
Abstract
Aim:
This study evaluated the effect of sitagliptin versus glibenclamide on arterial stiffness, blood pressure, lipid profile, oxidative stress, and high-sensitivity C-reactive protein (hsCRP) in type 2 diabetes mellitus patients.
Subjects and Methods:
Forty diabetes patients, inadequately controlled on metformin, were randomly assigned to either sitagliptin (100 mg/day) or glibenclamide (5 mg/day) for 3 months. Following a 1-month washout period, a crossover switch from glibenclamide to sitagliptin and vice versa was performed for an additional 3 months. Arterial stiffness, 24-h ambulatory blood pressure monitoring, lipids, hsCRP, glycated hemoglobin, fasting glucose, STAT-8-isoprostane (a measure of oxidative stress), body mass index (BMI), and waist circumference were measured at baseline and at 3 months with each of the study drugs.
Results:
Thirty-four patients completed the study. Glibenclamide had a better glucose-lowering effect than sitagliptin, but this was associated with more hypoglycemic events. BMI increased following glibenclamide treatment, whereas sitagliptin proved weight-neutral. Mean BMI gain was +0.5±1.0 kg/m2 for glibenclamide versus −0.01±0.9 kg/m2 for sitagliptin (P<0.001). Triglyceride levels significantly dropped following sitagliptin, although they remained unaltered after glibenclamide treatment. Mean triglyceride decrease was −18.4±45 mg/mL after sitagliptin but −0.2±57 mg/dL following glibenclamide treatment (P=0.018). There was no change in low-density lipoprotein, high-density lipoprotein, arterial stiffness, blood pressure monitoring, hsCRP, or STAT-8-isoprostane with each of the study drugs.
Conclusions:
Sitagliptin, but not glibenclamide, demonstrated a significant beneficial effect on BMI and triglyceride levels. However, arterial stiffness, blood pressure, oxidative stress, and inflammatory status were not significantly affected by adding sitagliptin or glibenclamide to metformin-treated type 2 diabetes patients.
Introduction
Glucagon-like peptide-1 (GLP-1) stimulates insulin secretion and inhibits glucagon secretion and gastric emptying, thereby reducing postprandial glycemia. 4 GLP-1 is rapidly inactivated by the enzyme dipeptidyl peptidase-4 (DPP-4). Two classes of drugs with the potential to act via incretin receptor signaling have been approved: GLP-1 receptor agonists and DPP-4 inhibitors. Sitagliptin is a DDP-4 inhibitor administered either as monotherapy or in combination with other oral antidiabetes agents. 5
Accumulating data suggest beneficial effects of the incretin-based therapies on CVD and its risk factors. For example, a recent large-scale retrospective study demonstrated that patients with T2DM treated with a GLP-1 agonist, exenatide, are less likely to have a CVD event compared with those controlled by other hypoglycemic drugs. 6 Emerging data suggest a cardioprotective effect for DPP-4 inhibitors as well. 7
Hypertension, increased arterial stiffness, dyslipidemia, chronic inflammation, and oxidative stress are well-established risk factors for CVD. These pathologies are highly correlated with both obesity and diabetes. 8 Designing optimal treatment regimens for patients with T2DM and comorbidities requires an understanding of the risks and benefits of individual antidiabetes drugs.
Although some data suggesting the beneficial effects of GLP-1 agonists on hypertension dyslipidemia and CRP have been cited in the literature, 9 –14 few data exist regarding the effect of DPP-4 inhibitors on these risk factors. Similarly, little is known about the influence of GLP-1-based therapies on oxidative stress. Arterial stiffness is increasingly recognized as a surrogate end point for CVD. 15 Increased arterial stiffness associated with diabetes may partially explain the increased CVD risk observed in this condition. 16 Although GLP-1 receptor antagonists may have beneficial effects on endothelial function, 17,18 the effect of DPP-4 inhibitors on endothelial function has not yet been investigated.
Information regarding the effects of sulfonylurea drugs on cardiovascular risk factors is scanty. Nevertheless, based on the available information one may conclude that sulfonylureas, such as glibenclamide, have no appreciable effects on the major cardiovascular risk factors, such as systemic blood pressure, arterial stiffness, blood lipid levels, oxidative stress, and inflammatory status of diabetes patients. 19 –21
The aim of this study was to evaluate the effect of sitagliptin on cardiovascular risk factors such as arterial stiffness, 24-h blood pressure monitoring, lipids, STAT-8-isoprostane as a marker of oxidative stress, and high-sensitivity C-reactive protein (hsCRP) as a marker of inflammation in T2DM patients inadequately controlled on metformin monotherapy. In order to neutralize the glucose-lowering effect of sitagliptin, we compared sitagliptin treatment with glibenclamide treatment in a crossover fashion, assuming from the available literature that a sulfonylurea (specifically glibenclamide) has a neutral effect regarding these cardiovascular risk factors.
