
Abstract
Background:
The performance and accuracy of the Enlite™ (Medtronic, Inc., Northridge, CA) sensor may be affected by microbubble formation at the electrode surface during hypo- and hyperbaric conditions. The effects of acute pressure changes and of prewetting of sensors were investigated.
Materials and Methods:
On Day 1, 24 sensors were inserted on the right side of the abdomen and back in one healthy individual; 12 were prewetted with saline solution, and 12 were inserted dry. On Day 2, this procedure was repeated on the left side. All sensors were attached to an iPro continuous glucose monitoring (CGM) recorder. Hypobaric and hyperbaric tests were conducted in a pressure chamber, with each test lasting 105 min. Plasma glucose values were obtained at 5-min intervals with a HemoCue® (Ängelholm, Sweden) model 201 glucose analyzer for comparison with sensor glucose values.
Results:
Ninety percent of the CGM systems operated during the tests. The mean absolute relative difference was lower during hyperbaric than hypobaric conditions (6.7% vs. 14.9%, P<0.001). Sensor sensitivity was slightly decreased (P<0.05) during hypobaric but not during hyperbaric conditions. Clarke Error Grid Analysis showed that 100% of the values were found in the A+B region. No differences were found between prewetted and dry sensors.
Conclusions:
The Enlite sensor performed adequately during acute pressure changes and was more accurate during hyperbaric than hypobaric conditions. Prewetting the sensors did not improve accuracy. Further studies on type 1 diabetes subjects are needed under various pressure conditions.
Introduction
For those who have diabetes, there are restrictions regarding aviation as well as scuba diving. In most countries, those with type 1 diabetes are prohibited from working as a pilot, but in the United States an individual with the disease may be considered for a third-class airman medical certificate by demonstrating good overall diabetes control. In some countries, recreational diving is prohibited for those with either type 1 or insulin-treated type 2 diabetes.
Self-monitored blood glucose (SMBG) is frequently used as the most common method of obtaining glucose measurements, but SMBG only provides a value when sampling is carried out. The accuracy of SMBG readings is important when used to evaluate the insulin dose or to initiate treatment of hypoglycemic episodes. Glucose meters with inaccuracies (measured as the mean absolute relative difference [MARD] between SMBG readings and paired readings from a reference instrument) below 15% are unlikely cause large insulin dosing errors. 1
Atmospheric pressure and the partial pressure of oxygen can affect the accuracy of a glucose meter. Test strips using the glucose dehydrogenase method are affected less than test strips using glucose oxygenase, and differences are seen among meters from different manufacturers. 2 Altitude also has an impact on the accuracy of glucose readings, 3 as do temperature and relative humidity. 4 The glucose meters underestimated glucose levels by approximately 1–2% for each 1,000 feet of increased elevation after correction for changes in temperature and humidity.
New pharmacological agents for the treatment of diabetes have been developed with the aim of reducing the risk of hypoglycemia. In parallel to this, continuous glucose monitoring (CGM) is also possible. Today, CGM can provide data either retrospectively or in real time. This technique enables detection as well as reduction of hypoglycemia. 5 –7 An individual assessment of diabetes subjects' risk of hypoglycemia is of importance during activities such as flying and recreational scuba diving. 8,9
The number of hypoglycemic events may be decreased when monitors showing glycemic trends or equipped with predictive alarms prompt appropriate intervention. 10 However, glycemic excursions during hypobaric (flying) or during hyperbaric (diving) conditions have not been carefully evaluated, nor have CGM techniques been assessed for accuracy during changes in atmospheric pressure. The aim of the present study was to evaluate the accuracy and reliability of the Enlite™ (Medtronic, Inc., Northridge, CA) subcutaneous glucose sensor in hypobaric and hyperbaric conditions and to determine whether prewetted sensors improve the accuracy of sensor readings.
Research Design and Methods
Participant
One healthy individual was included. Study eligibility required scuba diving certification and a past experience of pressure chambers. Prior to the test, a health declaration and laboratory test certified that the individual was in good health. One healthcare professional accompanied the participant in the pressure chamber for adverse event monitoring and frequent blood sampling. The ethics committee at Uppsala University, Uppsala, Sweden, approved the study protocol (Dnr. 2010/246), and signed informed consent was obtained prior to the study procedures.
Glucose measurements
Capillary blood glucose (P-glucose) values were measured by a healthcare professional using a HemoCue (Ängelholm, Sweden) model 201 glucose analyzer at 5-min intervals.
