
Abstract
Objective:
This study compare the effect of various liquid diets on 24-h glycemic variability in diabetes patients on tube feeding.
Patients and Methods:
The study included type 2 diabetes patients in whom percutaneous endoscopic gastrostomy had been performed for dysphagia as a sequela of cerebrovascular disease and who had been put on tube feeding with a standard high-carbohydrate liquid diet (HCD). Once stable glycemic control was achieved, these patients were continuously monitored for glucose levels for 5 days on continuous glucose monitoring. Of the 14 patients included, seven were given HCD on day 1, a low-carbohydrate/high-monounsaturated fatty acid liquid diet (LCD) on Days 2 and 3, and a isoleucine-containing liquid diet (ICD), which is known to promote glycemic uptake by skeletal muscle, thus suppressing increases in glucose levels, on Days 4 and 5, with the remaining seven given the same diets but ICD given on Days 2 and 3 and LCD given on Days 4 and 5. All comparisons were made under the same caloric conditions (caloric intake, 800–1200 kcal/day).
Results:
The 24-h mean glucose level was significantly lower with LCD and ICD than with HCD but was also significantly lower with LCD than with ICD. On the other hand, the SD of 288 glucose levels over a 24-h period, 24-h total area for glycemic fluctuations, and mean amplitude of glycemic excursion were significantly lower with LCD than with HCD or ICD, whereas they did not differ significantly between HCD and ICD.
Conclusions:
LCD and ICD led to significant decreases in mean glucose levels, compared with HCD. However, of the diets compared, LCD had the greatest effect on glycemic variability in these patients on tube feeding.
Introduction
Various liquid diets are currently available or in development to suppress postprandial glucose increases in diabetes patients on tube feeding. These include products rich in dietary fiber, those containing carbohydrates (CHOs) known to be slowly digested and absorbed, or low-CHO/high-monounsaturated fatty acid (MUFA) diets characterized by a low-CHO and a high-lipid blend ratio. 1 –3 All of these are associated with a low glycemic index, but the low-CHO/high-MUFA diets contain smaller amounts of CHOs and thus are associated with a low glycemic load.
In recent years, research evidence is emerging to show that isoleucine (Iso), a branched-chain amino acid, suppresses postprandial glucose increases, 4,5 and this has led to products containing Iso at 0.5 g/100 mL being developed, 6,7 while their effects on postprandial glycemic variability remain to be unclarified in detail.
In this study, type 2 diabetes patients who had undergone percutaneous endoscopic gastrostomy (PEG) for dysphagia as a sequela of cerebrovascular disease and had been put on tube feeding were given three kinds of liquid diet—a standard high-CHO (55–60%) diet (HCD), an Iso (46%)-containing diet (ICD), and a low-CHO (32%)/high-MUFA diet (LCD)—to monitor glycemic variability in these patients over a 24-h period by continuous glucose monitoring (CGM).
Patients and Methods
Patients
This was a prospective, non-blinded, crossover study. The study was performed in accordance with the ethical principles of the Declaration of Helsinki; all patients or their families were fully informed about the proposed study by the investigators, and the study was implemented after the subjects gave written informed consent to participate in it. The present study included a total of 14 type 2 diabetes patients who had undergone PEG for dysphagia after cerebrovascular disease and in whom stable glycemic control had been achieved with HCD (PN-Hi [Morinaga, Tokyo, Japan] or Meibalance [Meiji Milk, Tokyo]). Patients were excluded from the study if they had a glycosylated hemoglobin (HbA1c) value of 8.0% or greater, had had their treatment for diabetes changed, or had undergone a clinically relevant change in their health status within 1 month before the start of the study.
