
Abstract
Background:
The additive effect of α-glucosidase inhibitors (α-GIs) was investigated in patients with type 2 diabetes (T2D) under control with rapid-acting insulin analog.
Subjects and Methods:
Thirty-six poorly controlled T2D patients were recruited, and plasma glucose (PG) was controlled by three times daily injection of insulin lispro mix 50/50 (Mix50) to maintain fasting PG <130 mg/dL and 2-h postprandial PG (PPG) <180 mg/dL. Another group of 20 patients was randomly assigned to either 0.3 mg of voglibose or 50 mg of miglitol, which was administered at breakfast every other day. Another group of 16 patients was assigned to a crossover study, in which each α-GI was switched every day during the 6-day study. PPG, C-peptide, and lipid profile were analyzed.
Results:
The addition of voglibose had no effect on PPG, but miglitol blunted the PPG rise and significantly decreased 1-h and 2-h postprandial C-peptide levels compared with Mix50 alone. In addition, miglitol significantly decreased the 1-h postprandial triglyceride rise and the remnant-like particle-cholesterol rise, while it increased the 1-h postprandial high-density lipoprotein-cholesterol and apolipoprotein A-I levels in the crossover study.
Conclusions:
Miglitol appears to have rapid action, which appears earlier than that of lispro. The combination of miglitol and Mix50 seems effective for the control of PPG and lipid profile in T2D.
Introduction
The use of the recently developed continuous glucose monitoring system has identified a significant number of diabetes patients with peak postprandial PG (PPG) occurring around 1 h postprandial. 9 The American Diabetes Association has also focused on the control of PPG and recommended that peak PPG, not 2-h PPG, should be <180 mg/dL. 10 Despite these reports and guidelines, the PPG profile has neither received adequate attention nor been controlled in the majority of diabetes patients in current clinical practice.
To investigate the PPG profile of diabetes patients, we conducted a clinical survey in 50 T2D patients who were admitted to our facility because of poor glucose control by oral glucose-lowering medications. The patients were treated with insulin analogs, including lispro and aspart, to maintain fasting PG <130 mg/dL and 2-h PPG <180 mg/dL, and then PPG was evaluated throughout the morning. The results showed that 78% of the patients with the targeted PG had approximately 50 mg/dL (on average) higher 1-h PPG than 2-h PPG, suggesting that even rapid-acting insulin analogs cannot achieve ideal PPG in T2D. 11 Based on the results of the above survey (published in preliminary abstract form 11 ), we conducted the present study to determine the therapeutic procedure(s) that can achieve “normal” PPG in T2D patients treated with rapid-acting insulin analogs. The results showed that miglitol, an α-glucosidase inhibitor (α-GI), controlled PPG and also improved postprandial lipid profile.
Subjects and Research Design
Subjects
The patients enrolled in this study had been diagnosed with T2D according to World Health Organization classification. Their PG concentration was poorly controlled with oral antidiabetes medications (fasting PG, 192.8±12.1 mg/dL; glycated hemoglobin, 10.3±0.4%) until admission to our hospital. Their fasting plasma lipid profile at the time of admission was as follows (mean±SE values): triglycerides, 150.0±21.5 mg/dL; low-density lipoprotein-cholesterol (LDL-C), 110.7±6.6 mg/dL; high-density lipoprotein (HDL)-cholesterol (HDL-C), 50.8±30 mg/dL; and nonesterified fatty acids (NEFAs), 0.52±0.04 mmol/L. Participants were recruited from the hospitalized patients who agreed to participate in the study during a period from 2008 February to 2011 June. The patients were placed on a diabetes diet with 27 kcal/kg of ideal body weight (carbohydrate, 56%; protein, 17%; fat, 27%) under the guidance of a registered dietitian, and all oral antidiabetes medications were withdrawn on admission to the hospital. The patients were also encouraged to exercise (walking for 30 min) after every meal, carrying a map of the hospital with several checkpoints indicated. PG was controlled by three times daily injections of insulin lispro mix 50/50 (Mix50). The insulin dose was titrated to maintain fasting PG <130 mg/dL and 2-h PPG <180 mg/dL (taking 3–4 weeks), and the dose was fixed during the following randomized or crossover study. Patients with advanced complications of diabetes or cancer were excluded. The study was conducted in accordance with the Declaration of Helsinki and was reviewed and approved by the ethics committee of the University of Fukui.
