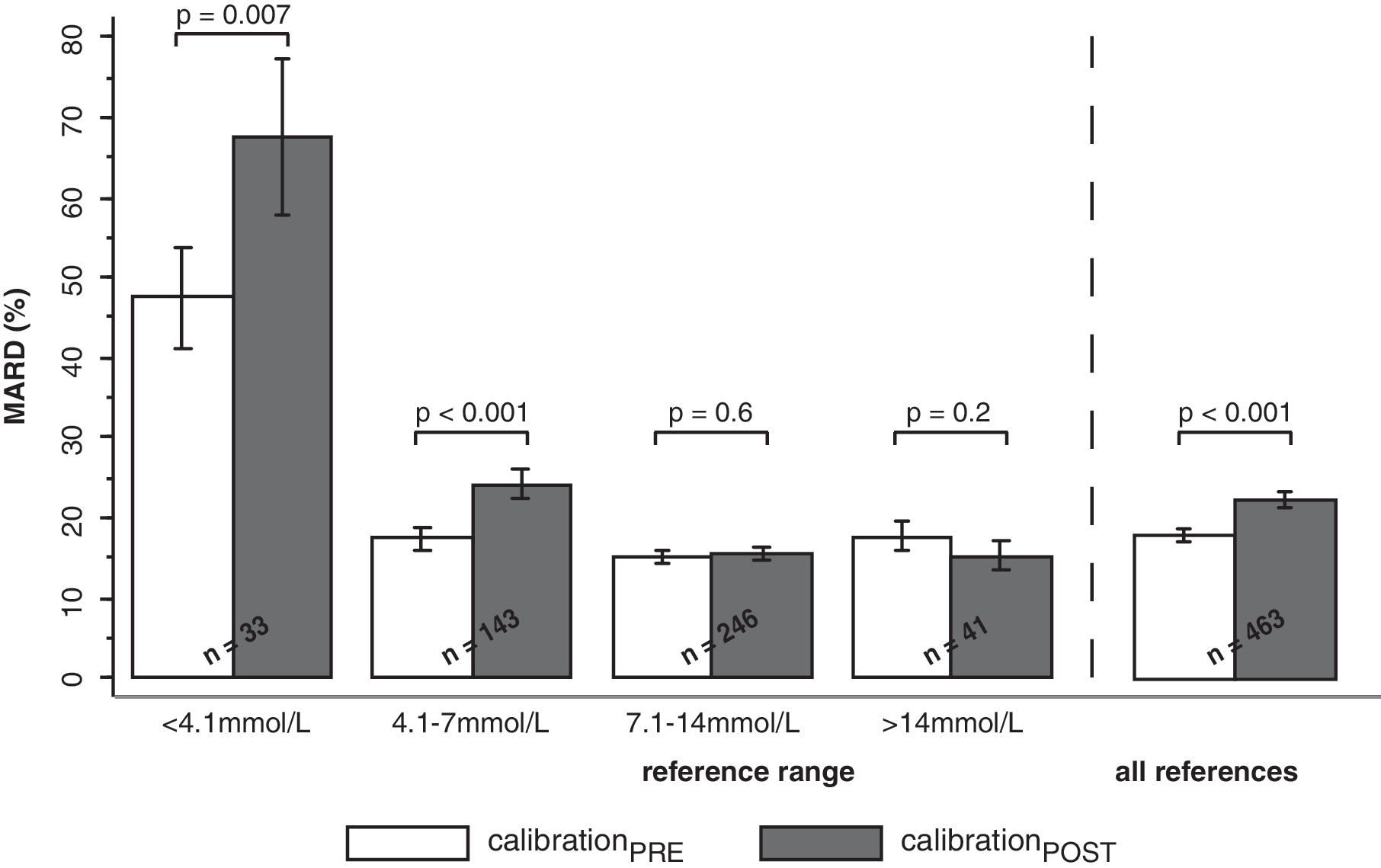
Mean absolute relative difference (MARD)±SEM of sensor glucose compared with capillary reference values for all data points and according to capillary reference range (left side). calibrationPOST, calibration with predominantly postprandial glucose (solid columns); calibrationPRE, calibration with predominantly preprandial glucose (open columns).
