
Abstract
Background:
The efficacy of automatic suspension of insulin delivery in induced hypoglycemia among subjects with type 1 diabetes was evaluated.
Subjects and Methods:
In this randomized crossover study, subjects used a sensor-augmented insulin pump system with a low glucose suspend (LGS) feature that automatically stops insulin delivery for 2 h following a sensor glucose (SG) value ≤70 mg/dL. Subjects fasted overnight and exercised until their plasma glucose (measured with the YSI 2300 STAT Plus™ glucose and lactate analyzer [YSI Life Sciences, Yellow Springs, OH]) value reached ≤85 mg/dL on different occasions separated by washout periods lasting 3–10 days. Exercise sessions were done with the LGS feature turned on (LGS-On) or with continued insulin delivery regardless of SG value (LGS-Off). The order of LGS-On and LGS-Off sessions was randomly assigned. YSI glucose data were used to compare the duration and severity of hypoglycemia from successful LGS-On and LGS-Off sessions and to estimate the risk of rebound hyperglycemia after pump suspension.
Results:
Fifty subjects attempted 134 sessions, 98 of which were successful. The mean±SD hypoglycemia duration was less during LGS-On than during LGS-Off sessions (138.5±76.68 vs. 170.7±75.91 min, P=0.006). During LGS-On compared with LGS-Off sessions, mean nadir YSI glucose was higher (59.5±5.72 vs. 57.6±5.69 mg/dL, P=0.015), as was mean end-observation YSI glucose (91.4±41.84 vs. 66.2±13.48 mg/dL, P<0.001). Most (53.2%) end-observation YSI glucose values in LGS-On sessions were in the 70–180 mg/dL range, and none was >250 mg/dL.
Conclusions:
Automatic suspension of insulin delivery significantly reduced the duration and severity of induced hypoglycemia without causing rebound hyperglycemia.
Introduction
The goal of adding the LGS feature to sensor-augmented pump therapy is to reduce the severity and duration of hypoglycemia, rather than to prevent it. In three published studies, experience with the system in children and adults has shown reductions in time spent in hypoglycemia and in its severity. The in-clinic ASPIRE (Automation to Simulate Pancreatic Insulin REsponse) study was undertaken to quantitatively determine the efficacy of the system's LGS feature combined with the Sof-Sensor® (Medtronic MiniMed, Inc.) glucose sensor in reducing severity and duration of hypoglycemia in a setting of carefully monitored exercise and is to be followed by the in-home ASPIRE study to determine the effectiveness and safety of this feature during routine usage.
Subjects and Methods
Subjects 17–58 years of age with type 1 diabetes for at least 1 year and at least 3 months of experience with a Medtronic insulin pump system were recruited. The research protocol was approved by the relevant Institutional Review Boards. Subjects≥18 years of age gave written informed consent; younger subjects gave written informed assent, and a parent or guardian provided written informed consent. A history of hypoglycemic seizure or hypoglycemic coma within the last 2 years was an exclusion criterion. The complete experimental design, statistical methods, and inclusion/exclusion criteria have been published separately. 2 In brief, subjects participated in exercise sessions with the pump's LGS feature set to suspend insulin delivery for 2 h once an SG value of ≤70 mg/dL was detected (LGS-On) or with the pump set to deliver basal insulin regardless of the SG value (LGS-Off). Sensors were inserted 24–72 h prior to hypoglycemic inductions. Sessions were separated by washout periods lasting 3–10 days. Upon successful completion of an LGS-On or an LGS-Off session, subjects crossed over to the opposite LGS setting for subsequent attempt(s). The order of the LGS-On and LGS-Off sessions was randomly assigned. Plasma glucose concentrations were measured with the YSI 2300 STAT Plus™ glucose and lactate analyzer (YSI Life Sciences, Yellow Springs, OH). Samples were drawn at 5–30-min intervals during the experiment and at 5–10-min intervals during periods of hypoglycemia (YSI value≤70 mg/dL). If necessary, glucose or insulin could be administered intravenously (or glucose orally) to treat subjects whose YSI glucose values reached <50 or >300 mg/dL, respectively; if those glucose levels were reached, the session was terminated. For each session, the protocol called for subjects to start exercise after an overnight fast with a YSI glucose value of between 100 and 140 mg/dL and to exercise until a YSI glucose value of ≤85 mg/dL was obtained. Experiments were delayed or rescheduled if plasma glucose values were not in the target range. No attempt was made to measure or standardize exercise intensity. Subjects were observed for up to 4 h once a YSI glucose value of <70 mg/dL was reached. For this study, hypoglycemia duration was the period of time during which YSI glucose values were <70 and >50 mg/dL, and hypoglycemia severity was defined as the nadir observed YSI glucose value. A successful session was defined as one with an observation period of 3–4 h without intervention and with YSI glucose levels ≥50 mg/dL. Subjects who discontinued a session because of low or high blood glucose values, who did not reach the target range, or who did not follow protocol procedures could repeat the session up to three times.