Randomized study
To assess the additive effects of α-GIs on PPG and lipid profile, 20 patients were randomly assigned to either 0.3 mg of voglibose or 50 mg of miglitol. The patients were administered either α-GI at breakfast every other day (days 2, 4, and 6) during the 6-day study, in addition to Mix50. The carbohydrate and fat contents of the breakfast were adjusted during the study period. Blood was drawn at 0, 1, 2, and 4 h after breakfast time during the study to measure PG, and the mean value of the 3 days (days 1, 3, and 5 or days 2, 4, and 6) for each time point were compared between the two conditions (Mix50 alone vs. Mix50 + α-GI). Plasma concentration of C-peptide, triglycerides, LDL-C, HDL-C, and NEFAs were also analyzed using plasma samples taken on days 1 and 2. Patients refrained from exercise in the morning during the study.
Crossover study
Another group of 16 patients was assigned to the crossover study, in which a test meal was provided at breakfast and the α-GI was switched every day during the 6-day study. The first eight patients were treated with voglibose on days 1, 3, and 5 and with miglitol on days 2, 4, and 6; the last eight patients were treated with miglitol on days 1, 3 and 5 and with voglibose on days 2, 4, and 6. In addition to the parameters measured in the randomized study, plasma lipoprotein profile and concentration of apolipoprotein (apo) forms and remnant-like particle-cholesterol (RLP-C) were analyzed on day 0 (Mix50 alone), day 1 (Mix50 + voglibose or miglitol), and day 2 (Mix50+miglitol or voglibose). RLP-C measures cholesterol concentration in the lipoprotein fraction purified by an immunoaffinity mixed gel coupled with monoclonal antibodies against apo B-100 and apo A-I and represents plasma concentration of remnant particles. 12
Statistical analysis
Data are expressed as mean±SE values. Statistical analyses were performed using a paired or unpaired t test between the conditions. A P value of <0.05 was considered statistically significant.
Results
Subjects
All 36 patients completed the study without serious adverse events, including hypoglycemia or liver dysfunction. Table 1 lists the clinical characteristics and baseline laboratory data. The baseline glycated hemoglobin ranged from 6.2% to 12.4%, with a mean value of 9.0±0.3%. The subjects required 16.2±1.3 units of Mix50/day for the control of PG within the targeted range, and 7.7±0.7 units was used at breakfast to control 2-h PPG at <180 mg/dL. The fasting plasma C-peptide concentration was 1.2±0.1 μg/L, indicating significant secretion of endogenous insulin. The subjects did not have overt dyslipidemia, although some patients had a slightly elevated (to approximately 202 mg/dL) fasting plasma triglyceride concentration. There were no significant differences in the other parameters except LDL-C among the three groups.
Data are mean±SE values.
P<0.05 versus voglibose or crossover group.