Similarly, the MAD between sensor readings and reference values was 1.43±0.06 mmol/L for calibrationPRE and 1.57±0.07 mmol/L for calibrationPOST (P=0.039). MAD of the low, euglycemic, and hyperglycemic subgroups were 1.43±0.20 mmol/L, 0.93±0.07 mmol/L, 1.49±0.08 mmol/L, and 2.84±0.30 mmol/L, respectively, for calibrationPRE and 2.03±0.27 mmol/L, 1.29±0.09 mmol/L, 1.54±0.09 mmol/L, and 2.41±0.30 mmol/L, respectively, for calibrationPOST. Again, the difference in favor of calibrationPRE was based on significantly lower MAD in the low (P=0.006) and euglycemic (P<0.001) ranges, whereas no difference was apparent in the hyperglycemic ranges (Fig. 2).
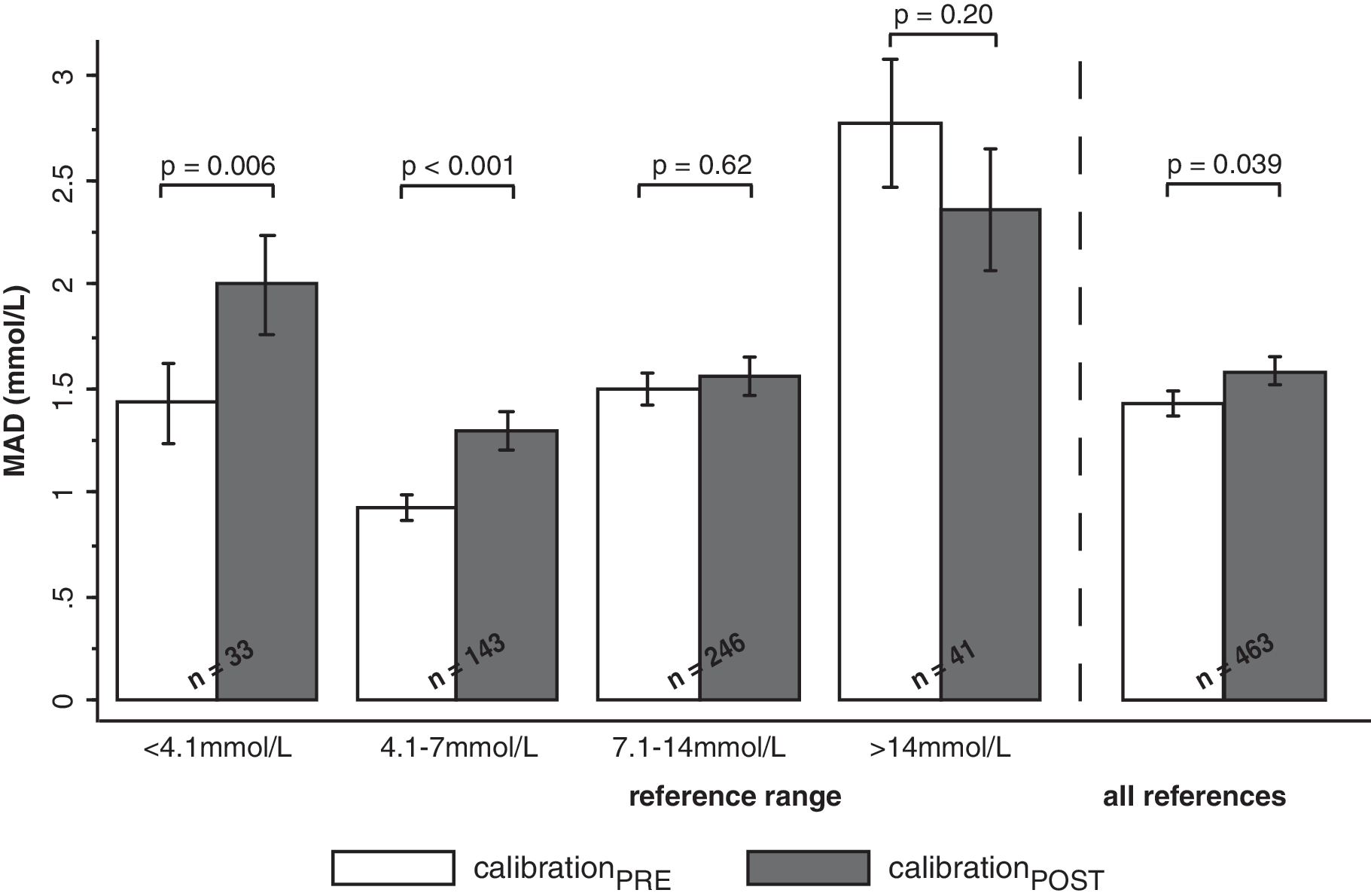
Mean absolute difference (MAD)±SEM of sensor glucose compared with capillary reference values for all data points and according to capillary reference range (left side). calibrationPOST, calibration with predominantly postprandial glucose (solid columns); calibrationPRE, calibration with predominantly preprandial glucose (open columns).