The primary end point was a comparison of the duration and severity of hypoglycemia measured with the YSI analyzer during successful LGS-On and LGS-Off sessions. Efficacy of the LGS feature was defined as a reduction in either duration or severity of hypoglycemia at the 0.0154 level of significance. The significance level for efficacy was determined by the observed intrasubject correlation after completion of the study and confirmed by polynomial imputation on missing YSI glucose values. The effect of the order of LGS-On and LGS-Off sessions was deemed significant for P≤0.1. If this order effect criterion was met, pre- and post-crossover sessions were to be analyzed separately. Secondary end points included sensor accuracy, YSI glucose values at the end of the 4-h session, and the number of times sessions were terminated for YSI glucose values <50 or >300 mg/dL.
Results
Fifty subjects (17–58 years old, 56% male) underwent a total of 134 sessions of induced hypoglycemia in order to have 98 successful sessions. Twenty-five subjects were randomized to have their first session with LGS-On, and 25 subjects to having their first session with LGS-Off. The mean and median observation times of successful experiments were 233 and 240 min, respectively. Subject characteristics are provided in Table 1. Details for attempted and failed sessions are given in Table 2.
A1C, glycosylated hemoglobin; BMI, body mass index; LGS, low glucose suspend.
One subject's reference YSI glucose level did not reach 70 mg/dL after three attempts, and one subject's reference YSI glucose level fell to below 50 mg/dL on each of three attempts. These two subjects had both previously completed a successful low glucose suspend (LGS)-Off session and refused to undergo further attempts.
Figure 1 shows examples of a successful LGS-On (Fig. 1A) and a successful LGS-Off session (Fig. 1B), including YSI and SG values, the 4-h observation period, and the 2-h pump suspension (Fig. 1A). Figure 2 depicts the mean (±SEM) YSI glucose values from all 98 successful sessions; time 0 represents the first YSI value ≤70 mg/dL. Shortly after time 0, the downward trend of YSI glucose values was reversed in LGS-On sessions (solid black line), and the mean YSI glucose value stayed in the euglycemic range after basal insulin delivery was resumed at 120 min until the end of the session. In successful LGS-Off sessions, where basal insulin delivery continued, the mean YSI glucose value remained in the hypoglycemic range during most of the observation period (dashed black line).

