
Abstract
Objective:
This study describes the clinical characteristics of childhood- and adolescent-onset type 2 diabetes mellitus (CAT2DM) seen at a diabetes center in southern India.
Research Design and Methods:
Between January 1992 and December 2009, 368 CAT2DM patients were registered. Anthropometric measurements were done using standardized techniques. Biochemical investigations included C-peptide measurements and glutamic acid decarboxylase antibody assay wherever feasible. Retinopathy was diagnosed by retinal photography; microalbuminuria, if urinary albumin excretion was between 30 and 299 mg/μg of creatinine; nephropathy, if urinary albumin excretion was ≥300 mg/μg; and neuropathy, if vibration perception threshold on biothesiometry was ≥20 V.
Results:
The proportion of CAT2DM patients, expressed as percentage of total patients registered at our center, rose from 0.01% in 1992 to 0.35% in 2009 (P<0.001). Among the 368 cases of CAT2DM, 96 (26%) were diagnosed before the age of 15 years. The mean age at first visit and age at diagnosis of the CAT2DM subjects were 22.2±9.7 and 16.1±2.5 years, respectively. Using World Health Organization growth reference charts, 56% of boys and 50.4% of girls were >85th percentile of body mass index for age. Prevalence rates of retinopathy, microalbuminuria, nephropathy, and neuropathy were 26.7%, 14.7%, 8.4%, and 14.2%, respectively. Regression analysis revealed female gender, body mass index >85th percentile, parental history of diabetes, serum cholesterol, and blood pressure to be associated with earlier age at onset of CAT2DM.
Conclusions:
CAT2DM appears to be increasing in urban India, and the prevalence of microvascular complications is high. Female predominance is seen at younger ages.
Introduction
Subjects and Methods
The study group was composed of patients with CAT2DM registered at Dr. Mohan's Diabetes Specialties Centre (DMDSC), a large diabetes center at Chennai in southern India, with over 200,000 registered diabetes patients.
Clinic procedures
At DMDSC, a young diabetes registry has been in existence since its inception, and for all patients in the registry, a standardized protocol is used. After the registration procedure, all patients are seen by the dietician/diabetes educator, who obtains a detailed medical history including current medications and family history of diabetes. Anthropometric measurements include height, weight, and waist measurement using standardized techniques. Waist circumference is measured with a nonstretchable tape by trained observers at the midpoint of the lowest rib cage and the iliac crest, to the nearest 0.1 cm, with the patient in a standing position during end expiration. 7 Body mass index (BMI) is calculated as weight (in kg) divided by height (in m) squared. Blood pressure is recorded in the sitting position in the right arm with a mercury sphygmomanometer using appropriate cuffs and rounded off to the nearest 2 mm Hg. A detailed physical examination is carried out by physicians, specifically looking for signs of insulin resistance like acanthosis nigricans and skin tags.
A fasting venous blood sample is obtained after an overnight fast of at least 8 h. Those without a confirmed diagnosis of diabetes are given anhydrous glucose (75 g) with 300 mL of water, and a 2-h post-glucose sample is drawn. 8 Plasma glucose, total serum cholesterol, triglycerides, and high-density lipoprotein cholesterol are estimated on a Hitachi 912 autoanalyzer (Hitachi, Mannheim, Germany) using commercial kits. Glycosylated hemoglobin (HbA1c) is estimated by high-pressure liquid chromatography using the Variant™ machine (Bio-Rad, Hercules, CA).
Fasting and stimulated (post-breakfast) C-peptide levels are estimated by the electrochemiluminescence method on an Elecsys2010 machine (Hitachi). To obtain the stimulated C-peptide value, we provide a standard breakfast and take a postprandial blood sample at 90 min. This method has been published earlier and has been used in several earlier publications as a measure of stimulated C-peptide as it helps to distinguish type 1 diabetes and type 2 diabetes in our population. 9,10 If the glucose levels are very high, the patients' C-peptide levels could be poor because of glucotoxicity. In such cases, we repeat the C-peptide assay during the next follow-up visit, usually within 3 months, after stabilization of the glucose levels. Among the CAT2DM subjects 48% had their C-peptide level measured within 6 months of their initial diagnosis. For the rest of the CAT2DM subjects who came to us later than 6 months after their diagnosis, the C-peptide levels were measured at the time of registration at our center. If the C-peptide level is good we do not repeat the measurement. If they have clinical features suggestive of CAT2DM but the initial C-peptide level is low, we repeat the C-peptide measurement after stabilization of glucose levels.