BMI, body mass index; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
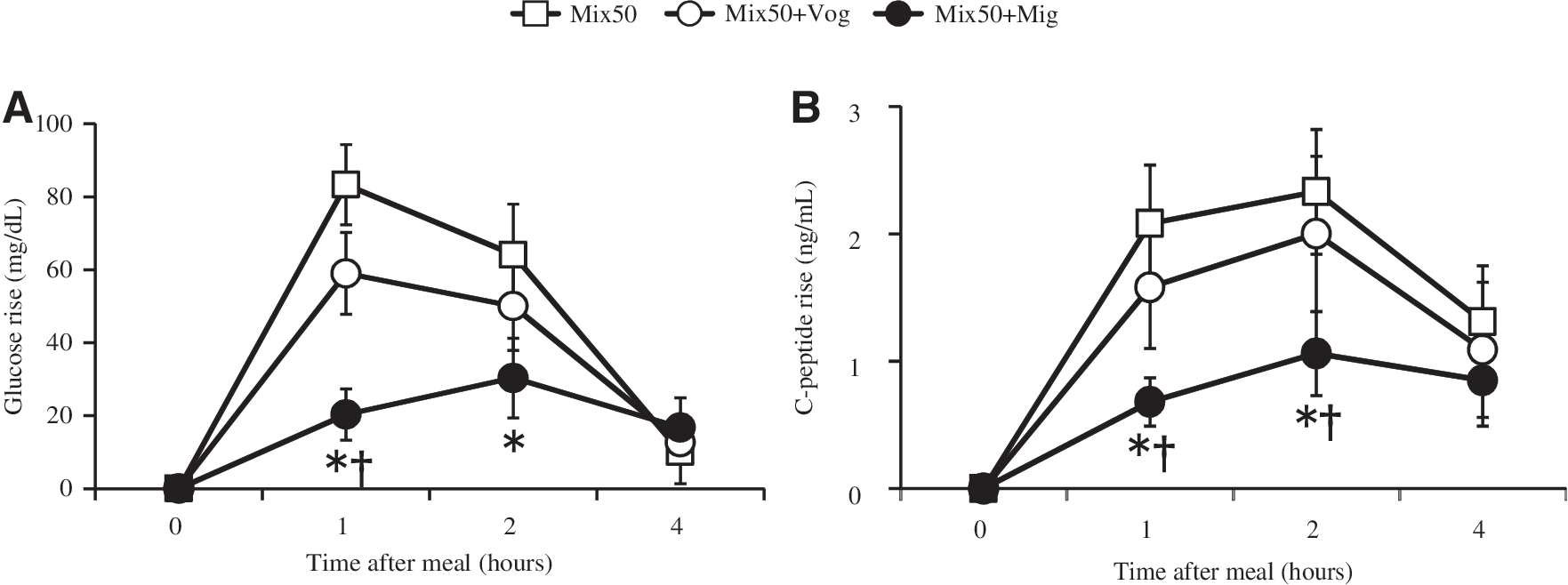
Randomized study
To investigate the efficacy of the α-GIs, 20 subjects were randomly assigned to voglibose or miglitol, and their metabolic parameters were compared. As shown in Figure 1A and B, respectively, although voglibose had no effect on PPG, miglitol markedly decreased 1-h and 2-h PPG when combined with Mix50. PPG rose to 71.4 mg/dL at 1 h postprandial with Mix50 alone, whereas it rose only to 2.1 mg/dL at 1 h postprandial and 13.6 mg/dL at 2 h postprandial (Fig. 1B). Neither voglibose nor miglitol had any effect on 4-h PPG. Thus, miglitol achieved almost “flat” PPG, when administered in combination with Mix50. The 1-h and 2-h postprandial plasma C-peptide concentrations were also significantly lower in those patients on miglitol, whereas voglibose had no effect (Fig. 1D and C, respectively). Although statistically insignificant, 1-h postprandial plasma triglyceride tended to decrease in the miglitol group when treated with miglitol (1-h change=5.2±3.5 mg/dL without miglitol vs. −2.3±3.3 mg/dL with miglitol, P=0.06), whereas it was comparable with or without voglibose in the voglibose group (1-h change=0.4±3.7 mg/dL without voglibose vs. −0.1±3.9 mg/dL with voglibose). The other components of the lipid profile were not significantly affected by the administration of either α-GI.