CGM system
Forty-eight Enlite glucose sensors were used together with iPro™ (Medtronic) recording devices. A prototype firmware was used to collect data in the iPro recorder at a faster sampling rate, 1-min intervals, compared with the commercial version, 5-min intervals. On Day 1, 24 sensors were inserted on the right side of the body, on the abdomen and back. Twelve of the sensors were prewetted with a sterile saline solution prior to insertion, whereas the other 12 sensors were not. Sensors were calibrated to two P-glucose values prior to pressure changes and to two P-glucose values after the pressure changes. After the 2-h sensor initialization period and a stabilization period at 1.0 atm outside the pressure chamber, the hypobaric test was implemented. On Day 2, the insertion procedure was repeated with 24 new sensors being inserted on the left side of the body. After the initialization and stabilization period the hyperbaric test was then conducted.
Study design
The study was performed in a 15-m3 hypobaric/hyperbaric pressure chamber at the Hyperbaric Medicine Unit at Karolinska University Hospital, Stockholm, Sweden. The ambient pressure during the experiment was varied according to Figure 1.
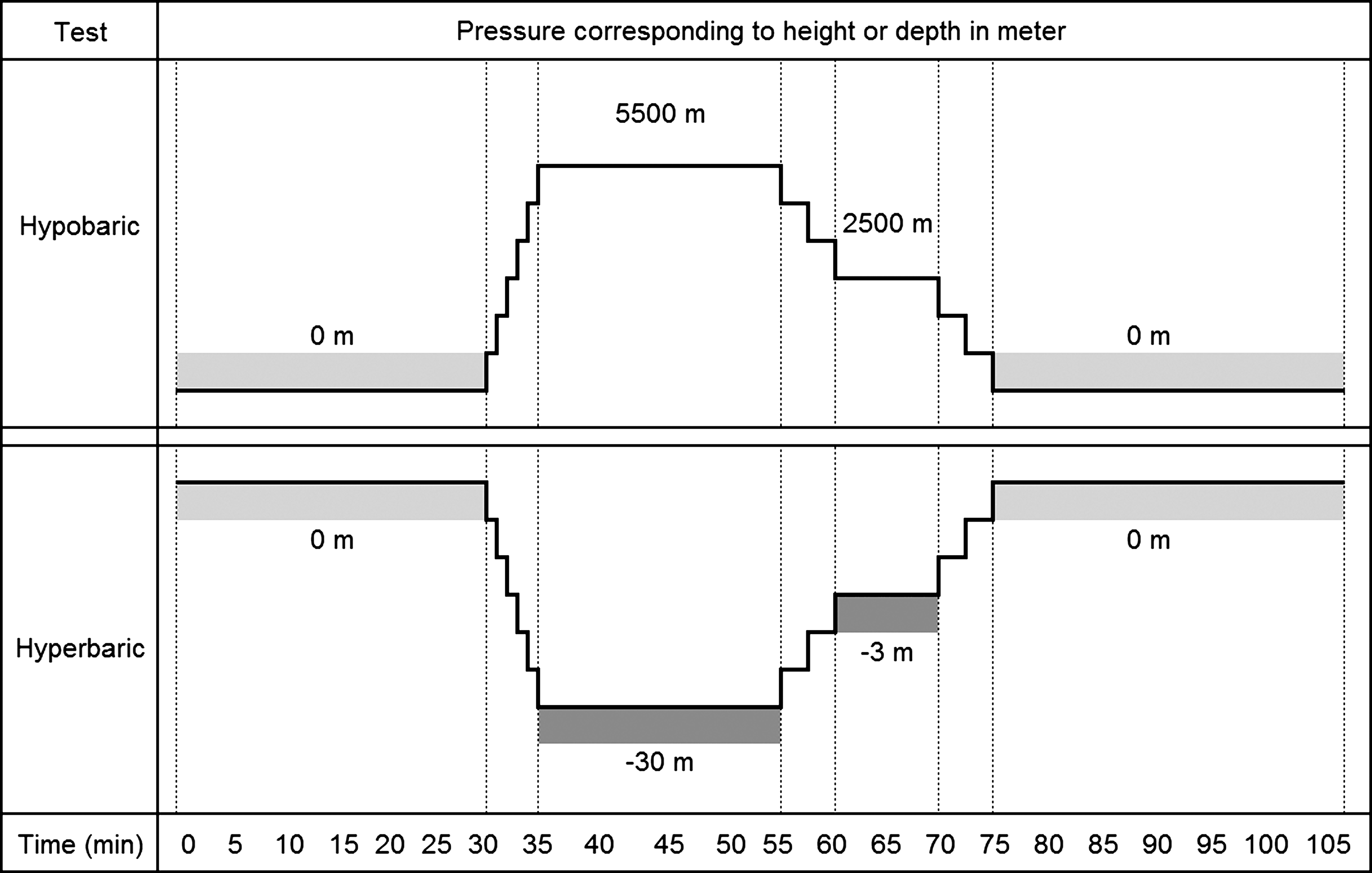
Study design of hypo- and hyperbaric tests. Pressure illustrated corresponding to height or depth in meters.