Glutamic acid decarboxylase (GAD) antibodies are measured whenever possible on a Bio-Rad plate reader (model 680) using an enzyme-linked immunosorbent assay kit (EUROIMMUN, Lübeck, Germany). The normal limit for GAD antibody assay in our laboratory is less than 10 IU/mL. An abdominal X-ray is routinely done to rule out pancreatic calculi. The DMDSC laboratory is certified by the U.S. College of American Pathologists and the Indian National Accreditation Board for Testing and Calibration of Laboratories.
Definitions
Childhood- and adolescent-onset diabetes was diabetes diagnosed at or below 19 years of age based on fasting plasma glucose (FPG) of ≥126 mg/dL (7.0 mmol/L) and/or 2-h post-load glucose level of ≥200 mg/dL (11.1 mmol/L). 11
This was further subclassified as follows: 1. Childhood- and adolescent-onset type 1 diabetes mellitus (CAT1DM), with a history of diabetic ketoacidosis, fasting and stimulated C-peptide values<0.6 pmol/mL, and requirement of insulin from the time of diagnosis.
12
2. CAT2DM, diagnosed based on the absence of ketosis, good β-cell reserve as shown by stimulated C-peptide assay (≥0.6 pmol/mL), absence of pancreatic calculi on abdominal X-ray, and response to oral hypoglycemic agents for more than 2 years. 3. Gestational diabetes mellitus was diagnosed according to the American Diabetes Association
13
(O'Sullivan and Mahan criteria revised by the National Diabetes Data Group). 4. Fibrocalculous pancreatic diabetes was diabetes plus chronic pancreatitis of unknown etiology.
14
5. Other types of diabetes were cases of diabetes other than those listed above.
World Health Organization growth reference curves for children and adolescents were adopted for defining the height for age and BMI for age and height, and BMI percentiles were divided into three groups as follows: less than median, median to the 85th percentile, and above the 85th percentile. 15 Cardiometabolic risk factors were diagnosed according to the International Diabetes Federation's Consensus Report for Children and Adolescents. 16
To detect retinopathy, the ocular fundi were photographed using four-field stereo color retinal photography (model FF 450 Plus camera, Carl Zeiss, Jena, Switzerland) and graded by an ophthalmologist according to the Early Treatment Diabetic Retinopathy Study criteria. 17 The minimum criterion for diagnosis of diabetic retinopathy was the presence of at least one definite microaneurysm.
Microalbuminuria was defined as urinary albumin excretion of 30–299 mg/μg of creatinine. 18
Nephropathy was diagnosed in those with macroalbuminuria (i.e., urinary albumin excretion of ≥300 μg/mg of creatinine). 18
To detect neuropathy, the vibratory perception threshold of both great toes was measured using a biothesiometer as previously described. 19 The mean value of three measurements was used, and neuropathy was diagnosed if the mean vibratory perception threshold was ≥20 V.
Statistical analysis
SPSS for Windows version 15.0 (SPSS, Inc., Chicago, IL) was used for data analysis. Student's t test was used for continuous variables and the χ2 test for categorical variables. Multiple logistic regression analysis was done using age at onset of diabetes 10–14 years or 15–19 years as the dependent variable; the entry criterion for independent variables into the multiple logistic regression analysis was that the variable had P≤0.05 on univariate analysis.
Results
Between January 1992 and December 2009, in total, 1,372 subjects with childhood- and adolescent-onset diabetes were registered at our center. This group comprised 940 (68.5%) with CAT1DM and 368 (26.8%) with CAT2DM, whereas the rest consisted of gestational diabetes mellitus (n=8), fibrocalculous pancreatic diabetes (n=34), and other types of diabetes (n=22). The rest of this article only deals with CAT2DM.