Effects of voglibose (Vog) and miglitol (Mig) on
Crossover study
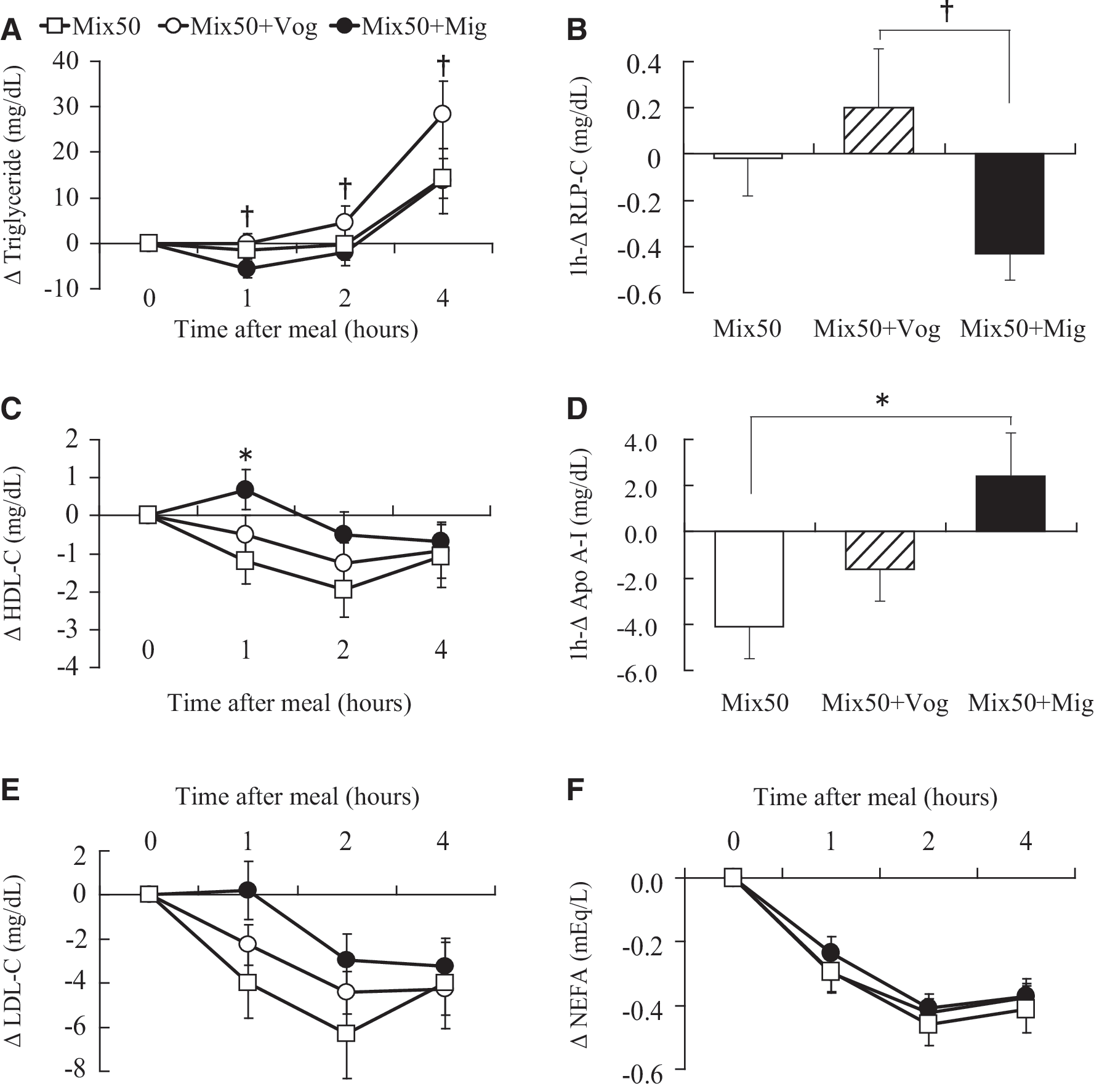
In order to confirm the effects of miglitol demonstrated in the randomized study, a crossover study was conducted in another group of 16 patients. As shown in Figure 2, miglitol, but not voglibose, significantly reduced PPG and C-peptide concentration compared with those after Mix50 alone. To clarify the effects of miglitol on postprandial lipidemia, we analyzed plasma lipid profile and apo concentrations. In support of the results of the randomized study, miglitol significantly reduced the postprandial plasma triglyceride concentration compared with voglibose throughout the morning (Fig. 3A). Parallel to its effect on triglyceride concentration, miglitol reduced the 1-h postprandial RLP-C concentration by 0.4 mg/dL (6.3%), whereas voglibose increased it by 0.2 mg/dL (3.1%) (P<0.05) (Fig. 3B and Table 2). On the other hand, miglitol tended to reduce the 1-h postprandial very low-density lipoprotein (VLDL) fraction, which was assessed by acrylamide gel, whereas voglibose and Mix50 alone increased it (P=0.06) (Table 2). In contrast to triglyceride and RLP-C, 1-h postprandial plasma HDL-C and apo A-I concentrations increased with miglitol, whereas they decreased with voglibose or Mix50 alone (Fig. 3C and D and Table 2). Other lipid parameters, including LDL-C and NEFAs, were not affected by the addition of either α-GI (Fig. 3 and Table 2). Thus, miglitol appeared to have distinct effects not only on PPG and C-peptide, but also on postprandial lipid profile, suggesting its rapid action on postprandial metabolism of remnant and HDL particles.
Effects of voglibose (Vog) and miglitol (Mig) on postprandial
Effects of voglibose (Vog) and miglitol (Mig) on postprandial
Data are mean±SE values.
P<0.05 for insulin lispro mix 50/50 (Mix50) versus Mix50+miglitol.
P<0.05 for Mix50+voglibose versus Mix50+miglitol.
Apo, apolipoprotein; HDL, high-density lipoprotein; IDL, intermediate-density lipoprotein; LDL, low-density lipoprotein; RLP, remnant-like particle; VLDL, very low-density lipoprotein.
