
Abstract
Background:
About 70% of the patients operated on for a gastric bypass (Roux-en-Y gastric bypass [RYGB]) suffer from dumping syndrome. In these patients, previous studies have demonstrated a high glycemic variability with hypoglycemia and with altered continuous glucose monitoring (CGM) profiles. The aim of this study was to evaluate the effect of treatment with dietary counseling plus acarbose administration on the symptoms and on the characteristics of the CGM profile.
Subjects and Methods:
Eight consecutive patients with dumping syndrome were given dietary counseling for 6 weeks and also treated with acarbose (50–100 mg three times a day). Their symptoms and the features of the CGM were compared before and after treatment.
Results:
The symptoms disappeared in seven patients. There was a significant increase in the time to the interstitial glucose (IG) peak and a reduction in the rate of the IG increase after a meal and in the rate of the IG decrease following the peak. The time below 60 mg/dL was significantly decreased, and the minimal IG value was significantly increased. The maximum and mean IG levels and the time above 140 mg/dL were decreased, but not significantly. Six patients spent more than 1% of the time with IG values below 60 mg/dL before treatment, but after treatment this was reduced to one patient. Before treatment only one patient had an IG level neither below 60 or above 140 mg/dL, and after treatment four patients were in this category.
Conclusions:
Dietary counseling and acarbose treatment eliminated the symptoms and improved the CGM profile of patients suffering from dumping syndrome after RYGB.
Introduction
Less severe hypoglycemic episodes are associated with dumping syndrome as a series of symptoms occurring late after a meal. The dumping syndrome occurs after anastomosis of the small intestine to the gastric remnant of a gastrectomy. 7 Early symptoms are digestive and adrenergic (the classical dumping syndrome), whereas the late components comprise adrenergic and neuroglucopenic signs. 7 A recent study with continuous glucose monitoring (CGM) suggests that asymptomatic episodes of hypoglycemia might occur in 33–50% of patients after RYGB. 8
Most of the time the hypoglycemic episodes follow an early and transient hyperglycemic rise, sometimes higher than 200 mg/dL, although the patients are not known to have diabetes. 3,6,8 –11 A hyperinsulinemic response promotes a rapid decrease in glycemia. 12,13 This sequence of hyperglycemia/hyperinsulinemic response/hypoglycemia has been observed after oral glucose challenges and with CGM, 11 –13 suggesting that carbohydrates are digested and absorbed very rapidly after a meal. Hanaire et al. 12 have described the CGM profiles in these cases: they show a specific reduction in the time to the glycemic peak after a meal and increased glycemic variability.
The treatment of post-gastric bypass hypoglycemia is not well developed (see Ritz and Hanaire 6 for a detailed review). Acarbose is a drug that inhibits α-glucosidase, thus reducing the glycemic peaks after a meal, and it is used for the treatment of diabetes and for the symptoms of dumping syndrome. 14 –16 It was reported to be efficient in preventing hypoglycemia in four patients following gastric bypass. 4,13,17 Halperin et al. 8 reported eight cases of severe neuroglucopenia treated with acarbose and described the CGM features of the treated patients compared with asymptomatic patients, although the study was not designed to demonstrate the effectiveness of acarbose treatment.
The aim of the present pilot study was to report the results of the treatment of late dumping syndrome after gastric bypass with dietary counseling plus acarbose treatment in eight consecutive patients. It describes both the effects on the symptoms and on the characteristics of the CGM profile.
Patients and Methods
Eight consecutive patients suffering from late dumping symptoms 7 after a gastric bypass were enrolled. Insulinoma was excluded in these subjects before their participation. A treatment combining dietary counseling and 50–100 mg of acarbose three times a day before meals depending on the digestive tolerance was initiated. To reduce glycemic peaks, patients were instructed to avoid high glycemic index food items (such as sweets, white bread, sodas, fruit juices, or syrups) or to introduce fat or protein together with these items, at breakfast, for example. They were encouraged to chose low glycemic index foods (such as whole wheat bread). They were also told to split food intake into five to seven small meals and not to drink and eat at the same time. This was done through a consultation with a senior dietician.