On Day 1, after the stabilization period of 30 min at 101 kPa/758 mm Hg (0 m, 1 atm, 21 kPa of O2), the chamber pressure was reduced to 51 kPa/383 mm Hg (5,500 m, 0.5 atm, 10 kPa of O2) for a period of 20 min and then increased to 75 kPa/563 mm Hg (2,500 m, 0.75 atm, 16 kPa of O2) for 10 min before return to 101 kPa/758 mm Hg (0 m, 1.0 atm, 21 kPa of O2). On Day 2, after the stabilization period of 30 min at 101 kPa/758 mm Hg (0 m, 1.0 atm, 21 of kPa O2), the chamber pressure was increased to 404 kPa/3,030 mm Hg (30 m, 4.0 atm, 84 kPa of O2) for a period of 20 min, followed by a decompression stop at 130 kPa/975 mm Hg (3 m, 1.3 atm, 27 kPa of O2) and return to 101 kPa/758 mm Hg (0 m, 1.0 atm, 21 kPa of O2).
The specific pressure levels were chosen to mimic extensive height (5,500 m) and air cabin pressure (2,500 m) and the specific depth to mimic extensive depth (30 m) and decompression stop at 3 m according to the diving table. 11
In order to evaluate the possible effect of microbubbles, formed at insertion at the sensor tip, half of the sensors were prewetted with a sterile saline solution prior to insertion.
Data analysis
The Statistical Package for the Social Sciences version 19.0 (SPSS, Chicago, IL) was used for statistical analysis. Differences in sensor function during the hypobaric and hyperbaric tests were evaluated using the Wilcoxon signed rank test. Sensor accuracy was evaluated by comparison with contemporaneous blood glucose values as the MARD, defined as 100×the absolute value of ([sensor glucose – P-glucose]/P-glucose). The Mann–Whitney test was used for comparison of dry and prewetted sensor accuracy under hypobaric and hyperbaric conditions. Clarke Error Grid Analysis plots were generated to evaluate the distribution of sensor glucose values. Sensitivity variation is defined as the state of the sensor: Sensitivity variation=1/(meter P-glucose/paired ISIG). Meter P-glucose is defined as that measured with the HemoCue device, and ISIG is the electrical output of the glucose sensor. Sensitivity variation is a method to determine the stability of the sensor over time and was evaluated during the different pressures. The Kruskal–Wallis test was used for comparisons of sensitivity versus pressure. A P value of<0.05 was regarded as significant.
Results
All of the sensors (24 of 24 [100%]) worked during the hyperbaric test, compared with 19 of 24 (79%) during the hypobaric test (P=0.025). All cases of failure during the hypobaric test, the first test in the study, were determined to be a result of the prototype firmware used to collect data in the CGMS recorder at a faster sampling rate than the commercial version. Once the failure was detected during the hypobaric test, the units were reprogrammed to correct the firmware failure and subsequently used during the second test, which was under hyperbaric conditions.
The mean ISIG values (in nA) from all sensors and the timing of the calibration during the hypobaric and hyperbaric test are shown in Figure 2.
