
Abstract
Objective:
This study determined if short-term (professional) blinded continuous glucose monitoring (CGM) improves hemoglobin A1c levels in a mixed group of patients with type 1 and type 2 diabetes in the clinical setting of an office practice.
Research Design and Methods:
This was a retrospective analysis of 102 consecutive patients with diabetes over the course of 10 months in a subspecialty practice undergoing 3-day blinded CGM using the iPRO™ device (Medtronic, Northridge, CA). Hemoglobin A1c levels were measured prior to and up to 7 months after the CGM procedure.
Results:
Before blinded CGM the average hemoglobin A1c level was 7.7±1.0%, and after it was 7.8±1.1%. These values are not statistically different. A subgroup analysis of subjects using continuous subcutaneous insulin infusion treatment also failed to show a significant hemoglobin A1c difference pre- and post-CGM.
Conclusions:
Using the iPro device for short-term (professional) blinded CGM in an office setting to improve hemoglobin A1c levels may not be a feasible goal for patients with type 1 and type 2 diabetes. The expectations of benefit, choice of patient, and choice of technology for short-term CGM are factors requiring careful consideration before testing takes place.
Introduction
There is a body of evidence supporting improvements in glycemic control using long-term (personal) CGM but little for short-term CGM. A multicenter study of patients with type 1 diabetes wearing a CGM device for 26 weeks showed in adults, but not in adolescents, that the CGM group achieved a significant 0.5% reduction in hemoglobin A1c levels compared with standard home glucose monitoring techniques. 1 Similar results were reported in another study of type 1 diabetes patients, but the initiation of continuous subcutaneous insulin infusion (CSII) in the CGM group adds a confounding variable to this study. 2 In distinction, a study of patients with insulin-requiring diabetes comparing self-monitoring of blood sugar versus short-duration CGM (3 days) showed no significant difference in hemoglobin A1c levels between these groups. 3 Another small study of non–insulin-requiring patients with type 2 diabetes showed that CGM did result in improved hemoglobin A1c levels, although this may have been the result of a significant drop in body mass index in the study group. 4 It remains unclear in the real-world practice setting of insulin- and non–insulin-requiring diabetes whether short-duration CGM procedures result in improved outcomes in hemoglobin A1c levels.
Our single subspecialty medical group in South Florida consists of eight endocrinologists treating adult patients. We have used short-term CGM protocols, such as those described above, for several years. We recently reviewed our accumulated experience to determine the effectiveness of short-duration blinded CGM using the iPRO™ device (Medtronic, Northridge, CA), to reduce hemoglobin A1c levels in adults with diabetes in a clinical practice setting.
Patients and Methods
The decision to pursue blinded CGM testing to improve glucose control was made by the individual endocrinologists and their patients. Because of cost considerations only patients who had insurance coverage for the procedure were tested. Published guidelines for insurance coverage in Florida for the procedure were provided by Medicare and third-party payers. This permitted inclusion of a heterogeneous group of subjects with type 2 and type 1 diabetes using treatment modalities of oral agents (one patient), insulin injection (76 patients), CSII (24 patients), and diet only (one patient). Of the insulin injection group, 55 had type 2 and 21 had type 1 diabetes, whereas in the CSII group, four had type 2 and 20 had type 1 diabetes.
Of the total group, 50 were male and 52 were female. Ethnicity was as follows: black, 15; Hispanic, six; Asian, three; American Indian, one; and white, 79.
Hemoglobin A1c levels were measured by high-performance liquid chromatography.
The iPRO device over a 3-day interval in a blinded fashion was used exclusively for CGM in all patients.
The iPRO was placed on and removed from the patient by a trained member of the office medical staff or an employee of Medtronic Inc. The information was delivered to the treating physician within a day or two of removal of the device.
During the observation period patients were managed by their respective endocrinologist according to the preferences of the individual doctor, which typically involved office follow-ups at between 1- and 3-month intervals. As an accredited American Diabetes Association Diabetic Teaching Center all patients in the practice were co-managed by our staff of five Certified Diabetes Educators, three of whom are Registered Dieticians, one Registered Nurse, and one Registered Dietician.
All subjects provided written consent to allow their medical data to be included in this study.
Comparison of hemoglobin A1c levels and body mass index before and after short-term CGM was made using the paired t test. Results are given as mean±SD values.
Results
Records of 104 consecutive adult patients with type 1 and 2 diabetes between the ages of 20 and 90 years (62.1±14.8 years) who underwent blinded CGM testing between June 2010 and March 2011 were reviewed retrospectively. Two patients were excluded because hemoglobin A1c levels obtained after CGM were thought to be too remote (8 months) to provide meaningful results.