The evaluation of the symptoms (early and late, according to Tack et al. 7 ) and of the CGM was carried out before and after 6 weeks of treatment. The Sigstad score was applied to diagnose dumping syndrome, 7 which is positive above 7 and has a maximum score of 25.
Gastric bypass was performed as described by Topart et al. 18
Continuous interstitial glucose (IG) was recorded for at least 3 days on an outpatient basis (CGMS® System Gold™, Medtronic MiniMed, Northridge, CA). The electrodes were installed in the patients in the hospital. Calibration was performed three times per day. There was no technical problem such that the monitoring had to be repeated. Patients were blinded to the results as the monitor did not display the IG. Patients were only trained to calibrate the device, to record the food they ate and mealtimes, and to mark the events (meals, exercise, hypoglycemic episodes, etc). The first recording was done before dietary counseling, and the second was after 6 weeks of dietary counseling and acabose treatment.
At the end of each CGM recording period, the data were downloaded from the monitor and analyzed using the manufacturer's software to obtain the IG (mean and SD), the minimum and maximum IG, and the percentage of time spent below 60 mg/dL and above 140 mg/dL (IG values that occur in only 1% of healthy patients). 19 Other specific parameters designed to further describe glucose variability were also calculated. The time to the postprandial peak was defined as the time between the lowest value before an identified meal (within 15 min before) and the highest value after this meal. The mean amplitude of glucose excursions (MAGE), a major index of intra-day glucose variability, was calculated as described by Service et al. 20 The rates of increasing and decreasing IG were calculated after each meal and expressed as mg/dL/min.
Statistical methods
Results are expressed as mean±SD values. The means were compared with a Mann–Whitney nonparametric test. Statistical significance was accepted at the 5% level.
Results
Most patients were women (seven of the eight) 37–58 years old, weighing 105–150 kg before surgery, who lost 12–34% of their weight after the gastric bypass. The delay between surgery and symptoms was 1–24 months. One patient had diabetes before the operation and was no longer treated for the disease after surgery. Symptoms occurred 34±17 min after the initiation of the meals. The Sigstad score ranged from 7 to 14. Three patients presented the early symptoms, five presented the late ones, and all had adrenergic symptoms. None presented with severe hypoglycemia requiring third-party intervention.
Acarbose treatment was well tolerated with the adapted doses. The symptoms disappeared in seven out of the eight patients after treatment.
The patients failed to totally reduce food items with a high glycemic index. The percentage of meals only containing carbohydrates with a glycemic index higher than 60 was 21±9% (range, 13–31%) before and 13±15% (range, 0–38%) after the intervention. The percentage of meals containing carbohydrates with a glycemic index higher than 60 within a mixed meal was 71±11% (range, 60–87%) before and 67±10% (range, 62–87%) after the intervention. The percentage of meals containing carbohydrates with a glycemic index lower than 60 was 8±13% (range, 0–27%) before and 20±14% (range, 0–39%) after the intervention.
Table 1 describes the CGM parameters before and after treatment. Six of the eight patients had IG values below 60 mg/mL before treatment. There was a nonsignificant decrease in the mean and maximum IG and of the time spent above 140 mg/dL. There was a significant increase in the time to the IG peak (from 52 to 98 min) and a decrease in the rate of the IG increase after the start of the meals. There was a significant decrease in the time spent below 60 mg/dL (from 2.5% to 0.18%) and of the rate of the IG decrease after the peak. The minimum IG values significantly increased with the treatment.
After the meal.
After the peak.
IG, interstitial glucose; MAGE, mean amplitude of glucose excursions.
Six patients spent more than 1% of the time with IG values below 60 mg/dL before treatment, but only one after treatment. Before treatment only one patient spent significant time with an IG neither below 60 or above 140 mg/dL. Four patients were in this category after treatment.
Figure 1 shows the case of one patient before and after treatment.