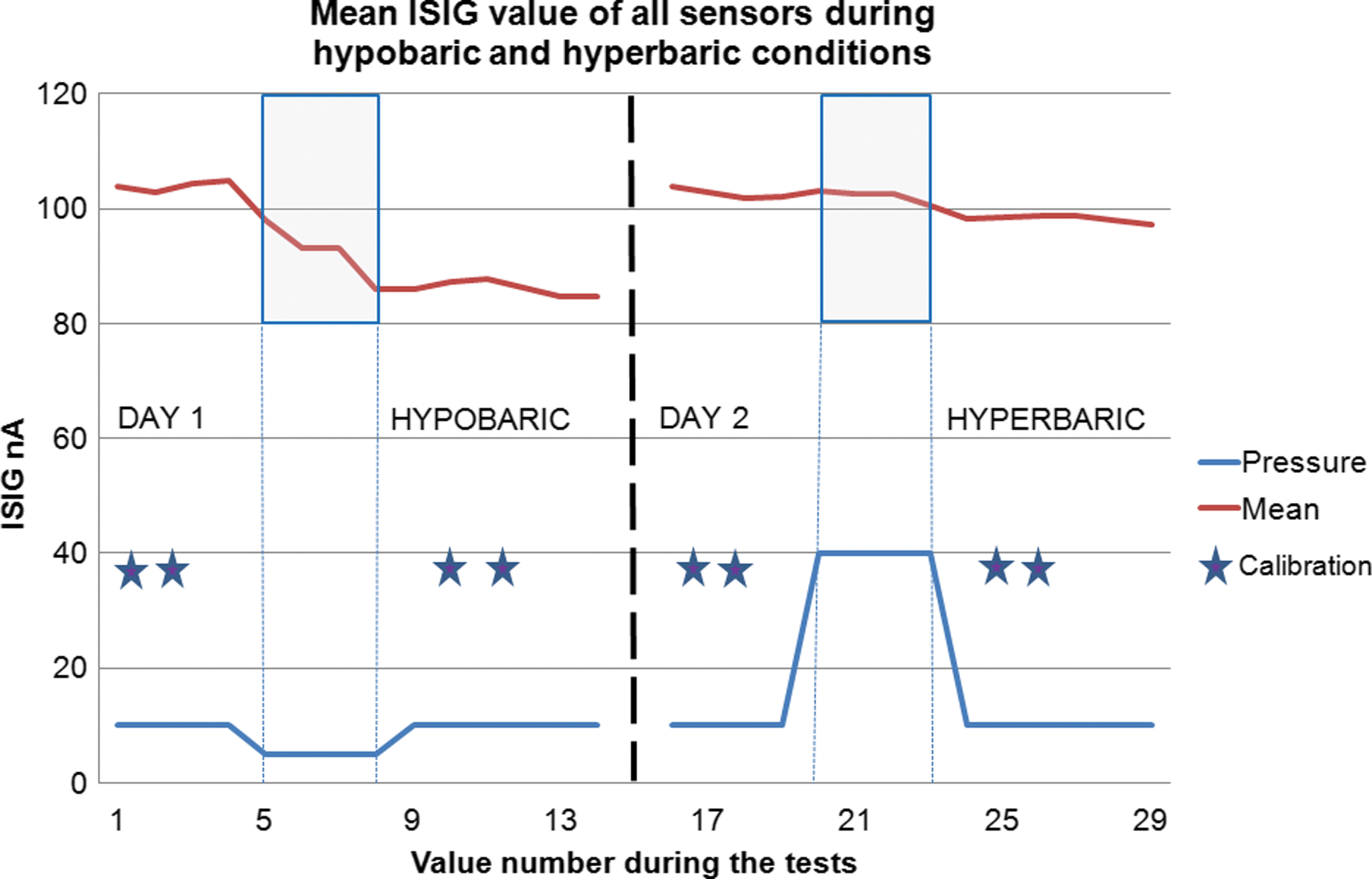
Mean electrical output of the glucose sensor (ISIG) values (in nA) from all sensors during the hypobaric and hyperbaric tests. Calibration of the sensors was conducted before and after pressure changes. Calibrations and pressure changes are illustrated to enhance interpretation of the figure. Color graphics available online at
During the hypobaric test, sensor accuracy (MARD) was 14.9±9.1% (95% confidence interval, 13.1–16.7) and was significantly lower during the hyperbaric test (6.7±7.9% [95% confidence interval, 5.8–7.5]) (P<0.001). The variation of sensor sensitivity at different pressure conditions is demonstrated in Table 1. Figure 3 shows a separate analysis of all sensors and the MARD of each sensor during both tests, illustrating that MARD was consistently lower during the hyperbaric test. When all sensor values were analyzed with the Clarke Error Grid Analysis, 100% of the sensor values were found to be in the A+B region.
