
Abstract
Background:
Severe hypoglycemic events are a major consequence of tight diabetes control. Continuous glucose monitoring systems (CGMSs) were recently introduced in order to minimize the risk of hypoglycemia. However, the present CGMSs are invasive and costly and have been recently demonstrated to be intolerant for most children and adolescents. Hence there is a need for a simple, noninvasive, convenient, and inexpensive device to detect hypoglycemic events. The Gili Medical Hypoglycemia Non Invasive Monitoring System (GMHNIMS) (Gili Medical Ltd., Migdal HaEmek, Israel) has been currently developed for these purposes.
Subjects and Methods:
Ten patients 14–18 years old with type 1 diabetes for at least 1 year participated in a pilot study that was held at the Meyer Children's Hospital, Rambam Medical Center, Haifa, Israel. All patients were either treated by insulin pump or by multiple daily injections. The GMHNIMS was connected to the study subjects during three consecutive nights in an inpatient setting while they received their usual insulin regimen. The system is composed of four sensors (heart rate, perspiration, skin temperature, and tremor) that detect physiologic changes during hypoglycemia. In addition, each patient was connected to a real-time CGMS for 3 nights. When a hypoglycemic event was suspected clinically by the patient, a bedside capillary glucose was checked by a glucometer.
Results:
The system was found to be convenient without any disturbances to sleep quality. The sensitivity of the GMHNIMS for detection of true hypoglycemic events was 100% with specificity of 85.7%.
Conclusions:
The new device showed high detection rates of nocturnal hypoglycemic events with an acceptable degree of false-positive readings. Being inexpensive and noninvasive, this device has the potential for routine use in insulin-treated patients.
Introduction
Recurrent mild hypoglycemia may give rise to hypoglycemic unawareness and hence increase the risk of severe hypoglycemia. 8 Standard methods for self-monitoring blood glucose provide patients merely with intermittent, single point-in-time snapshots of glucose levels. The readings often miss marked and sustained hyper- and hypoglycemic excursions mainly during the night. 9 In order to overcome these caveats, semi-invasive continuous glucose monitoring systems (CGMSs) were developed. 10 –12 Intermittent use of CGMSs has been shown to be a good mean of insulin dose adjustment in patients with frequent hyper- or hypoglycemia events. 13 However, it has been shown that this modality is effective in only small subpopulations of diabetes patients. 14 The Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group 15 demonstrated that only 21% of the pediatric cohorts with type 1 diabetes mellitus were able to continue the frequent use of these devices. Moreover, CGMSs are costly and therefore not available for most patients with type 1 diabetes mellitus.
Therefore, there is a need for a noninvasive, convenient, reliable, and inexpensive device to detect hypoglycemia. The Gili Medical Hypoglycemia Non Invasive Monitoring System (GMHNIMS) (Gili Medical Ltd., Migdal HaEmek, Israel) described in this article was developed for these purposes. Our device is based on measuring four physiological parameters related to hypoglycemic events concurrently and therefore is proposed to give better results than other devices based on fewer parameters. The device does not include any disposable parts so that its price would probably be less than the annual cost of operating a CGMS.
Other noninvasive devices have been developed to detect hypoglycemia. For example, the HypoMon® (AiMedics Pty. Ltd., Eveleigh, NSW, Australia) is a noninvasive nocturnal hypoglycemic alarm system based on electrocardiogram and sweating parameters. 16,17 The GlucoWatch® Biographer (formerly Cygnus Inc., Redwood City, CA; now Animas Corp., West Chester, PA) provides frequent and automatic glucose readings noninvasively. 18
The aim of this study was to test the newly developed device and to evaluate the ability of the first prototype to reliably detect nocturnal hypoglycemic events. Specifically, the study was designed to test the correlation between the new algorithm and the results of the CGMS.
Subjects and Methods
Recruitment and study participants
The subjects were recruited from the Pediatric Diabetes Clinic at the Rambam Medical Center (Haifa, Israel). The inclusion criteria were adolescents (12–18 years old) diagnosed with type 1 diabetes for more than 1 year, without a history of hypoglycemia unawareness, with glycated hemoglobin (HbA1c) above 7% (within the last 3 months) and ability to read and understand the study purpose, and parental consent was obtained.
The exclusion criteria were inability to give informed consent, the subject was taking any medication that may affect the results of this study, and the subject was participating in another clinical trial.