Figure 1 shows that there has been a gradual increase in CAT2DM (represented as a proportion of the total patients registered at our center during that period), from 0.01% in 1992 to 0.35% in 2009 (P for trend <0.001). Table 1 shows the clinical profile of CAT2DM. Of the CAT2DM cases, 200 of 368 (54.3%) were girls, of whom 67 (33.5%) were diagnosed between 10 and 14 years and 3 (1.5%) below 10 years, whereas the rest (n=130, 65%) were diagnosed between 15 and 19 years. Among boys, 26 (15.5%) were diagnosed between 10 and 14 years and none below 10 years, whereas the rest (n=142, 84.5%) were diagnosed between 15 and 19 years. The mean age at first visit and age at diagnosis of CAT2DM were 22.2±9.7 and 16.1±2.5 years, respectively. The mean systolic and diastolic blood pressures of CAT2DM cases were 119±16 and 79±9 mm Hg, respectively, and the respective mean C-peptide fasting and stimulated values were 0.8±0.4 and 1.6±1.0 pmol/mL.
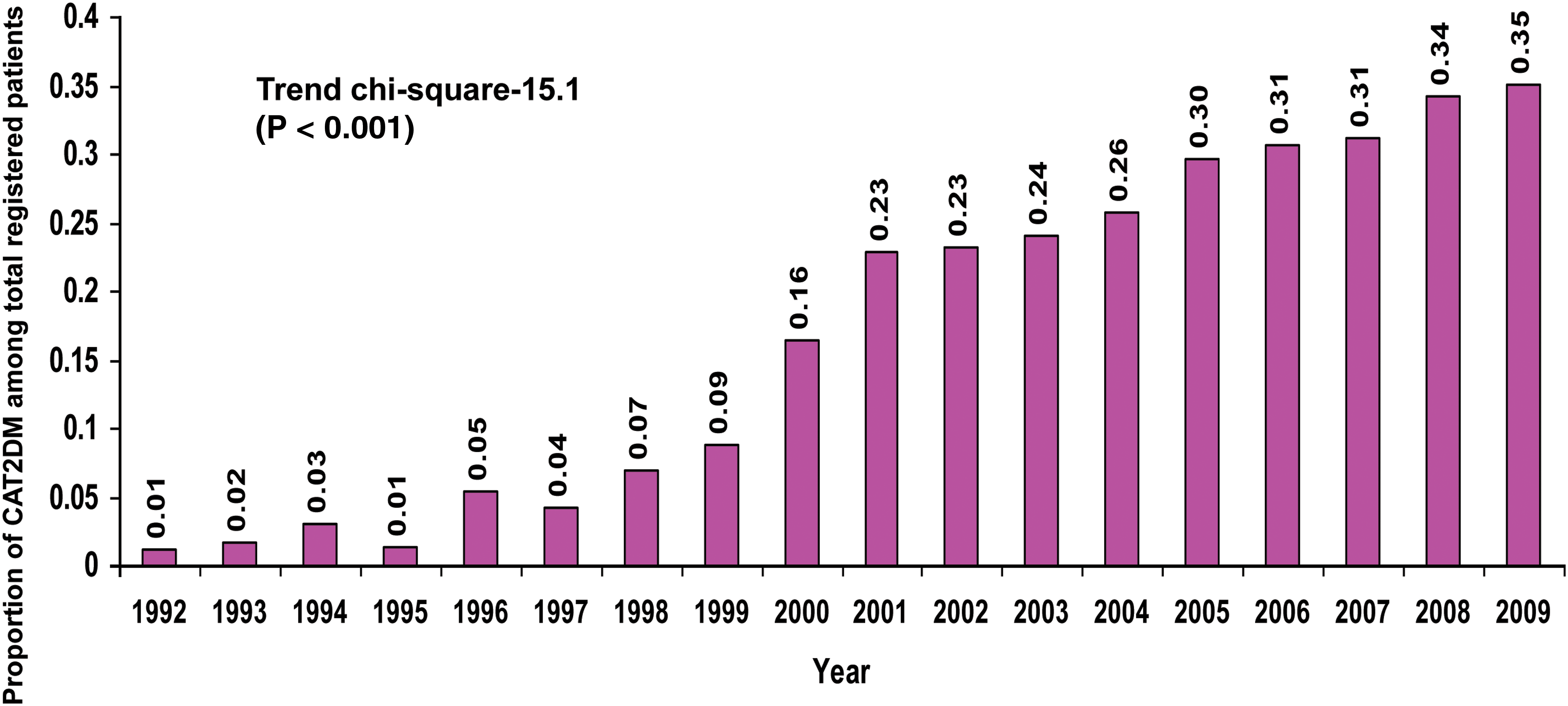
Prevalence of childhood- and adolescent-onset type 2 diabetes mellitus (CAT2DM) shown as a proportion of total patients registered at our center (1992–2009). Color images available online at
Data are mean±SD values.