Subjects and Methods
Patients
Patients with T2DM 18–75 years of age with inadequate glycemic control (glycated hemoglobin [HbA1c] >7%) while on metformin treatment were recruited to the study.
Exclusion criteria included creatinine clearance <30 mL/min, a history of treatment with incretins or sulfonylurea during the last 3 months, treatment with nitrates, uncontrolled heart failure, uncontrolled hypertension, and/or any change in the hypertensive medications within 1 month prior to starting the study, malignancy, and pregnancy.
Medications other than those used as a part of the study remained unaltered throughout the study period. Because all patients remained stable during the follow-up period and because the study protocol was planned as a crossover design, each patient served as his or her own control.
The study protocol was approved by the Medical Center's Helsinki Committee for Experiments in Humans. All patients provided written informed consent.
Study design
The study has been designed as a single-center, prospective, randomized, controlled, open labeled, crossover trial. Eligible patients were randomly assigned on a 1:1 ratio to receive either sitagliptin (100 mg) (Merck Sharp & Dohme Ltd., Tel Aviv, Israel) once daily or glibenclamide (5 mg) (Dexcel Pharma Ltd., Or Akiva, Israel) once daily, titrated as needed (to reach fasting blood glucose levels between 100 and 150 mg/dL). The randomization was achieved by applying the following recruitment order: the first patient started with glibenclamide for 3 consecutive months and then was switched to sitagliptin as will be described, the next patient started with sitagliptin and then was switched to glibenclamide, and so on. The first follow-up period lasted 3 months. At the end of 3 months, all patients were subjected to a 1-month washout period, receiving neither sitagliptin nor glibenclamide. At the end of the washout period, the patients treated with sitagliptin were switched to glibenclamide, whereas those on glibenclamide were switched to sitagliptin for 3 additional months (the second follow-up period).
The study design is presented in Figure 1. The follow-up period lasted for 28 consecutive weeks and included the patient's visits at 0, 12, and 28 weeks. During each visit, the patient's history was recorded, weight, height, and waist circumference were measured, and blood samples were obtained for HbA1c, fasting glucose, lipids, hsCRP, and STAT-8-isoprostane estimation. Blood for STAT-8-isoprostane determination was collected in EDTA-pretreated test tubes, and the measurements were performed using a specific competitive human enzyme-linked immunosorbent assay (Cayman Chemical Co., Ann Arbor, MI), according to the manufacturer's instructions. In addition, the patient's arterial stiffness was assessed, and 24-h blood pressure fluctuations were monitored. A follow-up call for recording any adverse events and for titrating the glibenclamide dosage was performed by the principal investigator every 2 weeks throughout the entire study period.