MARD was significantly higher in the lowest range compared with the euglycemic and hyperglycemic ranges (adjusted P≤0.001 for all comparisons).
The correlation between the sensor readings and the SMBG using calibrationPOST was good (coefficient=0.82, P<0.001), the correlation was even better using calibrationPRE (coefficient=0.86, P<0.001) (P=0.039 for comparison of calibration modes).
Figure 3 shows the corresponding Bland–Altman plot: The mean of the differences between the sensor readings and their references was −0.28 mmol/L (95% confidence interval, −0.46 to −0.11) for calibrationPRE and 0.11 mmol/L (95% confidence interval, −0.09 to 0.31) for calibrationPOST (P<0.001). The 95% limits of agreement of the differences between sensor readings and references versus the corresponding means ranged from −4.12 mmol/L to 3.56 mmol/L and from −4.17 mmol/L to 4.39 mmol/L, resulting in a smaller range for calibrationPRE (±3.84 mmol/L) compared with calibrationPOST (±4.28 mmol/L).

Bland–Altman diagram depicting deviation between continuous glucose monitoring (CGM) sensor readings and capillary reference values plotted against their means (open circles for calibration with predominantly preprandial glucose [calibrationPRE or calPRE] and solid triangles for calibration with predominantly postprandial glucose [calibrationPOST or calPOST]). Dashed lines show the mean difference between sensor readings and capillary reference, as well as the corresponding 95% limits of agreement (i.e.,±2 SD) for either calibration pattern.
Discussion
The present study prospectively compared the influence of a predominantly preprandial with a predominantly postprandial calibration pattern on the accuracy of a commercially available CGM device. The main findings are threefold. First, overall MARD and MAD were significantly lower using calibrationPRE compared with calibrationPOST. Second, the superior accuracy with calibrationPRE was based on significantly lower values for MARD and MAD in the low and euglycemic ranges, exclusively, whereas no differences emerged in the hyperglycemic ranges. This indicates that a predominantly preprandial calibration may be particularly useful for individuals with unstable glucose control and an increased risk for hypoglycemia. Third, independently from the calibration mode, MARD was highest in the lowest glycemic range.
To the best of our knowledge this is the first study prospectively assessing the effect of different time points of calibration on sensor accuracy. The present findings are in line with previously reported retrospective data in children showing a decrease in sensor accuracy when calibration was performed during periods of rapid change in blood glucose compared with stable blood glucose values. 5 This can at least partly be explained by the time lag between blood and interstitial glucose measurement. In situations with low glucose fluctuations, equilibration between interstitial and blood glucose is likely to be improved, and therefore the effect of time lag decreases. In contrast, when glucose levels are changing rapidly, the discrepancy between blood and interstitial glucose increases, potentially resulting in a less accurate calibration. 5,7 Because glucose fluctuations generally are more pronounced in postprandial than in preprandial situations, this might explain the higher accuracy of preprandial sensor calibration. It is interesting that despite the general finding of a negative association of sensor accuracy with the rate of change in glucose, Buckingham et al. 5 found no significant difference when comparing pre- and postprandial sensor calibration. There are several possible explanations for this apparent discrepancy to our analysis. The higher number of calibrations per day in their study (four compared with three in our study) might have diluted the differences between the two calibration patterns because the previous authors also reported a higher accuracy by increasing the number of calibrations per day. Furthermore, the present study was performed in adult individuals, and it is conceivable that the rate of glucose change might differ in the both pre- and the postprandial setting between children and adults because of differences in diet or other lifestyle factors.