Value given as mean (SE).
CAT2DM, childhood- and adolescent-onset type 2 diabetes mellitus; GAD, glutamic acid decarboxylase; HDL, high-density lipoprotein; LDL, low-density lipoprotein; OHA, oral hypoglycemic agent.
Acanthosis nigricans was present in 21.2 % of CAT2DM cases, and parental history of diabetes (one or both parents) was seen in 84.8% (312 of 368 subjects). Fifty-nine percent of CAT2DM cases were treated with oral hypoglycemic agents alone, and, by definition, none of the subjects required insulin continuously from the time of diagnosis. Some needed insulin initially to correct glucotoxicity and some later, in addition to oral hypoglycemic agents, in order to control hyperglycemia.
Table 2 shows the clinical and biochemical profile of GAD-positive and -negative CAT2DM subjects. There was no significant difference in any of the parameters studied except for height, which was lower in the GAD-positive CAT2DM cases (P=0.030). Prevalence of microvascular complications stratified by duration of diabetes is presented in Figure 2. As there were no significant differences between boys and girls with respect to any of the complications, the combined prevalence is presented. The distribution of patients by duration of diabetes was as follows: ≤5 years, 219 of 368 (59.5%); >5 years to ≤10 years, 67 of 368 (18.2%); >10 years to ≤15 years, 21 of 368 (5.7%); and >15 years, 61 of 368 (16.6%). Data are presented only for those in whom it was possible to screen for complications. The prevalence of retinopathy rose from 4.2% (eight of 192) in those with diabetes duration of ≤5 years to 81.5% (44 of 54) in those >15 years. The prevalence of microalbuminuria increased from 8.7% (19 of 219) in those with diabetes duration of ≤5 years to 29.5% (18 of 61) in those >15 years, whereas the prevalence of overt nephropathy increased from 9% (six of 67) in those with diabetes duration of >5 to ≤10 years to 34.4% (21 of 61) in those with duration of >15 years. The prevalence of neuropathy was 3% (five of 165) in those with diabetes duration of ≤5 years and increased to 49.2% (30 of 61) in those with duration of >15 years.
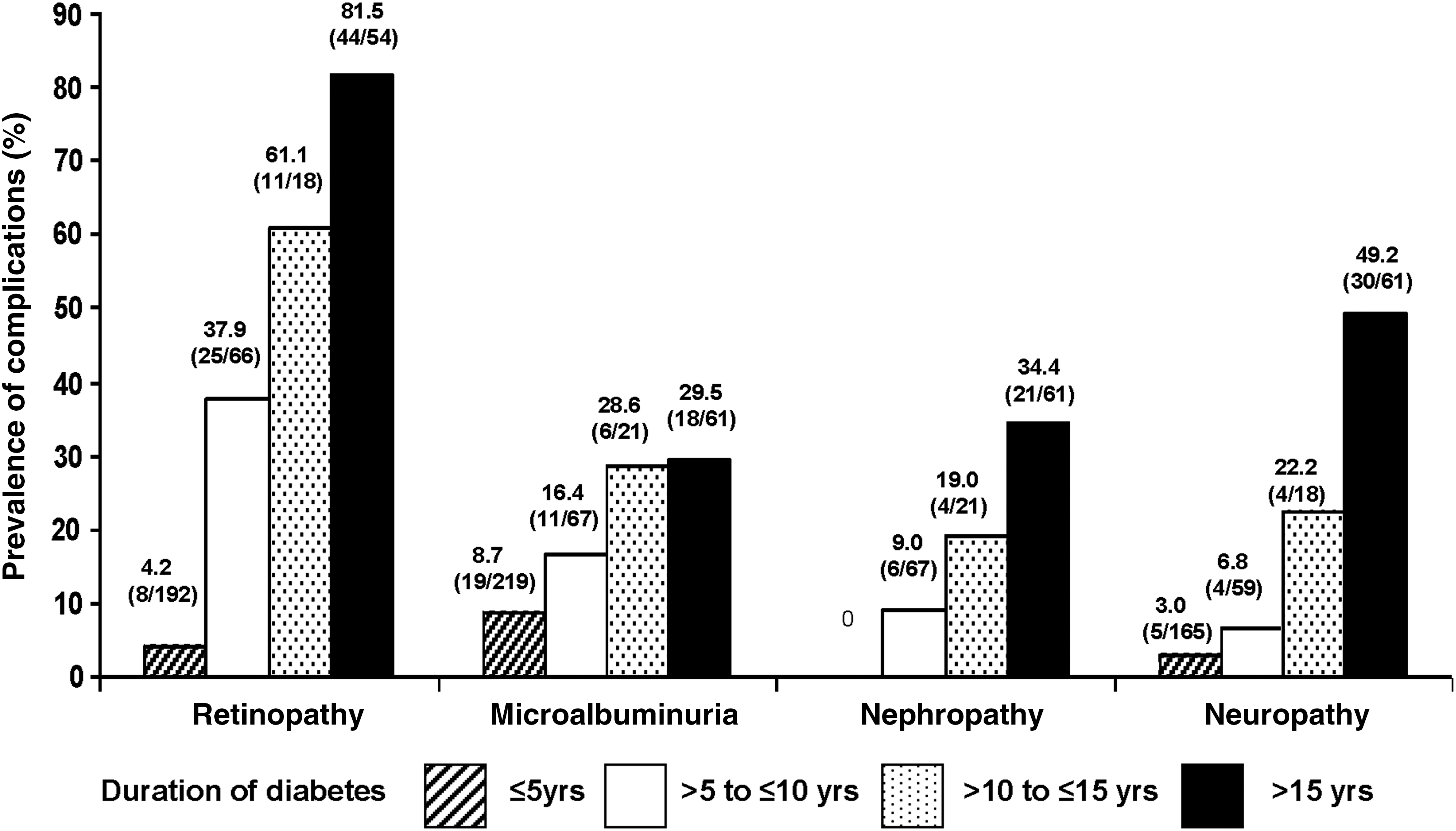
Prevalence of complications stratified according to duration of diabetes among patients with childhood- and adolescent-onset type 2 diabetes mellitus. The total number of patients in each duration category is as follows: ≤5 years, 219/368 (59.5%); >5 years to ≤10 years, 67/368 (18.2%); >10 years to ≤15 years, 21/368 (5.7%); and >15 years, 61/368 (16.6%). Note that the denominator shown is the number of patients in whom tests were done.
Data are mean±SD values.