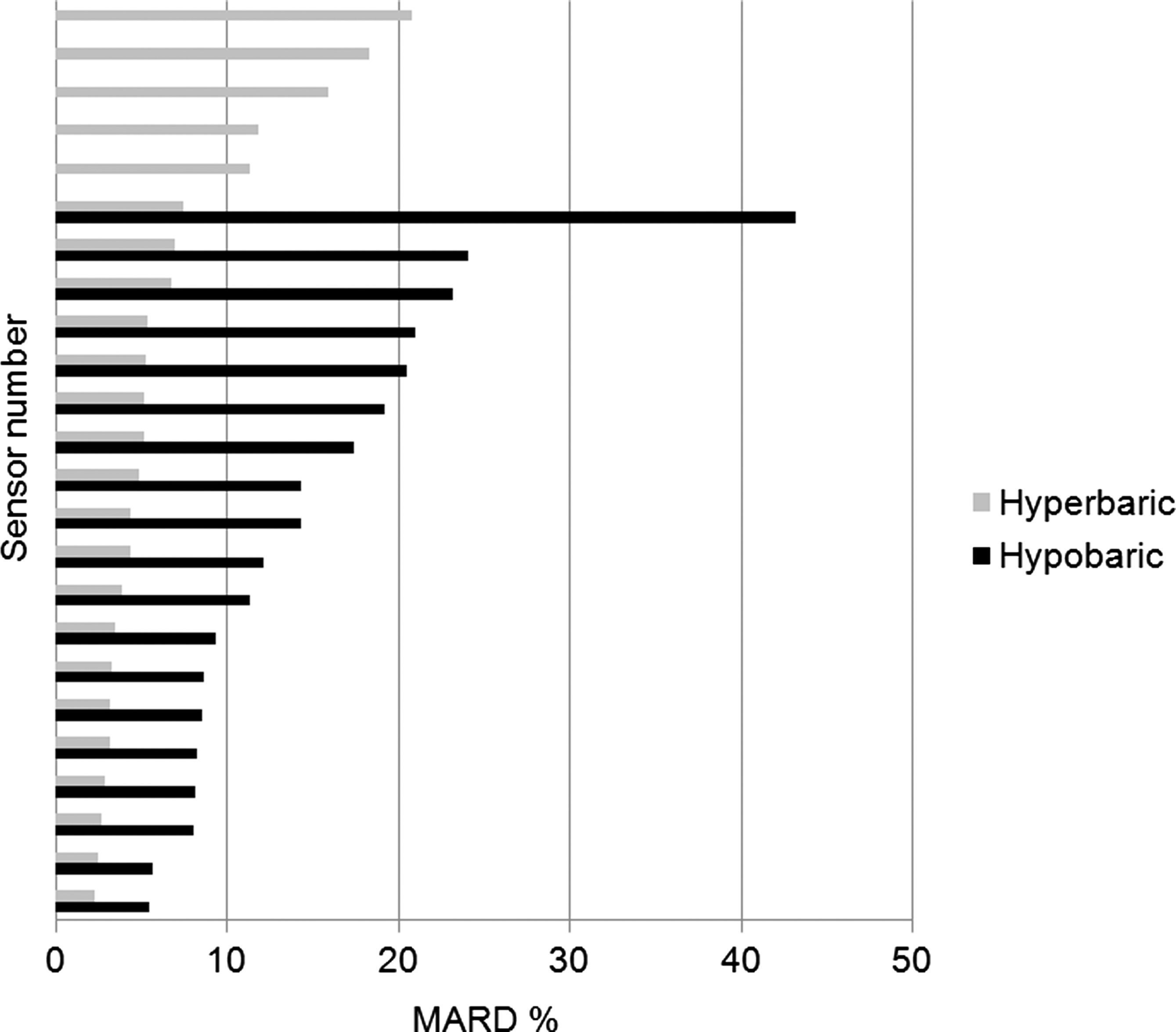
A separate analysis of all in vivo sensors and their accuracy, measured as mean absolute relative difference (MARD) (%), in hypo- and hyperbaric conditions. The respective condition's MARD was lower during the hyperbaric test (6.7%) compared with the hypobaric test (14.9%) (P<0.001).
Data are presented for hypobaric and hyperbaric tests. Sensitivity was examined as 1/(meter P-glucose/paired ISIG), where P-glucose is capillary blood glucose measured with the HemoCue device and ISIG is the electrical output of the glucose sensor.