The improved sensor accuracy associated with a predominantly preprandial calibration mode found in the present study may appear comparably small in absolute terms. Conversely, the difference emerges to be considerably higher in the range of glucose levels below 7 mmol/L and most strikingly in the lowest glycemic range. In view of the increased risk of hypoglycemia in case of deviant sensor readings in the lowest range, such a difference may therefore be of considerable clinical relevance to the patient with type 1 diabetes. This is even more emphasized by the Bland–Altman plot where both calibration modes tended to overestimate the true glucose values in the lower glycemic ranges. Taken together, this implies that individuals with diabetes and particularly those at increased risk for hypoglycemia (e.g., brittle diabetes, hypoglycemia unawareness) should be advised to calibrate in the preprandial period to improve safety.
The finding of an impaired sensor accuracy in the lower glycemic ranges is in accordance with earlier reports from a large retrospective analysis pairing 60,000 sensor values and SMBG values where sensor accuracy was decreased in the range below 6.7 mmol/L. 8 Of note is that MARD in this large study was comparable to the value in the present analysis. Controversy exists about the behavior of interstitial glucose in the hypoglycemic range and the potential interactions with accuracy of the CGM device. 7,9 –11 Monsod et al. 12 showed that the relationship between interstitial and plasma glucose becomes more divergent in hypoglycemia compared with euglycemia, offering a potential explanation for the reduced accuracy in the hypoglycemic range in the present analysis.
The strength of the present study lies in the direct and prospective comparison of two different calibration patterns with the application of the identical sensors at the same time. Furthermore, the setting reflects the use of the system in daily clinical routine, and the results are therefore more likely to be applicable to clinical practice. We nevertheless acknowledge several limitations. First, with 20 individuals our study population was comparatively small. This was essentially due to financial restrictions in terms of CGM devices and sensors. Second, the resulting differences might not only be a result of the different calibration patterns but might potentially be influenced by chance effects in sensor accuracy or the individual adherence to the prescribed calibration protocol. The latter was minimized by the fact that each individual had to fill in a detailed protocol during the study period. Third, the predefined statistical approach used in this study was comparably straightforward. However, results remained robust even when the data were analyzed again using a more complex model. Fourth, although the present study aimed at comparing pre- and postprandial calibration modes, this was compromised by the technical restraints of the CGM devices under investigation (maximum calibration interval of 12 h). As a consequence the two calibration modes under investigation differed with regard to the calibration interval. On the other hand, it could even be hypothesized that the difference between the two calibration modes would have been more pronounced if calibration had been restricted to pre- or postprandial time points, exclusively. Finally, the present study did not take into account potential differences in the rate of change of glucose at the time point of calibration. Therefore, the results of the present study have to remain descriptive and cannot directly be attributed to differences in glucose kinetics.
In conclusion, sensor calibration predominantly based on preprandial SMBG resulted in a significantly higher overall sensor accuracy compared with a predominantly postprandial calibration. The difference is most pronounced in the hypo- and euglycemic reference ranges, whereas both calibration patterns were comparable in the hyperglycemic range. Therefore we recommend preprandial sensor calibration to improve accuracy in the euglycemic and hypoglycemic glucose ranges. Although this conclusion may be applicable to every patient with diabetes in general, it appears particularly important for those at increased risk for hypoglycemia.
Footnotes
Acknowledgments
The authors would like to thank Iris Erdenbrink for her valuable advice, as well as all the volunteers for their enthusiasm.
Author Disclosure Statement
No competing financial interests exist.