Data from one subject's successful
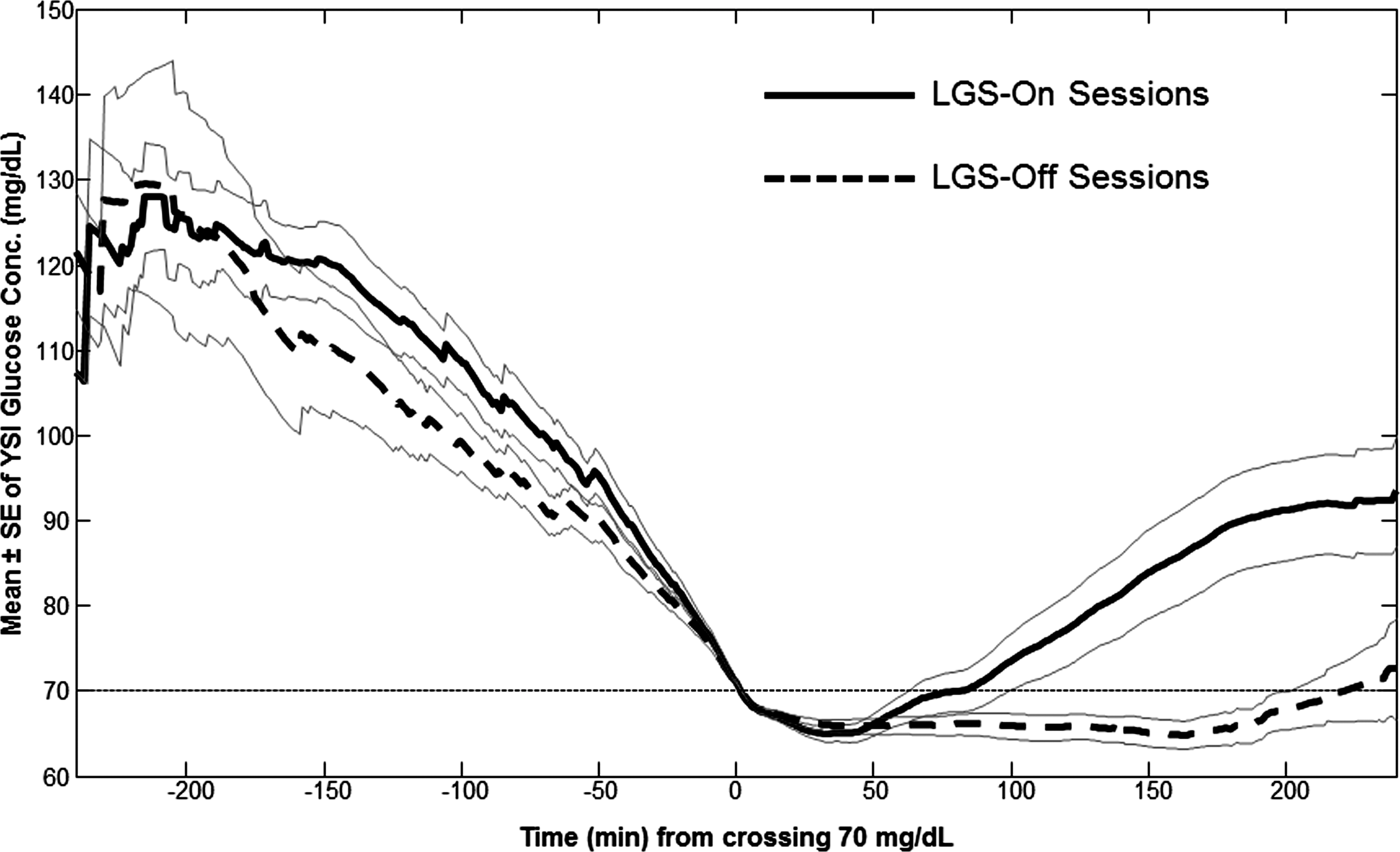
Reference YSI values for all 98 successful sessions. Tracings are centered at the time when the YSI glucose value fell below 70 mg/dL. Solid black line represents the mean of low glucose suspend (LGS)-On sessions, the dashed black line represents the mean of LGS-Off, and the gray lines represent mean±SEM values.
When all 98 successful sessions were analyzed, the mean duration of hypoglycemia was 32.2 min shorter in LGS-On than in LGS-Off sessions (mean±SD, 138.5±76.68 vs. 170.7±75.91 min, P=0.006), representing a 19% reduction. The mean nadir YSI glucose value was modestly higher during LGS-On compared with LGS-Off sessions (59.5±5.72 vs. 57.6±5.69 mg/dL, P=0.015), confirming that use of the LGS feature reduced the severity of induced hypoglycemia.
An order effect was seen for the duration of hypoglycemia in LGS-On experiments but not in LGS-Off experiments (P=0.051), thus allowing for separate analyses of pre- and post-crossover sessions. When the 50 successful pre-crossover sessions were considered separately, the mean hypoglycemia duration was 65.8 min shorter in LGS-On sessions than in LGS-Off sessions (107.8±71.24 vs. 173.6±71.17 min, P=0.001), representing a 38% reduction. When the 48 successful post-crossover sessions were considered separately, the mean hypoglycemia durations were not significantly different in LGS-On and LGS-Off sessions (171.5±67.00 vs. 167.7±81.75 min, P=0.432). The order of the LGS-On and LGS-Off sessions did not have a significant effect on the severity of hypoglycemia (P=0.134).
At the end of the observation period, the mean YSI glucose value was higher after LGS-On than after LGS-Off sessions (91.4±41.84 vs. 66.2±13.48 mg/dL, P<0.001). Most (53.2%) YSI glucose values at the end of LGS-On sessions were in the 70–180 mg/dL range, whereas 70.7% of YSI glucose values at the end of LGS-Off sessions were <70 mg/dL. The highest end-observation values were 245 and 109.5 mg/dL following LGS-On and LGS-Off sessions, respectively.
There was good agreement between SG and YSI values in the 40–70 mg/dL range, with mean and median absolute difference values of 12.0±8.6 mg/dL and 11.2 mg/dL, respectively. The mean and median bias values in this glucose range were 6.3±13.3 mg/dL and 7.7 mg/dL, respectively.