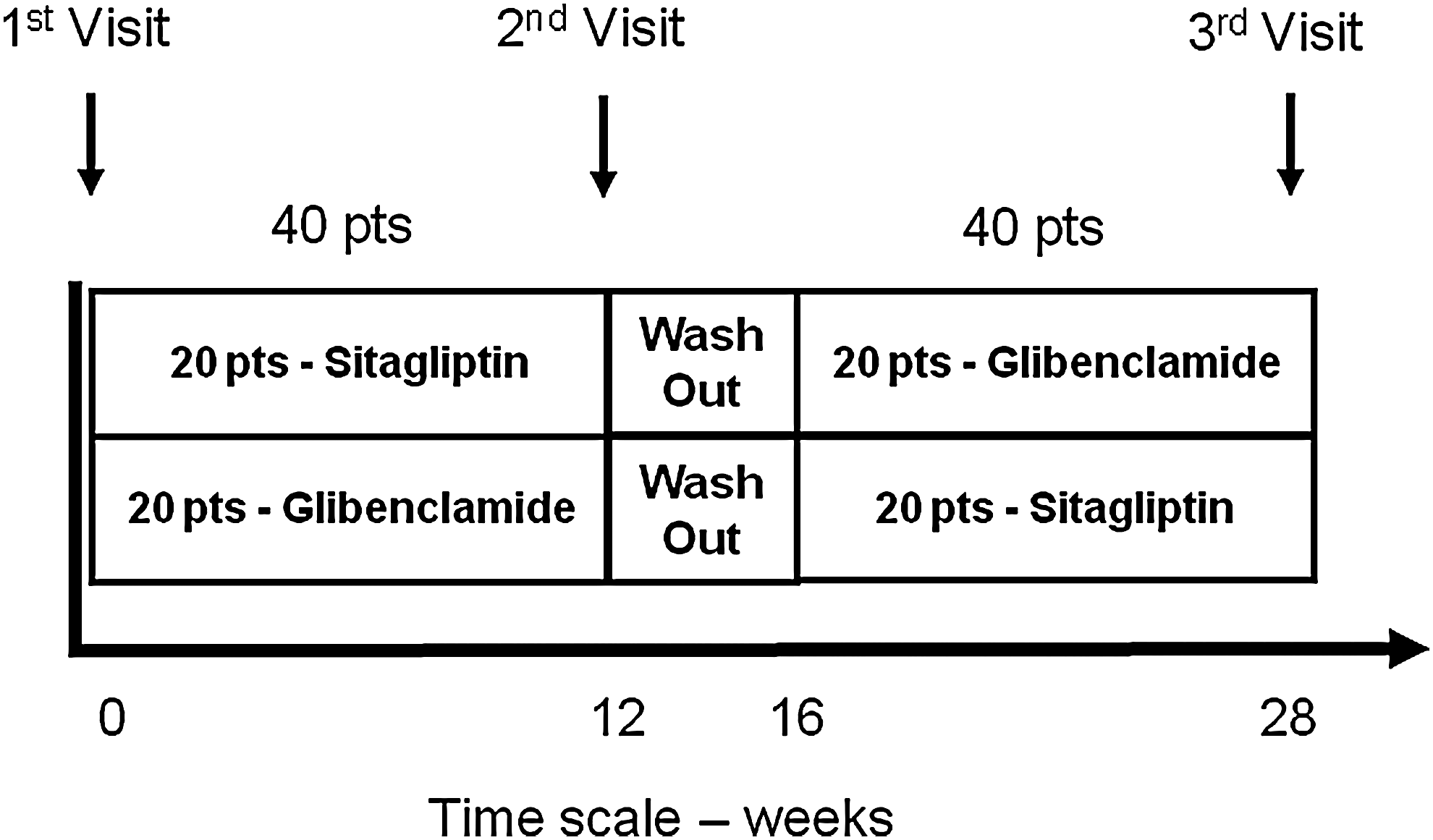
Crossover study design. pts, patients.
Arterial stiffness
Assessment of arterial stiffness was performed by a noninvasive technique using the commercially available SphygmoCor system (AtCor Medical, West Ryde, NSW, Australia). All measurements were performed in the morning after an overnight fast (8–10 h) and after a short rest period, while the patient was in a recumbent position at a room temperature of 25°C. Peripheral pressure waveforms were recorded from the radial artery at the wrist, using applanation tonometry with a high-fidelity micromanometer (Millar Instruments, Houston, TX). When 20 sequential waveforms were recorded, a validated 16–18 generalized transfer function was applied to generate the corresponding central aortic pressure waveform. The augmentation index (AIX) and augmented pressure were derived by calculation, using the pulse-wave analysis technique. 22
The augmentation of central arterial pressure is the difference between the first and second systolic peaks of the central pressure waveforms, and the central AIX is the augmentation expressed as a percentage of the pulse pressure.
Statistical analysis
Statistical analysis was performed using the statistical software SPSS version 15 (SPSS, Inc., Chicago, IL). Parametric data (waist circumference, body mass index [BMI], lipids, hsCRP, HbA1c, fasting glucose, blood pressure, and AIX) were expressed as the mean difference from baseline±SDs and compared by paired t test. Nonparametric data (sex, duration of diabetes, etc.) were expressed as absolute numbers and percentiles and compared using Fisher's exact test. Differences between the results yielding P values <0.05 were considered statistically significant.
Results
Of the 40 patients enrolled into the study, six discontinued in the second follow-up period. One patient was diagnosed with sarcoidosis and was put on corticosteroids, two patients suffered dizziness that was attributed to the study medication, and three patients were lost to follow-up. Consequently, 34 patients completed the study.
Baseline patient characteristics are summarized in Table 1. The majority of patients were males, with a mean age of 59 years. The average duration of diabetes mellitus was 7.8 years. Three patients had nephropathy (7.5%), two patients had retinopathy (5%), and five patients had neuropathy (12.5%). The mean BMI was 31 kg/m2, and average HbA1c was 8.3%. The majority of patients had CVD or several risk factors for CVD.
ACE, angiotensin-converting enzyme; AT2, angiotensin II; BMI, body mass index; CAD, coronary artery disease; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein, hsCRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein.