GAD, glutamic acid decarboxylase; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
In order to find out the proportion of overweight, obese, and cardiometabolic risk factors in children and adolescents by using World Health Organization growth standards criteria for classifying obesity and the International Diabetes Federation consensus report for metabolic syndrome in children and adolescents, we studied a subset of 202 patients with type 2 diabetes who were 10–19 years of age at the time of their first presentation to our clinic, and only their data are analyzed in Tables 3 and 4. Subjects who were >19 years of age at initial presentation at our center were excluded from the analysis as they could not be analyzed using pediatric normative data, and it was not clinically meaningful.
BMI, body mass index; HDL, high-density lipoprotein; WHO, World Health Organization.
For the dependent variable, 10–14 years at onset of diabetes was coded as 2, and 15–19 years at onset of diabetes was coded as 1.
Body mass index (BMI) of >85th percentile was coded as 1, and <85th percentile as 0.
Either or both parents coded as 1 and no parent as 0.
Serum cholesterol of ≥200 mg/dL was coded as 1 and <200 mg/dL as 0.
Blood pressure of ≥130/85 mm Hg was coded as 1 and <130/85 mm Hg as 0.
Using World Health Organization growth reference charts, 56% of boys and 50.4% of girls were >85th percentile of BMI for age, and 26.2% of boys and 32.5% of girls had BMI values in the median to 85th percentile (Table 3). Among the cardiometabolic risk factors, a high percentage of low high-density lipoprotein cholesterol was found in both genders (61.1% of boys vs. 69.2% of girls).
Multiple logistic regression analysis (Table 4) was performed to determine the association of age at onset of diabetes with gender among the two age groups (10–14 years, coded as 2, and 15–19 years, coded as 1). The various risk factors derived through univariate analysis were gender (female), which had the highest odds ratio (OR) (OR 3.785, 95% confidence interval [CI] 1.917–7.472, P<0.001), followed by BMI (OR 2.178, 95% CI 1.177–4.029, P=0.013), parental history of diabetes (OR 1.784, 95% CI 1.109–2.869; P=0.017), serum cholesterol (OR 0.309, 95% CI 0.121–0.789, P=0.014), and blood pressure (OR 0.367, 95% CI 0.159–0.844, P=0.018). In the logistic regression, age at onset of diabetes (10–14 years) was taken as the dependent variable and gender as the independent variable. The analysis showed that girls had higher risk of developing diabetes at younger age (10–14 years) (OR 3.73, 95% CI 1.70–8.19, P=0.001) even after adjusting for BMI, parental diabetes history, serum cholesterol, and blood pressure.