Study design
Of the 14 patients included (Table 1), seven were given HCD on Day 1, LCD (Glucerna®-EX; Abbott Japan, Tokyo) on Days 2 and 3, and ICD on Days 4 and 5, with the remaining seven given the same diets but ICD given on Days 2 and 3 and LCD given on Days 4 and 5 (Fig. 1). The total amount of energy to be given by tube feeding was set at 800–1200 kcal/day (approximately 25 kcal of body weight/day), and the patients were fed with three divided portions each day, with each portion being given over a 2-h period. The amount of Iso given through ICD was calculated as 4–6 g/day. The composition of each liquid diet used is shown in Table 2. The amount of energy given and the dosing schedule were not altered during the CGM study.
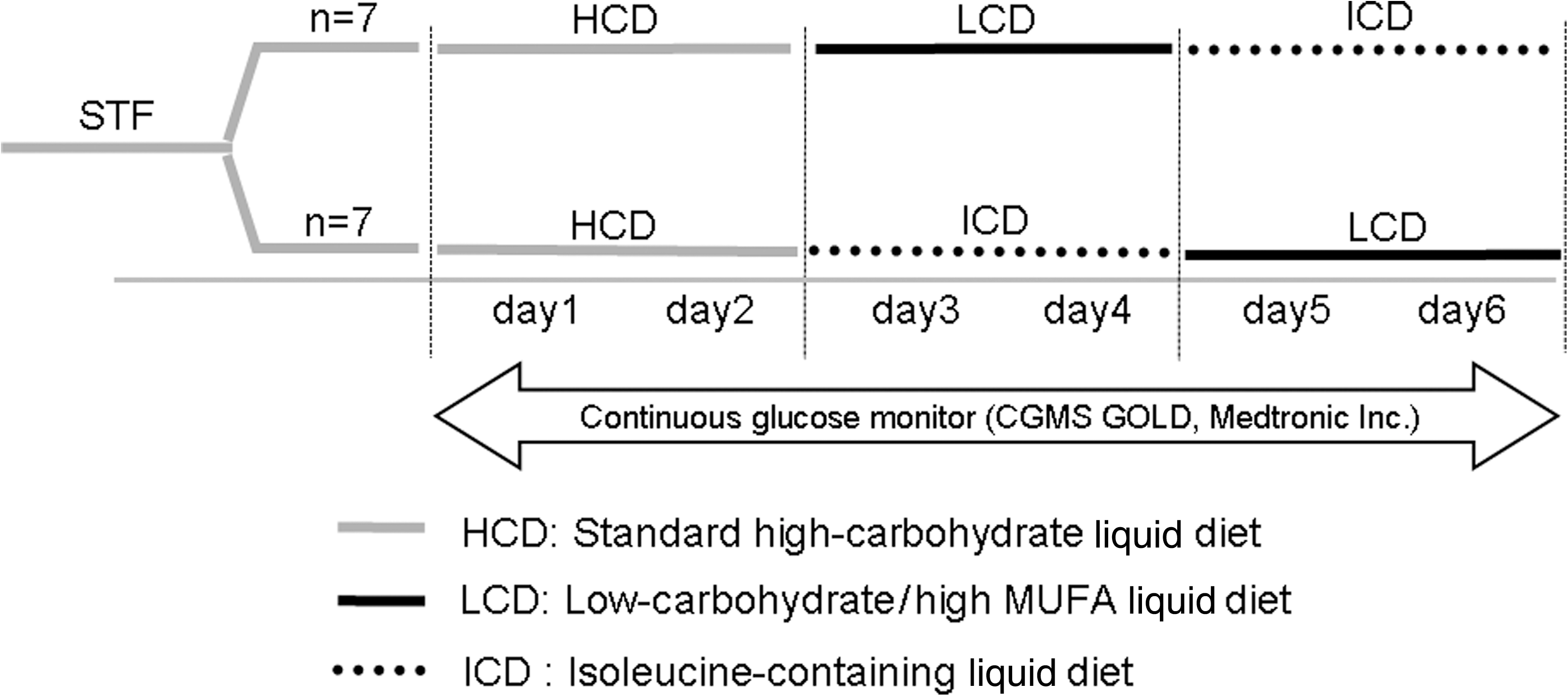
Study design. MUFA, monounsaturated fatty acid.