The sensitivity variation was assessed during the altered pressures. When a glucose sensor is calibrated, its electrical output (ISIG) is related to the blood glucose value at that specific time. A stable relationship between P-glucose and ISIG signal would verify that altered pressure does not affect the ISIG signal. During hyperbaric conditions no significant differences were seen. However, when the sensitivity was evaluated during hypobaric conditions, a higher value of 1/sensitivity (meter P-glucose/ISIG) was seen at 51 kPa/383 mm Hg (5,500 m height) and at 75 kPa/563 mm Hg (2,500 m height) compared with the corresponding value at 101 kPa/758 mm Hg (sea level=0 m) (P<0.001). This means that the ISIG signal was increased in relation to P-glucose during hypobaric conditions. Table 1 and Figure 4 show sensitivity variations during both tests.
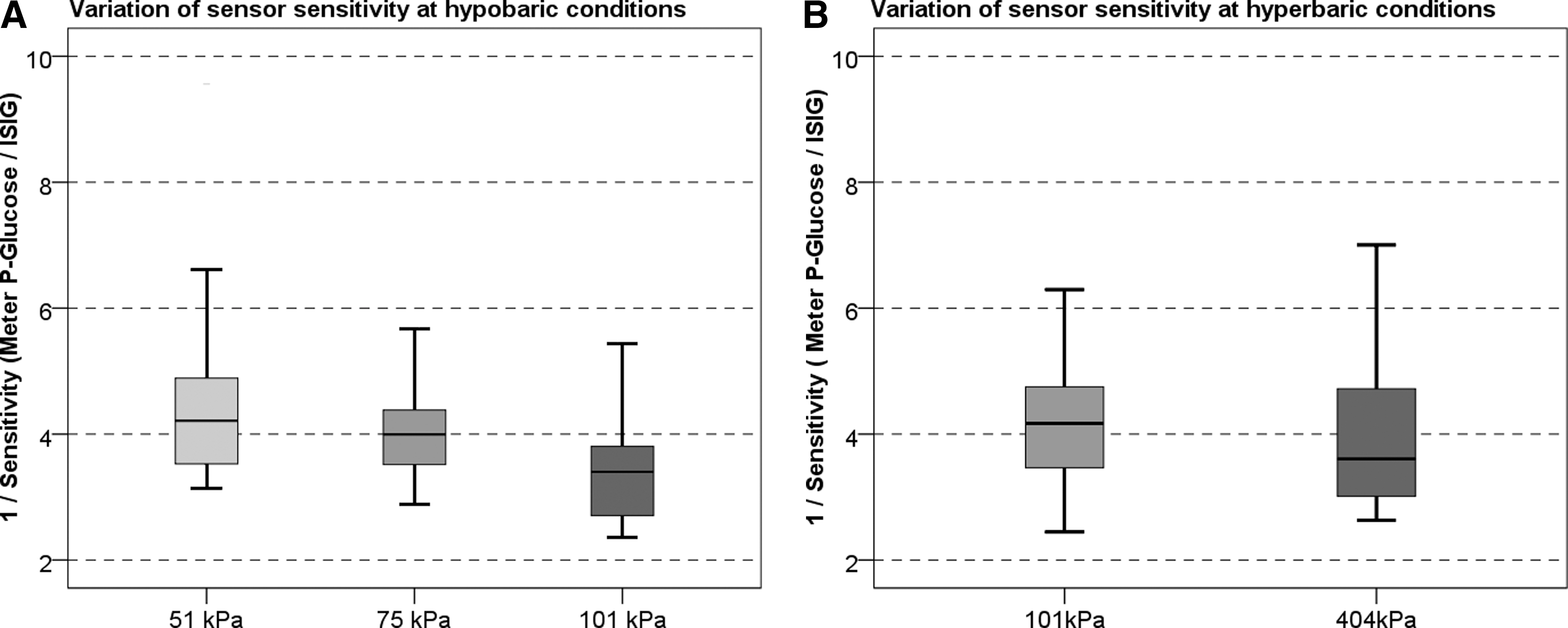
Variation of sensor sensitivity within the instrument's specification 1.5–15, in
No significant difference was found between MARD for the prewetted sensors (11.3±9.5%; 95% confidence interval, 6.4–15.2) and for dry sensors at insertion (9.4±6.8%; 95% confidence interval, 5.6–11.8).
Discussion
In this study we demonstrate that use of the Medtronic Enlite sensor in hypo- and hyperbaric conditions resulted in satisfying sensor and system performance, indicating that use of CGM in people with diabetes, in these specific conditions, may also be justified.