Of the remaining 102 patients, hemoglobin A1c levels were measured from within 2 weeks to 6 months before (1.4±1.3 months) blinded short-term CGM and 1.5 months up to 7 months (3.8±1.6 months) after blinded short-term CGM (Fig. 1).
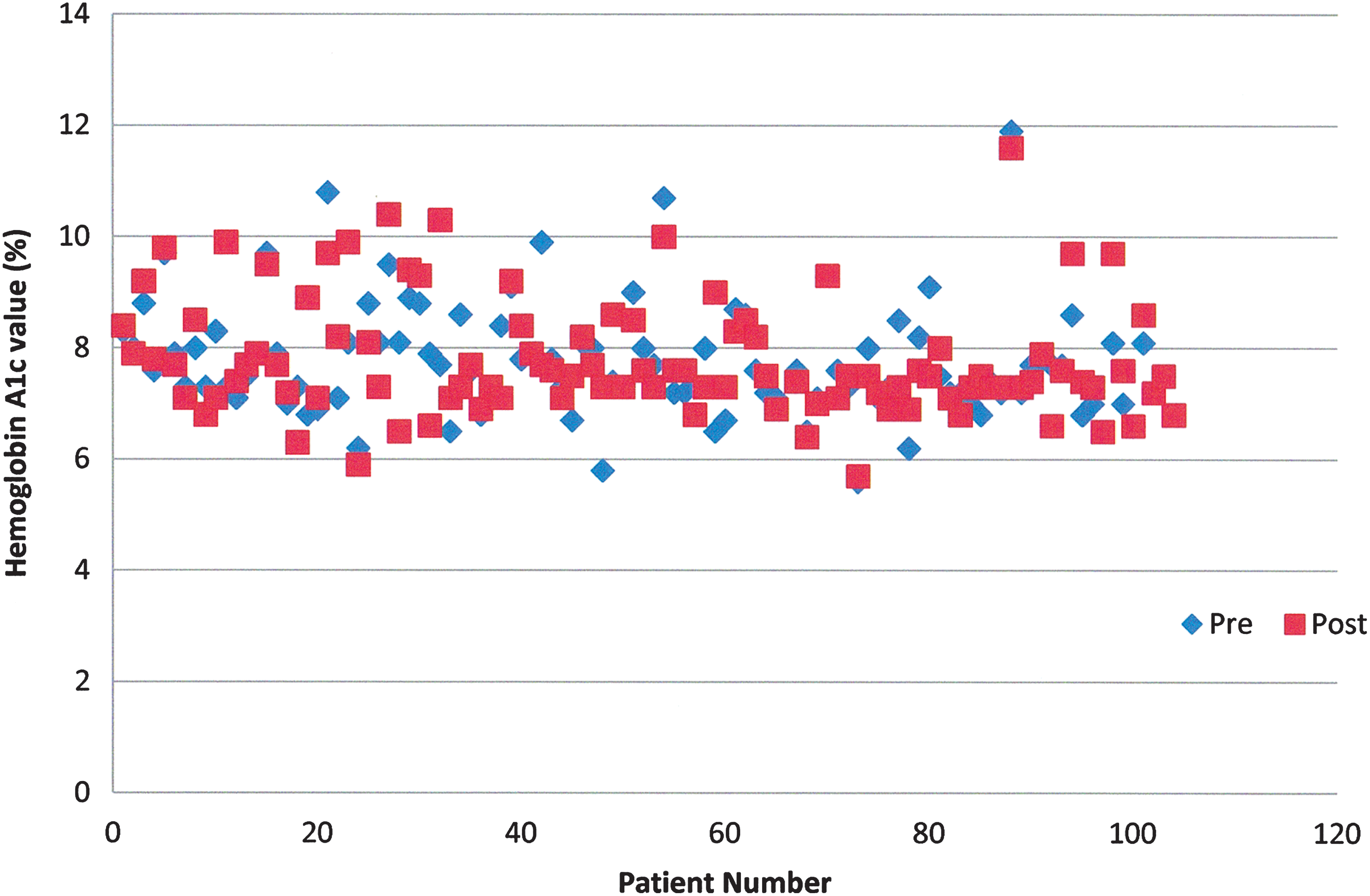
Hemoglobin A1c (glycosylated hemoglobin) before (Pre) and after (Post) continuous glucose monitoring. Color images available online at
Before blinded CGM the average hemoglobin A1c level was 7.7±1.0%, and after it was 7.8±1.1%. Body mass index was 31.6±7.8 kg/m2 pre-CGM and 31.5±7.8 kg/m2 post-CGM.
Analysis
In this group of 102 patients with diabetes, there was no statistical difference between hemoglobin A1c levels before blinded CGM testing using the iPRO device and after, based on two-tailed t test for paired variables (P=0.5). Eliminating the data of subjects over 80 years old (seven subjects) did not alter this finding. Eliminating subjects treated with diet only (one subject) and oral agent only (one subject) did not alter these findings.