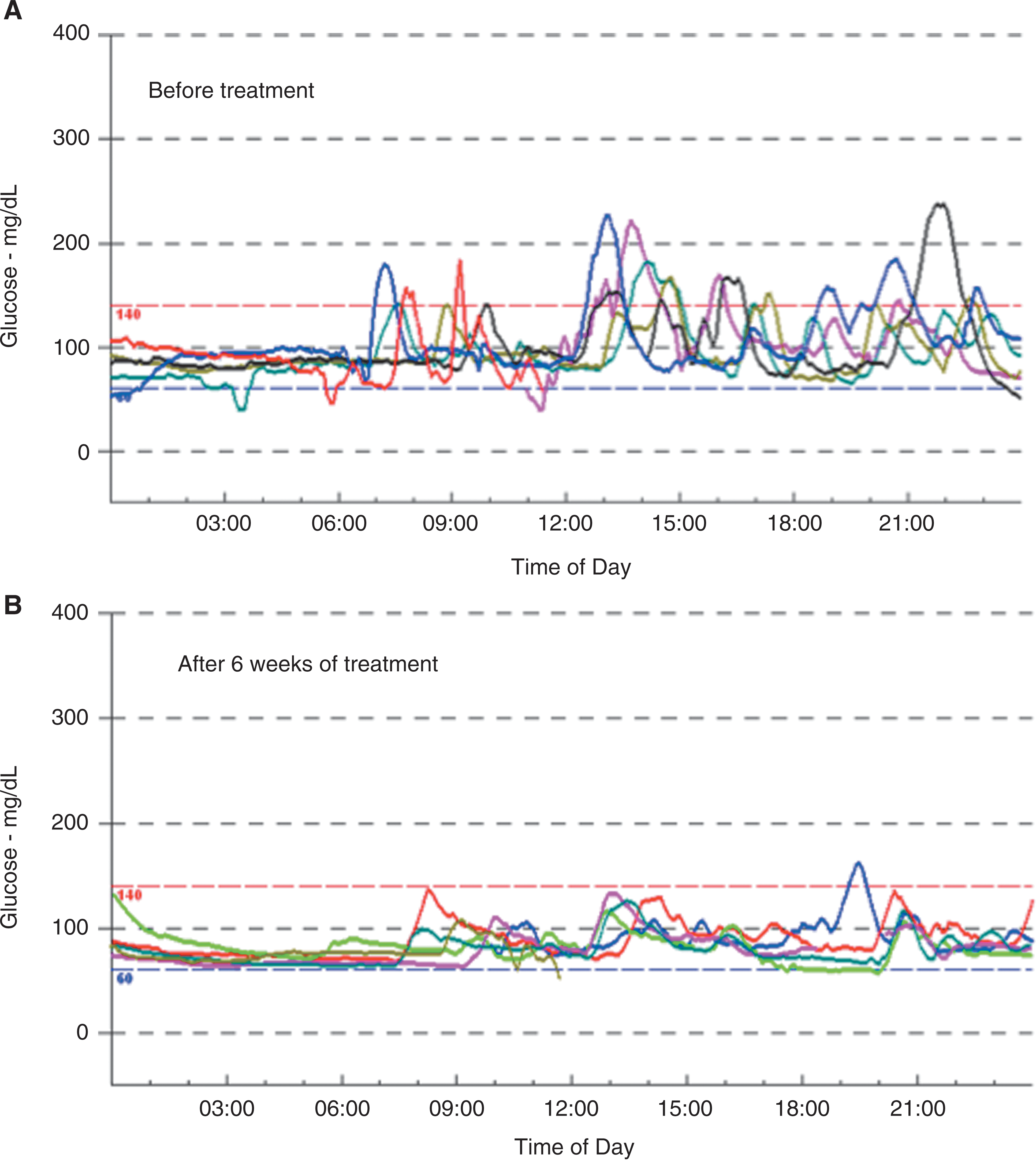
Continuous glucose monitoring profile in a patient (
Discussion
The present study is the first to report an improvement of the symptoms and of the IG profiles after treatment with dietary counseling and acarbose, in real life circumstances, of patients suffering from late dumping syndrome after RYGB.