The study group consisted of 10 adolescents (seven girls) with type 1 diabetes recruited by the Pediatric Diabetes Clinic in a tertiary referral center. Their age range was 14–18 years (median, 16.75 years). Duration of diabetes was 5.7±4 years. The adolescents remained on their usual insulin regimen throughout the study. Four adolescents were on insulin pumps, and six were treated by multiple daily injections. The average HbA1c level was 9.7%. None of the adolescents was using other medication except insulin and did not have any other chronic illness. None of the adolescents had evidence for microvascular complications. The study was approved by the Rambam Medical Center's Committee for Human Subject Studies. Each participant and his or her parents (for those patients younger than 18 years) signed an informed consent.
Data and procedures
Each patient arrived at the hospital on the first day of the experiment, underwent a medical examination, and was informed about the purpose and the procedure of the experiment. The patient was then connected to the approved subcutaneous continuous glucose sensor (DexCom, Inc., San Diego, CA).
In the evening the patient was connected to the GMHNIMS and laid in bed for his or her night's sleep. Both the alarm of the DexCom CGMS and the Gili Medical device were deactivated. Throughout the night, glucose levels and the relevant physiological parameters (oxygen saturation, heart rate, movements, skin conductance body temperature, and photoplethysmograph signal) were monitored. The same procedure was repeated during the second and the third night of the experiment.
If the patient woke up because a hypoglycemic event was suspected, the hypoglycemia was confirmed by self-measurement of blood glucose (less than 70 mg/dL), he or she was then treated accordingly, and the experiment was continued. The experimenter was blinded to the CGMS recordings throughout the experiment. Calibration was entered into the system by the hospital nurse before the subject went to sleep.
After three successive nights the data files obtained from the CGMS and the GMHNIMS were investigated for analysis and comparison.
GMHNIMS
The system is intended to warn insulin-treated diabetes patients or their parents of a hypoglycemic reaction occurring while they are asleep. Its uniqueness is the monitoring of several physiological effects concurrently, along with an algorithm for detecting an imminent hypoglycemic event based on these physiological effects.
The GMHNIMS consists of a monitor and a transmitter. The monitor is used to record in real time several physiological parameters received from different sensors (as presented in Fig. 1), while the transmitter is designed to evaluate the glucose level, from which the hypoglycemia condition can be detected.

Presentation of the Gili Medical Hypoglycemia Non Invasive Monitoring System.
The system is not a direct measure of low blood sugar. Instead, it monitors four symptoms expected to be related to hypoglycemic events: increased perspiration (decrease in skin conductivity), peripheral vasoconstriction (decrease in body surface temperature), trembling, and increased heart rate. The data collected are stored in the monitoring system and transmitted to the Gili Medical computer via the system software. Using the built-in algorithm, the GMHNIMS is able to detect the physiological changes related to hypoglycemia obtained from the sensors' array, analyze them, and provide an alarm if an event is detected.
The GMHNIMS contains four sensors: 1. The heart rate was sampled by the NONIN sensor (OEM III; NONIN® Medical, Plymouth, MN) in a sampling rate of 3 Hz. Heart rate was represented by average values in each 5-min interval. A significant increase in heart rate was defined by more than 15 bpm difference. 2. Perspiration level was calculated from the conductivity levels between the electrodes of the perspiration sensor (TDS203; BIOPAC, Goleta, CA) that had been connected to the skin. The sampling rate was at a frequency of 75 Hz, while the average value in each 5-min interval was shown. High perspiration levels were defined at skin conductivity values lower than 250 kΩ (compare with the Teledyne [Teledyne Avionics, Charlottesville, VA] Sleep Sentry
19
). 3. For the subject's skin temperature, we sampled the sensor voltage (TMP35; Analog Devices, Norwood, MA) at a frequency of 75 Hz. Skin temperature was represented by the average values in each 5-min interval. 4. The movement level was defined by the number of "seconds with movements" in each 5-min interval. A "second with movement" was termed when the average acceleration level was greater than 1.3 G. A significant increase in movements was defined by more than 30 s with movements. We used an actigraph device (ADXL335; Analog Devices) that is used to record body movements based on electromyographic activity.
20
The changes that occurred in each sensor over the experiment time lines were recorded and analyzed according to the algorithm developed. The expected physiological changes related to hypoglycemic events were increase in heart rate, increase in movements, decrease in body temperature, and decrease in skin conductivity (increased perspiration). For each sensor, the changes monitored were given a linear score between 1 and 0 (a significant increase and a nonsignificant difference, respectively) proportionally to the size of change. A "total score" was then calculated for each time frame. An event was marked when the total score was at least 3. This was then compared with hypoglycemic events defined by differences in glucose levels that had been recorded by the DexCom sensor over the same time frames and the glucometer measurement.