Discussion
The present study demonstrated a significant effect for miglitol on 1-h PPG, remnant, and HDL-C/apo A-I concentration in T2D patients under control with Mix50. In both the randomized and crossover studies, the addition of miglitol resulted in marked suppression of 1-h PPG, resulting in almost “normal” PPG trend as seen in subjects without diabetes (Figs. 1B and 2A). 13 The results indicate that the action of insulin lispro is not sufficiently rapid to control 1-h PPG, whereas that of miglitol, but not voglibose, appears earlier than 1 h postprandial, and that the combination produces potent suppression of PPG during the entire daytime period. Supporting our results, Osonoi et al. 14 have reported that switching acarbose or voglibose to miglitol for 3 months decreases glucose fluctuations and cytokine gene expression in leukocytes of T2D patients.
Miglitol also reduced endogenous insulin secretion (C-peptide) under the use of Mix50, whereas voglibose had no such effect (Figs. 1C and D and 2B). Although voglibose is known to reduce the postprandial plasma insulin concentration when used alone, 15 this effect was masked by Mix50 in the present study. Our results indicate that the peak effect of miglitol occurs much earlier (<1 h postprandial) than that of voglibose and insulin lispro, so that the blunted PPG rise resulted in less glucose-stimulated insulin secretion. The inhibitory effect on C-peptide could be favorable for pancreatic β-cells because it can reduce glucose overload and potentially prolong β-cell life.
The postprandial effects of miglitol could be mediated through the actions of incretins on non–β-cells. It has been reported that miglitol increases postprandial secretion of glucagon-like peptide (GLP-1) in diabetes patients. 16,17 Arakawa et al. 18 also reported that administration of miglitol, but not acarbose, significantly increased active type GLP-1 at 1 h and 2 h postprandial. Based on these reports, the miglitol-induced increase in GLP-1 could have reduced 1-h PPG by suppressing gastrointestinal movement and antagonizing glucagon action in our patients.
