
Abstract
Objective:
To our knowledge, no studies have been performed testing dose accuracy in both new and used patient insulin injection pens. We hypothesized that the dose accuracy of used (>1 year) insulin pens to be less accurate than that of new insulin pens and investigated whether possible differences influence the treatment. This study compared the dosing accuracy of 11 new and 11 used (>1 year) Novopen® 4 pens (Novo Nordisk, Bagsvaerd, Denmark).
Materials and Methods:
Dosing accuracy differences between new and used pens were studied by weighing the volume of the dosage of 8 international units of insulin (IU) and 32 IU of 11 pens. Each measurement was repeated 15 times. Whether the pens complied with the International Organization for Standardization (ISO) limits of 10% for 8 IU and 5% for 32 IU was tested. The statistical analyses were performed using the Mann–Whitney rank sum test (within Sigmaplot version 12.0; Systat Software, Chicago, IL), and a P value of <0.05 was considered to be statistically significant.
Results:
For the 8 IU dose, the mean delivered dose was 8.04 IU in new pens and 7.91 IU in used insulin pens. For the 32 IU dose, the mean delivered dose was 31.90 in new pens and 31.68 IU in used insulin pens. The difference in the median values between the two groups was statistically significant (P<0.001). Three individual doses in the 32 IU dose exceeded the ISO range in the lower range. The difference in mean variation coefficient between the two groups was also statistically significant (P<0.001).
Conclusions:
There was a significant difference between the accuracy of new versus used insulin pens. More studies with larger sample sizes are necessary to confirm our findings and further elucidate the relationship between age of insulin pens and dose accuracy.
Introduction
Materials and Methods
The Novopen® 4 (Novo Nordisk, Bagsvaerd, Denmark) is a reusable 3-mL refill pen available for injection of insulin aspart. For this experiment 11 new pens were obtained from Novo Nordisk (Alphen aan den Rijn, The Netherlands). The new pens were compared with 11 pens that had been used for over 1 year. These pens where randomly obtained from patients at our outpatient clinic.
Dosing accuracy was tested for all 22 pens according to the following protocol: to test the accuracy for a low dose the pen was set to deliver 8 international units (IU) of insulin aspart. High-dose delivery was tested by delivering 32 IU of insulin aspart. The 8 and 32 IU deliverances were alternately ejected to mimic the normal use of an insulin pen. A new needle was applied prior to every dose, strictly according to the instructions for the device. After a new pen refill was added, 4 IU of insulin was ejected and discarded to avoid any air trapping during the release of a dose of insulin. New pen refill cartridges were inserted whenever necessary. Each pen was tested 15 times for 8 IU and 15 times for the delivering of 32 IU.
A sensitive pharmaceutical balance (XS204; Mettler, Toledo, OH) was used for the assessment of the applied volumes. The results were corrected for the specific density of the insulin formulations (insulin aspart, 1.00355 g/mL measured at 20°C).
The test results were compared with the dose accuracy limits of 10% for 8 IU and 5% for 32 IU, as set forth by International Organization for Standardization (ISO) regulations (ISO 11608-1:2000). 1 The needles used for this evaluation were Novofine® 31-gauge 5-mm needles (Novo Nordisk).
Outcome measures were the dosing accuracies in both new and used pens in delivering the desired dose.
The statistical analyses were performed using the Mann–Whitney rank sum test (integrated in Sigmaplot version 12.0; Systat Software, Chicago, IL), and a P value of <0.05 was considered to be statistically significant.
Results
For the 8 IU dose, the mean delivered dose was 8.04 (±0.14) IU in new pens and 7.91 (±0.21) IU in used insulin pens. Mean dose accuracies of the 22 insulin pens for 8 IU dose were within the ISO acceptance range of 10% (7.20–8.80 IU). The individual doses for all pens also remained within the ISO acceptance range. The difference in the median values between the two groups was statistically significant (P<0.001).
For the 32 IU, the mean delivered dose was 31.90 (±0.26) IU in new pens and 31.68 (±0.41) IU in used insulin pens. Mean dose accuracies of the 22 insulin pens for 32 IU dose were within the ISO acceptance range of 5% (30.40–33.60 IU). There were three individual doses from two used pens exceeding the ISO acceptance range at the lower range (Fig. 1). The difference in the median values between the two groups was statistically significant (P<0.001). This difference still persisted after excluding the data of the two used pens exceeding the ISO acceptance range.