1,5-AG, 1,5-anhydroglucitol; BMI, body mass index; HbA1c, glycosylated hemoglobin; JDS, Japanese Diabetes Society.
MUFA, monounsaturated fatty acid.
CGMS® System Gold™ (Medtronic, Northridge, CA) was used for CGM, as it allows monitoring of glucose concentrations every 10 s as well as calculation of mean glucose levels every 5 min through its sensor put in place in the subcutaneous adipose tissue. Based on CGM data, the following parameters were assessed: 24-h mean glucose levels, SD values of 288 glucose levels measured over a 24-h period, total area for glycemic fluctuations (defined as the total area between the individual mean 24-h blood glucose level and the continuous blood glucose curve), mean amplitude of glucose excursion (MAGE), 8 proportion of time in hyperglycemia (>140 mg/dL), and proportion of time in hypoglycemia (<70 mg/dL). The total area for glycemic fluctuations and MAGE were calculated as previously described. 9,10
Statistical analysis
Statistical analyses were performed using SAS version 9.1 (SAS Institute, Cary, NC). Comparisons were made among HCD, LCD, and ICD using the Wilcoxon signed-rank test. A P value of <0.05 was considered to indicate statistical significance.
Results
Our present study demonstrated that the 24-h mean glucose levels as assessed by CGM were significantly lower with LCD and ICD than with HCD but was also significantly lower with LCD than with ICD (Table 3). Additionally, the SD values of 288 glucose levels measured over a 24-h period, as an index for glycemic variability in the patients, were found to be significantly lower with LCD than with HCD or ICD, whereas they did not significantly differ between HCD and ICD (Table 3). Again, the total area for glycemic fluctuations as an indicator of the range of glycemic fluctuations and MAGE were also found to be significantly lower with LCD than with HCD or ICD, but they did not significantly differ between HCD and ICD (Table 3).
P<0.05, ** P<0.01, versus standard high-carbohydrate liquid diet; † P<0.01, versus isoleucine-containing liquid diet.
MAGE, mean amplitude of glycemic excursion; MUFA, monounsaturated fatty acid.
LCD was associated with a significantly smaller proportion of time in hyperglycemia (>140 mg/dL) than HCD or ICD, but there was no significant difference observed between LCD and HCD or ICD with regard to the proportion of time in hypoglycemia (<70 mg/dL) (Table 3).
A case in point here that may help illustrate typical changes in diurnal glucose levels that result from switching from HCD to LCD or ICD is an 85-year-old woman who underwent PEG for dysphagia as a sequela of cerebrovascular disease and who is currently being tube-fed and treated with insulin therapy (insulin isophane [Novolin® N, Novo Nordisk Pharma, Bagsvaerd, Denmark], 4 units before breakfast): she exhibited wide diurnal glucose fluctuations with HCD, often oscillating between hyperglycemic (>140 mg/dL) and hypoglycemic (<70 mg/dL) states, then smaller diurnal glucose fluctuations and MAGE with LCD, and, again, wide glucose fluctuations and increases in MAGE with ICD (Fig. 2).