The differential effect of the two α-GIs can be explained by their site of action in the small intestine. Miglitol is absorbed in the upper portion of the small intestine where it inhibits multiple α-glucosidases, whereas voglibose acts on the surface of the entire small intestine before it is finally discarded into the colon. 19 In addition, miglitol exhibits broad-spectrum blocking activity against α-glucosidases compared with voglibose. Miglitol also inhibits lactase (which catalyzes lactose) and trehalase (which catalyzes trehalose), in addition to maltase, isomaltase, and sucrase. 20 This feature of miglitol might have contributed to its potency under the use of Mix50.
Miglitol also had a favorable impact on postprandial lipid profile in the crossover study; it decreased plasma triglyceride and RLP-C levels and at the same time increased HDL-C and apo A-I levels (Fig. 3 and Table 2). These results were unexpected because inhibition of glucose consumption in the small intestine is not directly linked to such rapid (approximately 1 h) changes in plasma lipid profile. Postprandial triglyceride consists of the two subfractions of triglyceride-rich lipoproteins: chylomicron remnant from dietary fat and endogenous VLDL from the liver. Although the precise mechanism remains obscure, several studies have suggested the effect of carbohydrate consumption on postprandial metabolism of triglyceride-rich lipoproteins. Chen et al. 21 reported that high-carbohydrate diet leads to a postprandial rise in chylomicron remnant and increased VLDL production in patients with T2D. Picard and Deshaies 22 used an α-GI (acarbose) to show a slowdown of de novo lipogenesis from carbohydrate precursors and reduced secretion of VLDL into the circulation in rats. High-carbohydrate low-fat diet has also been shown to delay clearance of VLDL and chylomicron in human subjects. 23 Robertson et al. 24 reported that glucose consumption per se stimulates a rise in postprandial (approximately 5 h) triglyceride level. Furthermore, hyperglycemia drives hepatic VLDL production and secretion in patients with T2D. 25 Considered together, these studies suggest that miglitol could have reduced plasma triglyceride concentration by inhibiting carbohydrate consumption, which could have driven overproduction of triglyceride-rich lipoproteins and delay their clearance.
The rapid effect of miglitol on HDL-C and apo A-I was somewhat incomprehensible. Several studies have investigated the long-term effects of carbohydrates on HDL metabolism. For example, high-carbohydrate diet increases plasma triglyceride and reduces HDL-C, 26 whereas restriction of dietary carbohydrate increases HDL-C. 27 To date, only a few studies have addressed the rapid effects of carbohydrates on HDL metabolism. The effect might be mediated by cholesteryl ester transfer protein, which transfers cholesteryl ester from HDL to apo B–containing lipoproteins in exchange for triglycerides. Recently, Alssema et al. 28 reported that postprandial plasma cholesteryl ester transfer protein is increased in response to hypertriglyceridemia, resulting in reduction in HDL-C in subjects both with and without diabetes. If applied, the miglitol-induced decrease in triglyceride could have suppressed cholesteryl ester transfer protein function, resulting in the observed increase in postprandial HDL-C in the crossover study.
Incretins could have also affected the postprandial lipid profile seen with miglitol. Intravenous infusion of GLP-1 was reported to reduce postprandial triglyceride and NEFA concentrations. 29 Another study using a GLP-1 receptor agonist reported inhibition of hepatic VLDL production. 30 Thus, miglitol could have decreased postprandial remnants by altering the actions of incretin, as described previously. 16,18,31,32
The present study demonstrated the differential effects of two α-GIs on PPG and lipid profile. Although the precise mechanism of action remains to be clarified, the results can be translated into clinical practice because the efficacy of the procedures have been tested in a practical setting without serious adverse events. Further studies are needed to evaluate the long-term efficacy of this procedure against complications of diabetes.
Limitations of the study
Although each α-GI was administered only breakfast time, a possibility of residual effects of each drug could not be ruled out in the crossover study because each drug was taken every other day. A crossover study with longer washout period would guarantee the results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.