The study has weaknesses that should be acknowledged. It is not a randomized trial comparing the treatment with acarbose to a placebo. Therefore, we cannot rule out that the improvement was solely explained by the dietary changes. Indeed, a strict low-carbohydrate diet can limit the glycemic variability after a test meal. 2,4 However, the patients in the present study were given the recommendation to reduce food items with a high glycemic index by a senior dietician, but they failed to do so completely. After the treatment period they had increased the amount of fiber (brown bread) but were still consuming sweet food. Therefore, we suggest that acarbose did influence the CGM parameters in addition to the influence of the diet.
Most (seven of the eight) patients treated by dietary counseling plus acarbose no longer presented symptoms of the late dumping syndrome and showed an improvment in the CGM parameters that have been described in such cases by Hanaire et al. 12 In that initial study, patients with hypoglycemic episodes after RYGB had higher IG variability than controls (type 2 diabetes and healthy subjects). They spent more time above 140 mg/dL and below 60 mg/dL, had higher rates of IG increase after a meal and of IG decrease after the peak, and had a dramatically reduced time to the IG peak after the meal. In the present study it is suggested that dietary counseling plus acarbose corrected some of the CGM features. The time to the peak after a meal was almost doubled and reached values (98 min) similar to those of the controls. 12 We know of no other circumstances where this time is modified and of no other treatment except acarbose to increase it. The time spent below 60 mg/dL was significantly reduced, and that above 140 mg/dL not significantly so. This contributes to the limiting of the IG variability, although the MAGE and the SD of the IG values were not significantly reduced.
Acarbose is an inhibitor of α-glucosidase that hydrolyzes complex carbohydrates, notably starch, into glucose units. Acarbose is therefore expected to slow down carbohydrate digestion and to delay the glycemic peaks after a meal. Therefore, the increase in the time to the peak and the reduction in the time spent above 140 mg/dL are likely to be directly due to the effect of the acarbose.
Acarbose has been used for the treatment of reactive hypoglycemia outside the surgical context. 21 It has also been used for the treatment of the dumping syndrome after gastrectomy for cancer or ulcers. 14 –16 Three case reports had suggested its use in patients presenting hypoglycemia after a gastric bypass. 4,13,17 A recent study 8 reported eight cases of severe hypoglycemia after an RYGB and compared the features of the CGM with those in asymptomatic operated patients. The authors suggested that CGM is a useful tool to diagnose asymptomatic hypoglycemic episodes and that, despite the acarbose treatment, patients with severe hypoglycemia still had higher IG values than asymptomatic patients. The study was not designed to compare CGM features before and after treatment.
Accordingly, we have observed a lower rate of decreasing IG values and then the time spent below 60 mg/dL with dietary counseling and acarbose. We cannot conclude that the reduction in the hyperglycemic peaks is responsible for the decrease in the time spent below 60 mg/dL. However, many reports suggest that hypoglycemic episodes after a gastric bypass follow early and transient hyperglycemic peaks, 3,6,8 –12 suggesting that future studies are required to understand better post-bypass hypoglycemia. The results of this pilot study should be completed by those of a controlled trial comparing dietary modifications with or without treatment with acarbose.
However, in the present study, dietary counseling plus acarbose treatment failed to fully correct the hyperglycemic peaks because 5% of the time was still spent above 140 mg/dL, whereas the corresponding time is below 1% in healthy controls. 19
In conclusion, dietary counseling plus acarbose treatment dramatically improved both the symptoms and the CGM parameters of late dumping syndrome in patients after RYGB. It restored the time to the peak IG after a meal, which appears to be a specific feature of the CGM profile after RYGB. It limited the glycemic excursions but did not fully correct the glycemic variability.
Footnotes
Author Disclosure Statement
No competing financial interests exist.