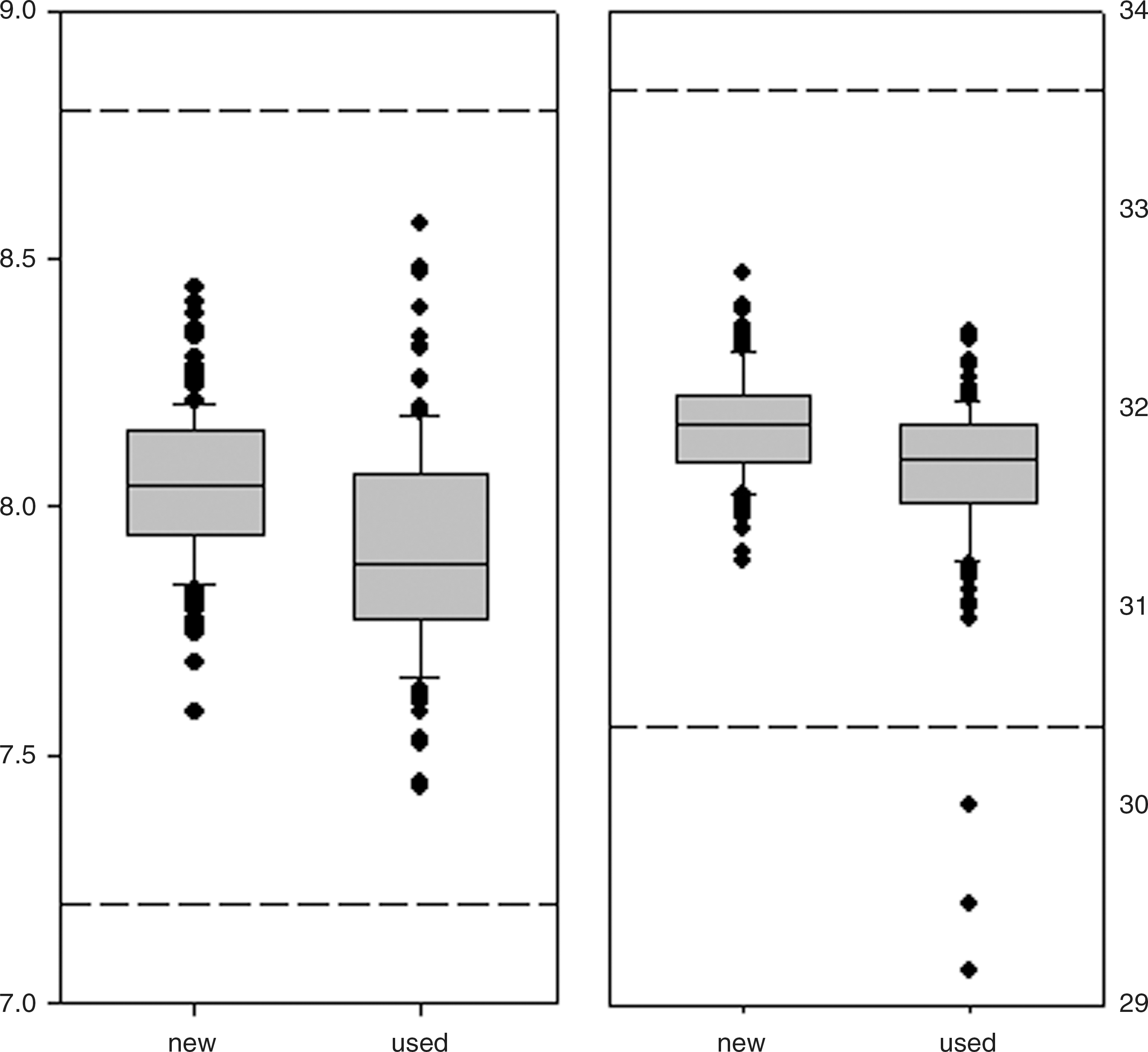
Box plots of insulin dose produced by 11 new and 11 used patient pens. The box represents median (25–75% interquartile ranges). The dots outside the 95% confidence interval are individually plotted. The dashed lines represent the range acceptable according to the International Organization for Standardization guideline 11608-1:2000. 1
The variation coefficient was calculated for all pens. For the 8 IU dose the variation coefficient was 1.85% in the new pens and 2.60% in the used insulin pens. This difference was statistically significant with P<0.001. For the 32 IU dose the mean variation coefficient was 0.82% in the new insulin pens and 1.29% in the used insulin pens. This difference was also statistically significant with P<0.001.
Discussion
There are several factors influencing insulin variability. With regard to the pharmacokinetic aspects, the absorption rate of insulin into the bloodstream is important. The absorption rate of insulin depends on injected dose and volume, injection site and depth, and factors influencing local blood flow in the subcutaneous tissue. 2 Therefore, the first step—maintaining an immaculate dosing accuracy in insulin pens—is important in the treatment of insulin-dependent diabetes mellitus. An incorrect low dose might lead to undertreatment in these patients, whereas a high dose could result in hypoglycemic events. Insulin pens undergo rigorous testing before being approved for sale. On average, manufacturers guarantee dose accuracy for 3 years. However, many patients use their pens for a longer period. Previous publications showed that newly manufactured insulin pens are accurate. 3,4 Also, previous publications studying durability of newly manufactured insulin pens have shown that insulin pens are durable in simulated lifetime use. 5,6 To our knowledge, we are the first to have conducted a study to evaluate the accuracy of newly manufactured versus pens that have been used for a period more than 1 year.
We observed that used pens deliver less insulin. We also observed that the variation of insulin delivery is higher in the used pen group. Our test was performed under ideal laboratory circumstances. In clinical practice the variability is prone to more error due to factors influencing insulin delivery as mentioned before. A clinical consequence might be that a patient switching to a new pen should be monitored more intensively. Also, the use of several pens by the same patient could lead to more variable insulin delivery. In the 32 IU dose there were three individual doses from two used pens exceeding the ISO acceptance range of 5%. In one of these pens two of the 15 measurements were outside the ISO acceptance range of 5%. This might lead to clinically relevant incorrect dosing for a patient using this pen. For instance, if this patient used his pen three times a day, this would lead to approximately six incorrect delivered doses in a 2-week period.
It is important that patients and physicians can rely on the precision of the insulin pen chosen. This is a requirement for good metabolic control. Although we found a statistical significant difference between the new and used pens, all measurements for the 8 IU dose were well within the ISO acceptance range of 10%. For the 32 IU two pens failed. The test sample size consisted of a total of 22 pens. More studies with more pens are necessary to further confirm our findings and address dose accuracy and precision in time.
Conclusions
There was a significant difference between the accuracy of new versus used insulin pens. We believe more studies with larger sample sizes are necessary to confirm our findings and further elucidate the relationship between age of insulin pens and dose accuracy in time.
Footnotes
Author Disclosure Statement
All authors have no conflicts of interest and have nothing to disclose.