Discussion
Until recently, childhood-onset diabetes was considered synonymous with type 1 diabetes. However, there has been a gradual increase in the number of CAT2DM subjects reported over the years in many parts of the world, including Asia. 6,20,21 Recent reports indicate that up to 45% of all childhood- and adolescent-onset diabetes at some centers consists of CAT2DM. 3
It is reported that Asian Indians have an increased susceptibility to type 2 diabetes, and according to a recent national study, India is home to 62 million people with diabetes. 22,23 In this context the present study, which examines the largest series of CAT2DM from India, assumes significance. We report that there has been a gradual increase in percentage of CAT2DM seen at our center. Although this may well be due to more cases being referred to a specialist diabetes center or due to increased awareness of the condition, it is also possible that CAT2DM is increasing in urban Indian children, consistent with the increasing obesity rates. 24 –26
Age at diagnosis of 19 years or below was taken as the cut point to discriminate adolescence from adulthood because in our earlier studies, we had used an age onset of 20 years and above to define adults (e.g., in our CUPS, 27 CURES, 28 and ICMR-INDIAB 22,29 studies). The SEARCH for Diabetes in Youth done in the United States 3 and the Indian Multicenter Study 30 also used an age cutoff as <20 years to define youth-onset diabetes.
A significant percentage of our girls developed CAT2DM before the age of 15 years. This has also been reported in other ethnic groups. 4,21,31 Multiple logistic regression analysis revealed that girls 10–14 years old have a higher risk of developing diabetes even after adjusting for BMI, parental history, serum cholesterol, and blood pressure. It is well known that the onset of puberty leads to increased insulin resistance and that hormonal change due to puberty could be a triggering factor for developing CAT2DM in girls. 32
In our study, 23.1% (45 of 195) of girls had clinical symptoms of polycystic ovarian syndrome (PCOS), and among the rest, 5 had not attained menarche at the time of presentation to the center. Among the subjects with PCOS, 64% had a BMI of >85th percentile. There was no correlation of PCOS with major end points like retinopathy or nephropathy, but the prevalence of hypertension was high in those with PCOS. There are very limited data on the incidence of type 2 diabetes in adolescents with PCOS and its complications, and undoubtedly studies are needed to address these issues.
The majority of our CAT2DM had a BMI above the median and over 50% above the 85th percentile, but 17.9% of boys and 16.2% of girls had a BMI below the median. This may partly be explained by the fact that the World Health Organization cut points used may be inappropriate (i.e., too high for our population). Even among adults we 33 and others 34 have shown that lower BMI cut points (e.g., >23 kg/m2) are more appropriate in our region. However, even given these differences due to different cut points, some of our CAT2DM cases are undoubtedly nonobese. This is one of the first studies, to our knowledge, to report on nonobese CAT2DM. This is consistent with reports on T2DM in adults in India, where a good proportion of T2DM cases are lean. 35 Whether this lean group has different etiopathogenic mechanisms (e.g., greater insulin secretion deficit rather than insulin resistance) merits more studies.
History of diabetes in one or both parents was seen in over 80% of CAT2DM subjects, and this figure corroborates a previous study done in children, adolescents, and young adults from North India. 36 However, acanthosis nigricans was seen only in a quarter of our CAT2DM cases. Hence this clinical sign, while useful if present, cannot be relied on as a diagnostic marker for CAT2DM.