Body mass index was also not statistically different pre- and post-CGM (P=0.6).
There was no correlation between the change in hemoglobin A1c levels pre- and post-procedure and initial hemoglobin A1c level (P=0.48).
A subgroup analysis of 24 patients who used CSII therapy was conducted. Although there was a trend toward improved glycemic control after blinded CGM (7.9±0.9% before CGM and 7.6±0.8% afterward), this did not reach statistical significance (P=0.13).
Analysis of the power of our study 5 reveals that it is powered at 0.85 to detect a difference of 0.3 in the hemoglobin A1c levels between pre- and post-procedure observations at a significance of 0.05.
We are unable to comment on the degree of diabetes control before the period of this study, other than that implied in the pre-CGM hemoglobin A1c level, which provides insight into glycemic control up to 3 months prior to CGM testing.
Discussion
In our retrospective study, short-term blinded CGM using the iPRO device in a private practice setting was ineffective for improving hemoglobin A1c levels in adult patients with type 1 and 2 diabetes. The heterogeneity of our study group reflects the inclusion criteria for short-term CGM provided by the maker of the CGM device and the private and Federal insurance carriers, who reimburse for this procedure. A subgroup analysis of those only using CSII therapies yielded a similar conclusion, although the small number of these patients limits our analysis.
In our study there was no correlation between initial hemoglobin A1c levels and the change in hemoglobin A1c levels pre- and post-CGM. This is particularly significant because there exists an expectation in studies of diabetes treatment modalities, including CGM technology, 6 that efficacy will be magnified at higher initial hemoglobin A1c levels.
Benefits derived from the CGM procedure extend beyond improvements in hemoglobin A1c levels. 7,8 In particular, formerly unrecognized episodes of nocturnal hypoglycemia can be detected with this technique. Obtaining information about postprandial glucose excursions, a quality of glucose control recognized to substantially impact metabolic parameters, can be a valuable objective of short-duration CGM. The overall intensity of glucose variability as it impacts clinical outcomes is an emerging target for CGM analysis. Because of the limitations of the available technology we did not attempt to compare the incidence or intensity of hypoglycemia or extent of glycemic excursions between groups.
The interval for repeat hemoglobin A1c testing after CGM in our study was variable. In clinical practice the time between completion of the CGM and institution of treatment changes responsive to the findings may vary by several weeks for individual patients. Additionally, successful implementation of the treatment changes can take place over the span of one or two office visits. We therefore believe that inclusion of post-CGM hemoglobin A1c data out to 7 months is valid.
The small number of subjects precluded our ability to break out subgroups based on anthropometric characteristics for further analysis. We do note that the subgroup using CSII showed a trend toward improved hemoglobin A1c levels after blinded CGM. Overall, however, our study was sufficiently powered to detect a change of 0.3 in the hemoglobin A1c level, which we regard as more than adequate for clinical purposes.
Limitations of the iPRO device itself may account for the failure of our practice to achieve hemoglobin A1c lowering with short-term blinded CGM. This does not preclude its potential ability to do so during long-term personal use. As pointed out by Xing et al., 9 optimal results with sensor devices may require much more intensive monitoring protocols such as 12–15 days every 3 months. In another study of subjects with type 2 diabetes using CGM intermittently over 12 weeks, a significant hemoglobin A1c decline was observed. 10 Other monitors that use sensors for longer duration in an unblinded fashion, such as that from DexCom™ (San Diego, CA), could permit more robust data acquisition with better results. In this regard, subjects with type 1 diabetes using the DexCom SEVEN® sensor for 2 weeks in an unblinded fashion showed significant improvement in multiple parameters of glycemic control. 6 It is pertinent to note that a longer duration of sensor use with the iPRO is already approved in Europe. We are aware that a second generation of the iPRO with a longer sensor life is planned by Medtronic for use in the United States.
It is tempting to use new technologies to assist in management of diabetes, but the complexities involved in regulating glycemic control in a real-life setting appear to require more than is offered by this popular device during short-term use. The potential failure of the iPRO in clinical practice to reduce hemoglobin A1c levels may waste valuable staff and monetary resources that could be directed toward more rewarding efforts.
Advancements in technology in the coming years can be expected to improve outcomes for this procedure. Until then, based on our findings our medical practice is reevaluating protocols and expectations for using short-term CGM. We are in agreement with the most recent recommendations by the American Association of Clinical Endocrinologists advising research to pinpoint patient groups which are the best candidates for CGM technology. 7 As a first step, restricting short-term blinded CGM procedures to the groups most likely to benefit such as those with frequent nocturnal hypoglycemia or as a lead-in to personal CGM use seems advisable.
Footnotes
Author Disclosure Statement
No competing financial interests exist.