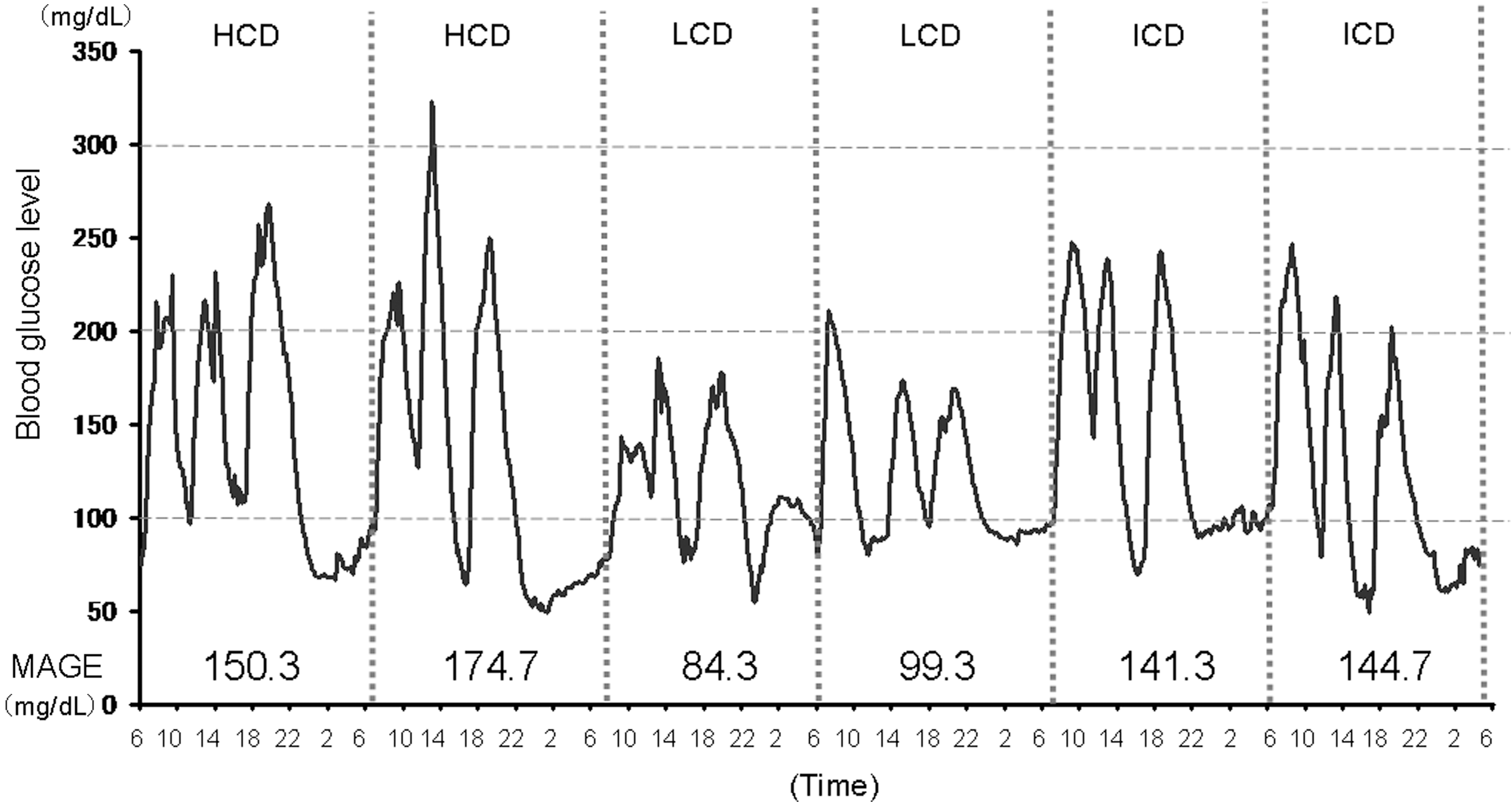
The 24-h glycemic fluctuations in an 85-year-old woman with type 2 diabetes on tube feeding who was fed standard high-carbohydrate liquid diet (HCD), low-carbohydrate/high-monounsaturated fatty acid liquid diet (LCD), or isoleucine-containing liquid diet (ICD) three times daily to provide a total energy intake of 1,200 kcal/day. MAGE, mean amplitude of glycemic excursion.