After titration the mean glibenclamide dose during the study was 4 mg/day, whereas the sitagliptin dose was fixed at 100 mg/day. Glibenclamide had a better glucose-lowering effect than sitagliptin (Fig. 2). Adjusted mean change in HbA1c from baseline at the end of 12 weeks of treatment was −1.0±1.1% (SEM±0.19%) with glibenclamide and −0.6±1.1% with sitagliptin (SEM±0.19%) (P=0.01). The mean change for fasting glucose was −31±36 mg/dL (SEM±6.17%) and −13±51 mg/dL (SEM±5.83 mg/dL) for glibenclamide and sitagliptin, respectively (P=0.02).

The overall incidence of hypoglycemia was significantly higher in the glibenclamide treatment period compared with the sitagliptin treatment period. Fourteen patients (37%) reported at least one event of hypoglycemia during the glibenclamide treatment period compared with one report (2.6%) of hypoglycemia with sitagliptin. No severe hypoglycemia (necessitating intervention) occurred in any patient throughout the study. Other adverse effects were rare. Two patients (one in each treatment period) discontinued the study because of dizziness.
At the end of 12 weeks, sitagliptin treatment was associated with modest weight reduction, and glibenclamide was associated with increased weight. The mean change of BMI from baseline was −0.01±0.9 kg/m2 and +0.5±1.0 kg/m2 in the sitagliptin and glibenclamide treatment periods, respectively (P<0.001. The mean change of weight from baseline was −0.2±2 kg for sitagliptin and +1.2±2.3 kg for glibenclamide (P=0.007). An insignificant decrease in waist circumference was recorded at the end of the sitagliptin period compared with glibenclamide (−0.8±3.5 cm and +0.3±3.8 cm, respectively; P=0.064).
The mean deviation of triglycerides (TGs) from baseline was significantly greater at the end of the sitagliptin treatment period compared with glibenclamide (−18.4±45 mg/dL and −0.2±57 mg/dL, respectively; P=0.018). There was no change in low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), or hsCRP levels at the end of both treatment periods. There was no change from baseline regarding STAT-8-isoprostane at the end of the two treatment periods compared with baseline (Table 2).
HDL, high-density lipoprotein; hsCRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein.
The effect of treatment on arterial stiffness and blood pressure are summarized in Table 3. Data for arterial stiffness are presented for only 16 patients because of technical problems with the software. There was no change from baseline regarding arterial stiffness at the end of the two treatment periods compared with baseline. There was a small decrease in systolic and diastolic blood pressure during the study period with no difference between the two treatment periods (systolic pressure, −2.5±9.5 mm Hg for glibenclamide and −3.4±7.5 mm Hg for sitagliptin, P=0.648; diastolic pressure, −1±7.4 mm Hg for glibenclamide and −0.46±7.4 mm Hg for sitagliptin, P=0.671).
Data for augmentation index and augmentation index percentage are presented for 16 patients only.
Discussion
There is a rapid global increase in the rates of T2DM and its associated detrimental cardiovascular effects. 1
The relatively new incretin-based therapies include the degradation-resistant GLP-1 agonists and the inhibitors of DPP-4 activity. Accumulating data from both animal and human studies suggest a beneficial effect of GLP-1 and its metabolites on myocardium, endothelium, and vasculature. 23 However, in this study, we found that sitagliptin, a DPP-4 inhibitor, had no beneficial effect, nor did glibenclamide, regarding arterial stiffness, blood pressure, oxidative stress, and inflammation in inadequately controlled T2DM patients on metformin.