Figures 2 and 3 show examples of the total score and the DexCom recording over the same experiment time line for two different adolescents: when a hypoglycemic event had occurred and when no hypoglycemic events occurred, respectively.
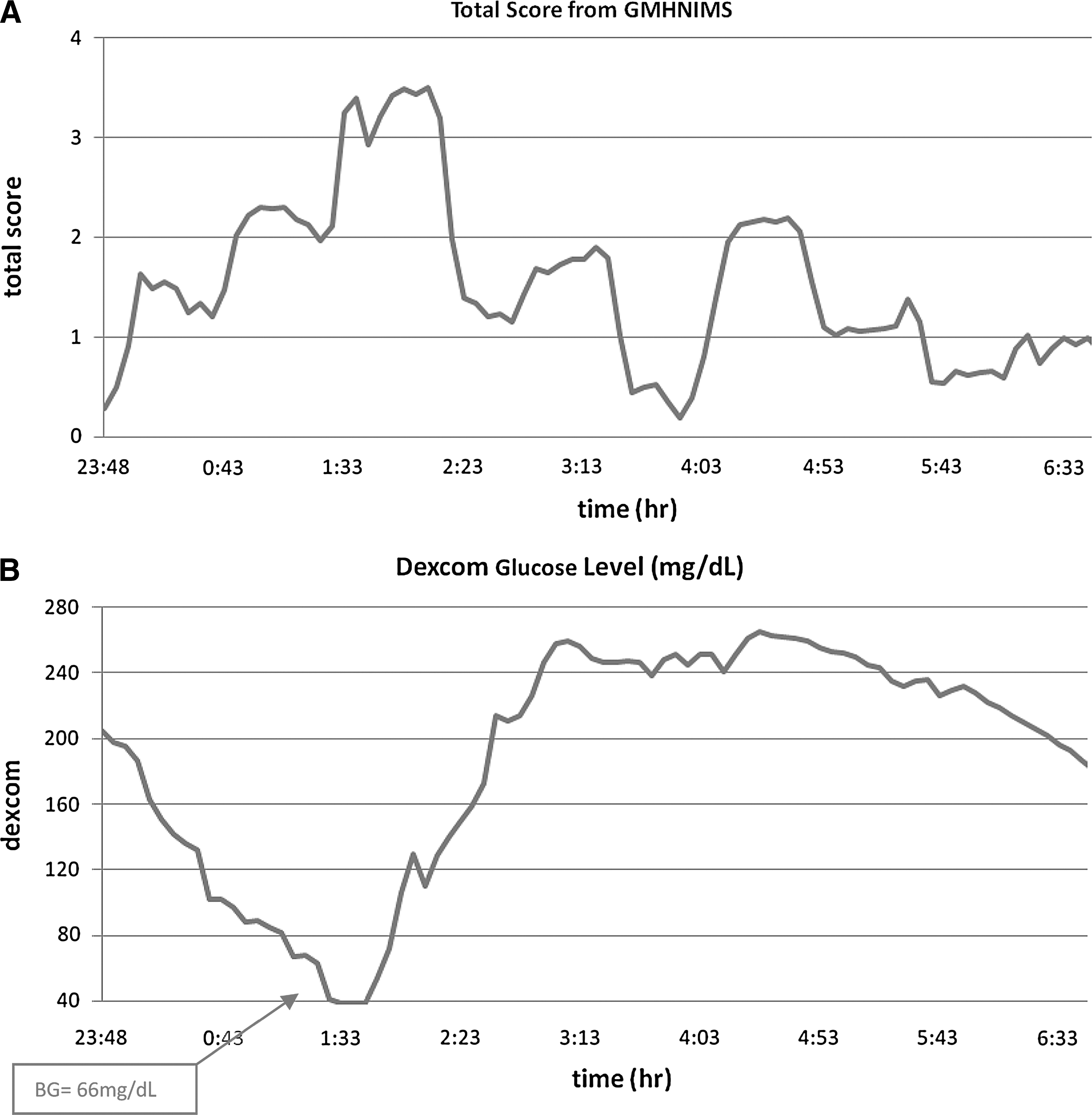
Subject A. A hypoglycemic event had occurred. Both (
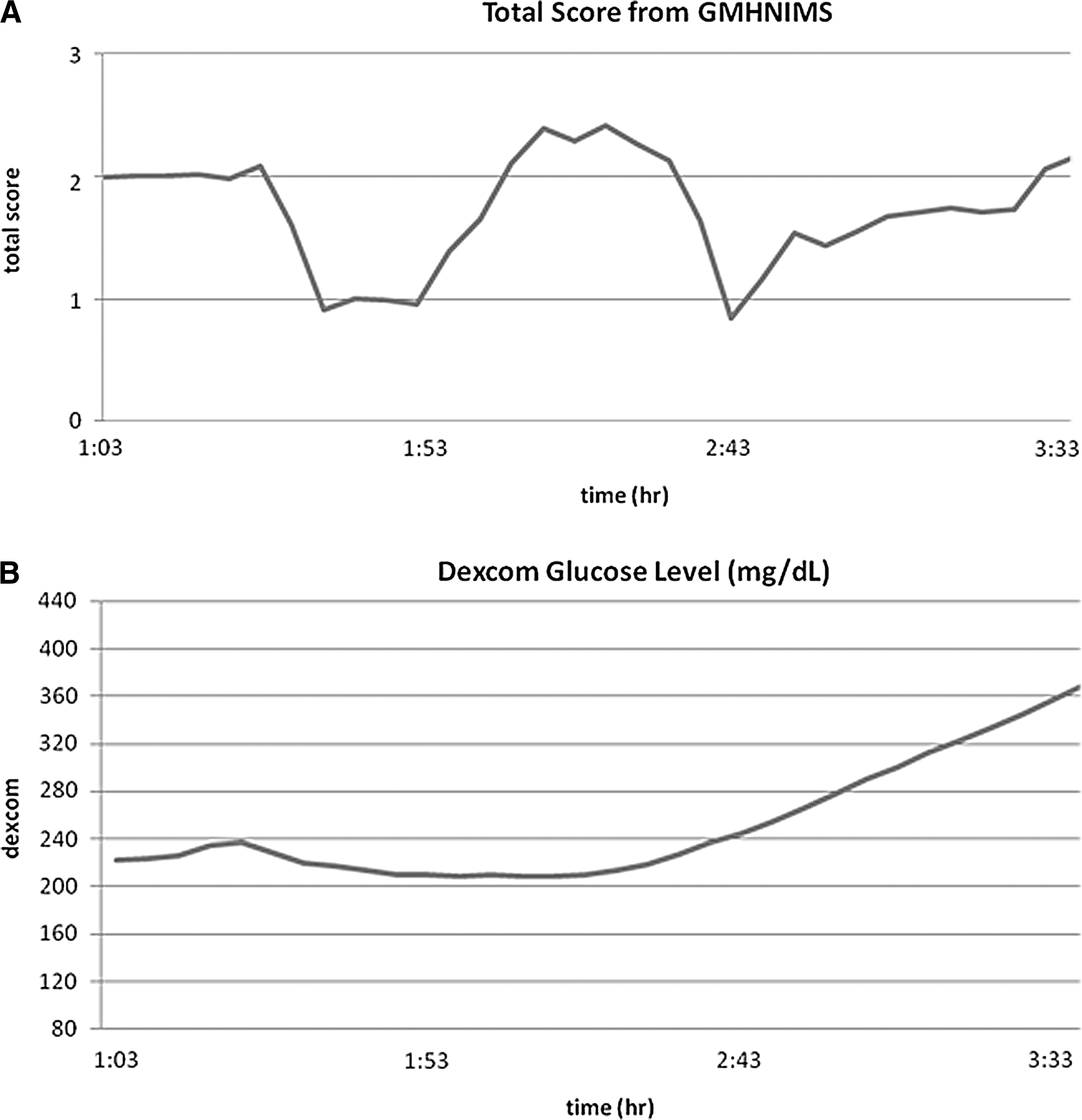
Subject B. No hypoglycemic events occurred. (
Results
Of the 10 patients who participated in the experiment for three successive nights each, there were 22 nights with valid data (missing data: 4 nights due to DexCom failure to log data, 3 nights due to GMNHIMS failure to log data, and 1 night due to subject noncompliance). The device was found to be well tolerated. No adverse events were recorded during or after the study.
Nine of nine hypoglycemic events that were confirmed by the glucometer measurement were detected by the GMHNIMS. According to these results, the sensitivity and specificity of the GMHNIMS are 100% and 85.7%, respectively. True-negative events were defined when the GMHNIMS did not detect a hypoglycemic event and in offline analysis CGMS values were above 70 mg/dL.
False-negative events were defined when the Gili Medical device detected a hypoglycemic event while in offline analysis CGMS values were above 70 mg/dL.