Discussion
Although an ultimate goal of effective diabetes management is prevention of hypoglycemia, strategies that reduce its duration and/or severity are desired because of the many short- and potential long-term adverse consequences associated with severe hypoglycemia. The LGS feature was designed to mimic physiology by stopping insulin delivery when a hypoglycemic threshold is reached. The 2-h time frame of pump suspension was designed to minimize rebound hyperglycemia. From this study, both appear to have been achieved. Although the present study showed a benefit of the LGS feature in reducing induced hypoglycemia in a relatively controlled setting, the feature may also help reduce hypoglycemia duration and severity at any time, and particularly at night when 2-h LGS events are most frequently seen. 3 –5 Therefore, LGS may help to prevent nocturnal seizures that appear to result from protracted (2.25–4-h) nocturnal hypoglycemia, as recently reported. 6
The study's rigorous protocol and narrowly defined target of hypoglycemia (50–70 mg/dL) may limit the generalizability of its results. In particular, the attenuation of hypoglycemia reported here may not be representative of the effects of the LGS feature when used in a real-world setting. Because we did not analyze data from sessions in which subjects' YSI glucose values fell to ≤50 mg/dL, our estimate of the beneficial effects of pump suspension on the severity of induced hypoglycemia is likely to be a conservative one. No attempt was made to measure or control for subjects' varying levels of physical fitness or the intensity of exercise. The modest reduction in hypoglycemia severity (approximately 2 mg/dL) in LGS-On sessions, while statistically significant, is of uncertain clinical significance. The number of failed and repeated sessions attests to the difficulty of inducing and maintaining hypoglycemia for extended periods of time.
A strength of the ASPIRE study was its use of a reference instrument for frequent plasma glucose determinations, allowing independent quantification of hypoglycemia. The ASPIRE study also used a single hypoglycemic threshold and a single length of pump suspension for all LGS events. This is in contrast to other studies, where analyses were done on convenience samples of SG readings that were then used to estimate the impact of the LGS feature or where subjects were free to change the pump's LGS settings.
A recent study of 21 children and adolescents compared the frequency of hypoglycemic episodes during 2 weeks without the LGS feature and 6 weeks with the LGS feature programmed to alert users to SG values <75 mg/dL and suspend insulin at SG values <70 mg/dL. Use of the LGS feature in this manner reduced the number of hypoglycemic excursions (to ≤40 mg/dL) by more than half (P=0.005) and reduced the time spent in hypoglycemia <70 mg/dL by 43 min/day (P=0.002) without significantly increasing the mean glucose value (P=0.30). 5 Another retrospective study of almost 50,000 patient-days of system use from 935 patients compared uploaded data from LGS-On and LGS-Off intervals. By interrogating the CareLink® database (Medtronic MiniMed, Inc.) of voluntarily uploaded and anonymized insulin pump and continuous glucose monitoring (CGM) data, it was found that the LGS feature was turned on for 82% of the observed patient-days and significantly reduced exposure to hypoglycemia compared with days when the LGS feature was turned off. Use of the LGS feature was also associated with a decrease in the percentage of SG readings >240 mg/dL (P=0.02) and >300 mg/dL (P<0.01). 3 A third study of 31 adults evaluated the efficacy and acceptability of the system. A reduction in nocturnal hypoglycemia in those at greatest risk was noted. All the subjects found the LGS feature “useful,” and 93% of the subjects wanted to continue using it at the end of the study. 4
We observed that the duration of hypoglycemia was much longer among subjects who had previously undergone a hypoglycemic induction session, consistent with the notion that “hypoglycemia begets hypoglycemia.” 7 Patients with a history of hypoglycemic seizure or coma in the 2 years prior to enrollment were excluded. The effect may be related to depletion of glycogen stores or an impaired counterregulatory hormone response that had not fully recovered in the 3–10-day washout period. 8 Because counterregulatory hormone levels were not measured during this study, washout periods were not uniform, and some subjects had multiple hypoglycemic inductions, it is not possible to assess the reason(s) for the order effect. The recovery of the autonomic response to hypoglycemia has been shown to occur with use of CGM for 4 weeks. 9 The addition of an automatic LGS feature to the insulin pump/CGM system may further improve autonomic recovery and mitigate hypoglycemia to an even greater extent.
Results of this study provide evidence that the LGS feature, when programmed to suspend insulin delivery for 2 h when an SG value of ≤70 mg/dL is detected, can significantly reduce the duration and severity of hypoglycemia without causing significant rebound hyperglycemia.
Footnotes
Acknowledgments
Medtronic, Inc. (Northridge, CA) funded the study and supplied the insulin pump systems used in the study. We thank Scott W. Lee, M.D., Thomas Troub, and Kathy Beaver, R.N., employees of Medtronic, who provided comments on an earlier draft of the manuscript and coordinated data analysis at the authors' request.
Author Disclosure Statement
S.G., R.L.B., T.S.B., B.A.B., R.H.S., and D.C.K. have received research support and/or travel support and/or serve on advisory boards from or for Medtronic. J.S., J.B.W., and F.R.K. are employees of Medtronic, Inc. No other potential conflicts of interest relevant to this article were reported.