For diagnosis of CAT2DM, we chose a combination of clinical and biochemical criteria including C-peptide estimation. There are several problems with using a single C-peptide cut point in a clinic. At the time of presentation, C-peptide levels may be low in T2DM because of glucotoxicity, which can improve on follow-up. 8 Again, during the remission phase of type 1 diabetes mellitus, C-peptide levels may be good. Finally, C-peptide values are dependent on the type of assay and the laboratory that performs the assay, and hence it is unlikely that a single cut point can be universally adopted. We have found that a combination of clinical criteria and C-peptide criteria is largely helpful for classification of our children with diabetes, and this also has been reported by Ludvigsson et al. 37 Moreover, repeating the C-peptide measurement after the glucotoxicity is corrected often helps distinguishing type 1 and type 2 diabetes. 8
The presence of GAD antibodies is a useful pointer to type 1 diabetes. 38 However, a small proportion of CAT2DM subjects also may have GAD antibodies. 36,39,40 Unfortunately, owing to financial constraints we were able to carry out GAD antibody assay only in 141 CAT2DM subjects, and six of them were positive for GAD antibodies (4.3%). The clinical profile of these subjects was not significantly different from the GAD-negative subjects. When the GAD-positive CAT1DM and CAT2DM cases seen at our clinic were compared, significant differences were seen in their clinical profile, with the CAT2DM subjects having greater BMI, family history of diabetes, and significantly higher C-peptide values (data not shown).
It is not surprising that a clustering of cardiometabolic risk factors is seen in both male and female CAT2DM subjects. The presence of multiple cardiovascular risk factors such as dyslipidemia and raised blood pressure shows that CAT2DM subjects are at increased risk of developing cardiovascular disease in the future. This underscores the need for prevention and aggressive control of these risk factors in childhood in order to prevent premature cardiovascular disease in the future.
One of the disturbing features in our study is the high frequency of microvascular complications. Overall, 26.7% of cases had retinopathy, and two subjects had retinopathy at the time of diagnosis of diabetes. Moreover, in those with diabetes duration of >16 years, >80% had retinopathy. There are some reports suggesting that CAT2DM is a more aggressive disease, and in one series 41% of adolescent T2DM subjects had retinopathy. 41
Overall, microalbuminuria was found in 14.7% and overt nephropathy in 8.4% of the CAT2DM cases. In a Japanese study, higher figures were reported, perhaps because of longer duration of diabetes in their series. 42 In our series also, in those with diabetes duration of >15 years, 29.5% had microalbuminuria, and 34.4% had overt nephropathy.
There are few reports on the prevalence of neuropathy in CAT2DM. An Australian study reported that there is equal prevalence of neuropathy in type 1 and type 2 diabetes despite the shorter duration of diabetes in T2DM. 43 We report that even using a relatively less sensitive technique (biothesiometry), 14.2% had neuropathy. Obviously, if more sensitive techniques such as nerve conduction studies were used, the prevalence of neuropathy would have been much higher.
This study has certain limitations. First, it is a clinic-based study restricted to one private tertiary-care diabetes center in southern India. Second, some of the patients were treated at other centers before they were referred to our center. Third, because ours is a referral center, there could be referral bias of the subjects attending the center. Therefore the conclusions from the study cannot be extrapolated to the whole of India. The Indian Council of Medical Research recently set up a national registry of diabetes in the young (onset <25 years of age). This shows that private diabetes centers have more cases of young-onset T2DM, whereas government hospitals mostly deal with type 1 diabetes. This is probably a socioeconomic issue as the free supply of insulin would attract type 1 patients to government hospitals, whereas the more affluent with obesity-related T2DM would visit private diabetes centers. We could not screen for complications in all, as there were compliance issues in some adolescents. Finally, GAD antibodies could not be tested for all patients. The strengths of the study are the large number of CAT2DM cases studied and the data on complications in CAT2DM, which is the first from India and South Asia.
In summary, we report that CAT2DM is not uncommon in urban diabetes centers in India, particularly in private centers. Girls tend to develop the disorder earlier than boys. Cardiometabolic risk factors are common, and the prevalence of microvascular complications is high. The presence of parental diabetes along with overweight/obesity would justify screening for CAT2DM in this ethnic group. Lifestyle modifications including diet and exercise along with appropriate medications and good control of diabetes and associated risk factors could help reduce the morbidity due to CAT2DM.
Footnotes
Acknowledgments
We gratefully acknowledge Mrs. Jebarani Saravanan (Information Technology), Mrs. Manjula (Medical Records), Ms. B. Mohanavalli and Ms. P. Latha for data management support.
Author Disclosure Statement
No competing financial interests exist. V.M. conceived the study and revised all drafts of the article. A.A. coordinated the study and did all the data entry, checked the integrity and accuracy of results, and wrote the first draft of the article. M.D. provided the statistical input and interpretive analysis of the data. R.U. and R.M.A. gave valuable comments and suggestions and contributed to the case selection and to the writing of the article.