Events detected by the CGMS were confirmed by the adolescents waking because of events and by glucometer measurements. If a false-negative event occurred, that whole night was considered a false-negative night (i.e., 2 nights). The specificity calculation was defined as the number of false-negative nights out of the total number of non-event nights according to the CGMS.
The scoring analysis for all true events and false events during the whole experimental nights revealed that the average score for hypoglycemic events (mean, 3.40; SD, 0.37) was higher than the average score for false events (mean, 2.40; SD, 0.72). Based on the unequal variance t test, this difference is highly significant (t 27.5=5.135, P<0.001), suggesting that the times prior to the development of severe events have an effect on the relevant physiological measures recorded by the GMHNIMS, and thus on the total score, compared with the times prior to non-events.
Discussion
CGMSs were developed to overcome the under detection of hyper- and hypoglycemic events by self-monitoring of blood glucose. 9 However, the inconvenience of using CGMS devices is the major obstacle to more consistent use of these systems. 21 In addition, in patients with type 1 diabetes mellitus variation in plasma insulin and glucose levels might affect CGMS performance. Hyperinsulinemia itself reduces interstitial glucose concentration, as detected by the sensor compared with plasma glucose values at around 20% in humans. 22 The sensor interstitial fluid glucose level tends to lag behind the blood glucose level, causing the device to underestimate the true rate of fall in glucose insulin-induced hypoglycemia in some patients. 11 Therefore there is a need for a noninvasive, convenient, and reliable device for the detection of hypoglycemia. The device studied here has a potential to be such a device. We have shown high levels of accuracy in detection of nocturnal hypoglycemic events. The device was found to be safe and convenient.
Nocturnal hypoglycemia is reported in 13–56% of adolescents with type 1 diabetes mellitus. In more than 50% of the patients it may be asymptomatic. 23 So far, no noninvasive method for detecting asymptomatic nocturnal hypoglycemia has been proven successful. The HypoMon, as previously mentioned, is a noninvasive device that is worn by the patient in a belt at nighttime. It picks up on a body's stress response symptoms (such as sweating) and alerts the wearer (or caretaker in the case of a young child) to the facts that hypoglycemia might be happening. Nevertheless, recent studies reported a sensitivity of 73% and specificity of 68%. 16,17
Another noninvasive device that has been studied is the GlucoWatch Biographer. This device provides frequent and automatic glucose readings noninvasively. Although the device has been shown to be safe and well tolerated and may improve glucose control in children, it has some limitations, including relatively high incidence of false-positive alarms, calibration failure when there are significant changes in skin temperature or excessive sweating, and skin irritation from use of the Biographer. 18
The current study included 30 experimental nights from 10 patients with type 1 diabetes mellitus who were connected to the DexCom glucose sensor and the GMHNIMS. During this time, nine hypoglycemic events occurred (one a repeated event). The risks associated with the use of the GMHNIMS seem to be low.
Comparing the results obtained from the GMHNIMS with hypoglycemic events suspected by the patient and confirmed by the glucometer reveals extremely high detection rates (100%) of the system with relative low (14.3%) false-positive rates (lower than other off-the-shelf sensors). CGMS recordings did not show any events that had not been suspected by the patients. These results imply that not only can the GMHNIMS activate an alarm in order to try to wake up the patient prior to all cases of severe nocturnal hypoglycemic events and thus prevent deleterious effects, but also the system can activate an alarm in order to try to wake up the patient during all mild nocturnal hypoglycemic events. The results also show that the system caused the patient to falsely wake up in only 2 out of 22 nights. Moreover, the GMHNIMS has a high distinguishable ability between times of events and non-events, as concluded from the significant difference resulting between scores obtained from the GMHNIMS at times prior to events compared with those obtained prior to non-events.
This study was a pilot study that included patients with relatively high HbA1c. Future research should include a larger sample size with a variety of HbA1c levels, especially tightly controlled patients. The definition of the cutoff point for significant differences in each of the four sensors should be further investigated. Further studies should also include improved sensors, aiming at minimizing missing values as a result of technical disconnections.
The data collected will assist in developing the final design of the system. In order to be an acceptable device by adolescents and also not to miss as many nights as the CGMS, technical and aesthetic improvements will need to be made, such as creating a bracelet-like hypoglycemia noninvasive monitoring system.
Footnotes
Acknowledgments
This study was funded by Gili Medical Ltd.
Author Disclosure Statement
A.S. and V.A.-B.-Y. are employees of Gili Medical Ltd. N.W. and N.S. are medical consultants for Gili Medical. No competing financial interests exist for O.E. and N.Z.-L.