Discussion
Dysphagia as a sequela of cerebrovascular disease often leads to the need for PEG in affected patients who are often found to have diabetes as an underlying disease. Tube feeding for these patients entails not only required nutritional supply but also glycemic management aimed at prevention of tube feeding-associated complications. In diabetes patients being tube-fed, acute increases in postprandial glucose levels and reactive hypoglycemia associated with excessive insulin secretion that occur immediately after feeding are of particular note, as they contribute to wide diurnal glucose fluctuations. Indeed, in this study, an in-depth CGM-based examination revealed that a majority of patients with relatively favorable glycemic control as assessed by their HbA1c levels are associated with wide glucose fluctuations during a 24-h period, suggesting that a majority of tube-fed diabetes patients may also be found to be often oscillating between hyperglycemic and hypoglycemic states. Of note with regard to hypoglycemic episodes is that the decreases in glucose levels in tube-fed patients were shown to be such that they could lead to symptomatic hypoglycemic episodes in non–tube-fed diabetes patients, thus calling for therapeutic intervention. It is also reported that hypoglycemia could be a cause of death by causing increases in sympathetic tone in affected patients, 11 suggesting that reactive hypoglycemia secondary to acute increases in postprandial glucose levels after intake of liquid diets could adversely affect the cardiovascular system in these patients. Again, given that the higher the glucose peaks become, the more conspicuous the “reactive hypoglycemia” becomes, dampening acute postprandial glucose increases after tube feeding may help prevent further hypoglycemic episodes in tube-fed diabetes patients.
The International Diabetes Federation guidelines for the management of postprandial glucose levels 12 recommend the use of low-glycemic load (<10) foods as useful in controlling postprandial glucose levels but provide no specific guidance on tube feeding. Again, today, when CGM-based 24-h glucose monitoring is still not widely available, it is hardly feasible to change nutritional therapy or medications to address glycemic fluctuations over a 24-h period in tube-fed patients with diabetes. Our study results clearly demonstrated that LCD as a low-glycemic index/glycemic load meal not only decreased 24-h mean glucose levels but also potently narrowed the range of glycemic fluctuations in tube-fed patients with diabetes. Of note is that the long-term usefulness of LCD as a solid diet has been reported in a 1-year follow-up study of obese, type 2 diabetes patients, 13 but no long-term follow-up data on LCD as a liquid diet have been reported.
Iso, which formed part of the ICD examined in this study, has been reported to suppress postprandial glucose increases in humans in an earlier study 7 —with the caveat that the study involved a small number of subjects. It also remains unclear how ICD as a liquid diet may contribute to postprandial glycemic control, compared with conventional liquid diets. Iso has been shown in animal studies 5,6 to dampen postprandial glucose increases, as well as to suppress increases in HbA1c levels over the long term, where the mechanisms involved have been accounted for in terms of Iso's inhibitory effects on gluconeogenesis in the liver, in addition to its contribution to increases in skeletal muscle glucose uptake and systemic oxidative utilization of glucose. 14 However, our study results showed that the glucose levels in tube-fed patients with diabetes were greatly affected by the amount of CHOs given through tube feeding and by changing the blend ratio of CHOs in the liquid diet given, whereas Iso did not show clear clinical benefits in regard to glycemic control.
HCD, LCD, or ICD was given in this order in patients who had undergone PEG for dysphagia as a sequela of cerebrovascular disease and had been tube-fed with a standard HCD to compare their effects on diurnal glycemic fluctuations in these patients by CGM, which demonstrated significant decreases in any of the indices examined for magnitude of glycemic fluctuations (i.e., the SD of 288 glucose levels measured over a 24-h period, total area for the range of glycemic fluctuations, MAGE, and proportion of time in hyperglycemia [>140 mg/dL]) with LCD but no clear effects with Iso as part of the ICD examined on the range of glycemic fluctuations in patients given ICD. It is thus concluded that LCD (i.e., a liquid diet with a low-CHO blend ratio) may be the most efficacious of all diets examined in narrowing the range of glycemic fluctuations in diabetes patients on tube feeding.
Footnotes
Author Disclosure Statement
No competing financial interests exist.