CGM has previously been evaluated in hyperbaric conditions in connection to recreational scuba diving 8,9,12 but not in hypobaric conditions. The CGMS® (Medtronic) that was used in these studies on divers with type 1 diabetes and healthy controls showed promising results as it was possible to evaluate the glucose fluctuation during dive 8,12 and to detect hypoglycemia before, during, or after a dive. 8 Furthermore, it was possible to identify those individuals suitable for diving. 8 The CGMS was used with good accuracy, having a mean MARD of 14.4±6%, during a 3-day period and five dives, 9 which also is confirmed by an outpatient ambulatory study with a MARD of 15.8%. 13 In our study we recorded acceptable MARD values during both hypobaric (14.9%) and hyperbaric (6.7%) tests, which are below the 15% level suggested as the limit for proper adjustment of insulin dosing. 1 In the Clarke Error Grid Analysis, we also found all values in the A+B region of clinically accurate results. One possible contributing factor to the relatively low MARD seen in our study could be that two blood glucose values were used to calibrate the sensors prior to the pressure changes and another two values after the tests. Another contributing factor is that the participant was a healthy individual, with a stable glycemic control. As we did not note any large rates of change in glucose we did not experience any problem about the time lag between blood and interstitial glucose. The described time lag between interstitial and blood glucose values 14 may otherwise contribute to increased MARD. Although we show that sensors could be used during both conditions, significantly more systems failed during the hypobaric test; we attribute this to a failure of the prototype firmware used to collect data in the CGMS recorder. In the hypobaric conditions, MARD was significantly increased compared with MARD in hyperbaric conditions. A lower oxygen partial pressure in hypobaric conditions could be one explanation of the increased MARD as this has been shown to affect home glucose meters. 2 This phenomenon merits further investigation.
The difference recorded can also be attributed to the increased variation in sensor sensitivity, also seen during the hypobaric test. Sensitivity variation is a method to calculate the change in sensitivity over time, from point to point, during conditions of changes in environment (ie oxygen partial pressure, pressure conditions). The clinical significance of the decreased sensitivity under hypobaric conditions might be of minor importance taking into account the values of sensor sensitivity during our tests. A test to determine this variation in sensor sensitivity shows that the variation was well within the sensitivity threshold of 1.5–15 as defined by the real-time device.
In this study it was hypothesized that microscopic gas bubbles formed at insertion of the sensor might impair sensor accuracy because such bubbles would expand under hyperbaric conditions, causing a reduced contact area between the sensor electrode and the surrounding interstitial fluid. The noted difference in MARD between the hypobaric and hyperbaric tests supports this hypothesis. However, in our study the procedure with prewetted sensors did not affect the sensor accuracy.
CGM has been shown to reduce the incidence and duration of hypoglycemia 7,15 and to reduce the number of severe hypoglycemic episodes in subgroups of patients 5 as well as in individuals with well-regulated diabetes. 16 In persons with type 1 diabetes, especially those under intensive insulin treatment, hypoglycemia is common not only during daytime but also at night. 17 Studies show that physical activity is associated to an increased variability in glucose before, during, and after physical exercise. 18 CGM also reveals delayed nocturnal hypoglycemia after intermittent high-intensity exercise. 19 In spite of the differences found during the hypobaric and hyperbaric tests, the stability and level of accuracy, shown in our study, is of great importance because one of the main benefits would be to both identify and reduce the occurrence of hypoglycemia in hypo- and hyperbaric conditions. CGM has considerable potential to become a tool to detect but also prevent hypoglycemia during special circumstances such as when flying or diving. However, to ensure the value of CGM in these conditions, further studies are needed on type 1 diabetes subjects as well as during large changes in glucose levels at different pressure conditions.
Footnotes
Acknowledgments
This work was supported by unrestricted grants from Medtronic and a grant from the Center of Clinical Research at the County Council of Värmland, Sweden. The skillful technical assistance of Joakim Trogen, M.D., at the Hyperbaric Medicine Unit at Sahlgrenska University Hospital and Peter Kronlund at the Hyperbaric Medicine Unit at Karolinska University Hospital, Stockholm, Sweden, is gratefully acknowledged. We also acknowledge the skillful assistance of Raghavendhar Gautham, M.S., Medtronic Diabetes (Sensor R&D), Northridge, CA.
Author Disclosure Statement
K.C. is an employee of Medtronic. No competing financial interests exist for the other authors.