In accord with results from previous studies, glibenclamide was found to be more efficient in reducing HbA1c and fasting glucose and caused more hypoglycemic events compared with sitagliptin. 24
Glibenclamide therapy resulted in BMI increase, whereas sitagliptin treatment brought about a modest weight reduction. The differences in BMI gain (glibenclamide therapy) as well as in weight loss (sitagliptin treatment) between the two treatment periods were found to be significantly different. Treatment with sitagliptin also demonstrated a tendency toward decreasing the patients' waist circumference. These results are compatible with the previously published data in which sulfonylureas have been shown to cause weight gain, 8 whereas DPP-4 inhibitors have been demonstrated to exert positive effects with respect to the weight profile 25 : in a recently published study, 52 weeks of treatment with glipizide brought about weight gain (mean change from the baseline +1.1 kg) compared with substantial weight loss achieved by treatment with sitagliptin (change from baseline −1.5 kg). 26 In yet another study, vildagliptin, a different DPP-4 inhibitor, was found to be weight neutral. 27
With respect to the lipid profile, sitagliptin therapy resulted in significant decrease in TG levels compared with glibenclamide. However, neither medication had any significant effects on LDL-C and HDL-C. Different drugs from the incretin family have been shown to have a beneficial effect on lipid profile: three placebo controlled trials examined the effect of exenatide (a GLP-1 agonist) on lipid parameters in patients either on metformin alone, on sulfonylurea alone, or on metformin plus sulfonylurea; at 30 weeks no significant differences were observed for either the exenatide group or placebo in terms of total cholesterol, LDL-C, TG, or HDL-C. 28 –30 Nevertheless, in an open-labeled 82-week extension of these studies, exenatide treatment led to significant improvements in HDL-C and TG. 31 Significant reductions in TG and total cholesterol have also been reported retrospectively for exenatide. 12,13 Liraglutide, another GLP-1 agonist, has been associated with a significant reduction in TG levels with no change in LDL-C and HDL-C. 11 When added to metformin, sitagliptin (100 mg/day) provided generally small but significant decreases in total cholesterol, TGs, non–HDL-C, and the TG-to-HDL ratio. 32 Reported effects of vildagliptin on lipid parameters include decreased TG levels and increased HDL-C levels. 22
The effect of sulfonylureas on lipid parameter is not known. 8
The most common pattern of dyslipidemia in T2DM patients is elevated TG levels and decreased HDL-C levels. This pattern may be a treatable risk factor for subsequent CVD. Although intensive lifestyle modification remains the gold standard, an antidiabetes drug that can modulate this lipid pattern would be beneficial. Our observation that sitagliptin has the potential to improve the alarming pattern of dyslipidemia in diabetes might therefore be of clinical importance.
It is well documented that diabetes is associated with endothelial dysfunction and increased arterial stiffness. 33,34 GLP-1 receptor expression has been detected on endothelial and vascular smooth muscle cells. 35 Previous animal studies have shown that GLP-1 can induce a nitric oxide-dependent or -independent relaxation of arteries. 36,37 Two small clinical studies found that GLP-1 infusion improved endothelial function. 17,18 Arterial stiffness can be described by distensibility and compliance coefficient, pulse-wave velocity, and wave reflection expressed as AIX. AIX measurements have been shown to predict coronary artery disease in whole populations as well as in patients with T2DM. 38,39 To the best of our knowledge, this is the first study to examine the effect of a DPP-4 inhibitor on AIX as an indicator of arterial stiffness and endothelial function. In the present study, by contrast to the previously published data suggesting a beneficial effect of GLP-1 analogs on arterial stiffness, neither glibenclamide nor sitagliptin demonstrated any positive effects on arterial stiffness. Similarly, both drugs had no significant effect on oxidative stress estimated by STAT-8-isoprostanes. Data from isolated mouse heart models show that GLP-1 (9–36), the metabolite of GLP-1 degradation by DPP-4, exerts a vasodilatory effect through a GLP-1 receptor–independent mechanism involving nitric oxide formation. 35 This might explain the diverse effects of GLP-1 analogs and DPP-4 inhibitors on the vascular bed.
Some large studies have shown a significant reduction in both systolic and diastolic blood pressure with different GLP-1 analogs. 9,10 Sitagliptin has been associated with small but significant reductions in 24-h ambulatory systolic and diastolic blood pressure compared with placebo in hypertensive patients without diabetes. 40 The main mechanism for this antihypertensive effect seems to be related to weight loss. In accordance with the latter, our cohort of T2DM patients demonstrated nonsignificant decreases in systolic and diastolic blood pressure, irrespective of the drug applied.
Inflammation plays an important role in the pathogenesis of atherosclerosis, and considerable evidence points to hsCRP as an independent predictor of future cardiovascular events. Liraglutide, a GLP-1 agonist, can reduce hsCRP levels in T2DM patients in a dose-dependent way. 14 Exenatide has been shown in a retrospective analysis to decrease C-reactive protein as well. 12 However, in the current study, as with endothelial function, neither sitagliptin nor glibenclamide had any significant effect on hsCRP.
The present study has several limitations, such as the relatively small number of participants, the limited follow-up period, the absence of data collection immediately after the washout period, and the lack of information on arterial stiffness in a significant number of patients.
In conclusion, sitagliptin administration was found to be associated with reduction in BMI and TG levels compared with treatment with glibenclamide in a T2DM patient cohort inadequately controlled by metformin prior to their enrollment in the present study. No additional beneficial effects were exerted by either sitagliptin or glibenclamide on the patients' lipid profile, inflammatory status, oxidative stress, arterial stiffness, or 24-h ambulatory blood pressure monitoring.
Footnotes
Acknowledgments
The authors wish to thank Vivienne York for her valuable editorial assistance.
Author Disclosure Statement
No competing financial interests exist.