
Abstract
By definition, brittle diabetes (BD) is an unstable condition. Patients with BD suffer chronically from poor metabolic control, characterized by severe instability of glycemic values with frequent and unpredictable hypoglycemic and/or diabetic ketoacidosis episodes that cannot be attributed to failure in management. Quality of life is dramatically compromised because of very frequent acute complications leading to hospital admissions and because of premature chronic complications. It remains difficult to identify all patients with BD as diagnostic criteria are still not well defined. In practice, metabolic instability is manifested most obviously by chaotic glycemic profiles, which show greater and more unpredictable variation than in “stable” patients with diabetes. It is important that patients with BD are not adequately controlled, even by closely supervised, intensive insulin regimens, including continuous subcutaneous and/or intravenous insulin infusion. Their care is often very expensive in terms of time and resources, and their lives are constantly at risk for severe metabolic derangement. Management can also be frustrating and demoralizing for everyone involved, including the patient's family as well as the diabetes care team. Adopting a team approach, involving a broad range of disciplines, is essential in treating patients with BD and helping them to achieve and maintain both normoglycemia and quality of life.
Introduction
In the current era, BD has been defined pragmatically as metabolic instability sufficient to disrupt the patient's lifestyle. Patients cannot be controlled adequately by closely supervised, intensive insulin regimens, including continuous subcutaneous, intramuscular, intravenous, and intraperitoneal insulin infusions. 4 The disruption of life, which is fundamental to the definition, depends on the patient's lifestyle and on numerous independent factors (i.e., the emergency admission policy of the diabetes and emergency care team and arbitrary limits for rates of hyper-and hypoglycemia). 4 Definitions of lifestyle disruption and “brittleness” include very frequent acute complications, leading to hospital admissions, duration of hospitalization, and precocious development of chronic complications. 3,5 The cardinal functional feature of BD remains its everyday unpredictability with unexpected hypoglycemic reactions or recurrent diabetic ketoacidosis. Nevertheless, there are no universally agreed diagnostic criteria for BD, and “brittleness” is a concept that is difficult to quantify, even if diabetologists recognize the syndrome—and can usually identify those patients whom they think are affected.
Patients with BD (three cases per 1,000 patients among the population with diabetes), mainly young women with type 1 diabetes mellitus (T1DM), suffer chronically from poor metabolic control, which cannot necessarily be attributed to patients' or clinicians' errors. 4,5 In practice, metabolic instability is manifested most obviously by chaotic glycemic profiles, which show greater and more unpredictable variation than in stable patients with diabetes. 6,7 It is notable that studies performed before the occurrence of blood glucose self-monitoring probably mix both nonacceptance of diabetes and organic or unexplained causes of BD. Therefore, with the advent of enhanced capability of self-monitoring as well as continuous glucose monitoring and the ability to anticipate rather than react to changing glycemic control, apparent brittleness may be reduced. For this reason, glucose monitor evaluations should be carefully designed and executed in order to control protocol-specific bias and random patient interferences. 8
Despite improvements in glucose control, medical care is often very expensive, with the estimated healthcare cost of a patient with BD being $1,500 per year compared with $564 per year for patients with diabetes, 9 consuming both time and resources, and lives are constantly at risk for severe metabolic derangement and complications. Fluctuation in glycemic control has been shown to contribute to pain independent of glycated hemoglobin 10,11 and what is known as the insulin neuritis syndrome. 12 Management of these patients can also be frustrating and demoralizing for patients, their families, and the entire diabetes care team. They demand the ultimate in resourcefulness of their healthcare provider team.
This review focuses on a clinical approach to recognition of BD, unraveling its mechanisms and translation of the ongoing research into its pathophysiologic mechanisms into clinical care. In addition, attention is drawn to the common and life-threatening clinical manifestations, their diagnosis, and treatment. An electronic literature search of the Medline (via PubMed) and ScienceDirect (via SciVerse) databases without date limitations was conducted for this article. Combinations of the following key words were used: “brittle,” “unstable,” “stable,” “diabetes,” “type 1,” “type 2,” “glucose,” “insulin,” “monitor,” “continuous,” “diagnosis,” “etiological,” “causes,” “clinical,” “manifestations,” “complications,” “recurrent,” “ketoacidosis,” “hypoglycemia,” “treatment,” “outcome,” “pancreas,” “transplant,” “islet,” “cell,” and “pump.” All types of articles published in English were included and studied in full. Studies published in languages other than English were only considered in abstract form. We retrieved 289 studies by hand-searching, and 127 met the criteria of sufficient evidence-based information to be able to draw conclusions applicable to adaptation into routine clinical care. The last search was run on April 6, 2012.
Etiological Basis of “Brittleness”
Causes of “brittleness” include obesity and physical inactivity with the interplay of diet imbalance, impaired insulin sensitivity, and decreased glucose removal in the skeletal muscles, 13 puberty, 14 and defects of counterregulation by hyperglycemic hormones, 15 –18 infections, 7 drugs, 19 –21 and psychiatric and psychological problems, 3 as well as delayed gastric emptying due to autonomic neuropathy. 22
The stomach is an important regulator of blood glucose levels, and early in the course of diabetes the rate of gastric emptying is enhanced. 23 Under normal circumstances the ingestion of food slows the rate of gastric emptying, a process mediated by the release of human islet amyloid polypeptide. 24 This in turn slows the rate of gastric emptying, preventing dumping of nutrients into the duodenum and the rapid absorption leading to wide swings in blood glucose. 25 In T1DM the secretion of human islet amyloid polypeptide may be dysfunctional with the potential of a loss in this naturally occurring brake mechanism. 22 These pathophysiological pathways are summarized in Figure 1.

Regulation of gastric emptying. Ach, acetylcholine; CCK, cholecystokinin; GIP, glucose-dependent insulinotropic peptide; GLP-1, glucagon-like peptide 1; hIAPP, human islet amyloid pancreatic peptide; NANC, nonadrenergic noncholinergic; NO, nitric oxide; PYY, peptide YY. Reprinted with permission from Vinik et al.
22
Color images available online at
Other potential causes are organic problems involved in hypoglycemia unawareness due to autonomic dysfunction or failing central nervous system recognition, 26 hypoglycemia unresponsiveness with defective counterregulation due to impaired hormonal secretion, 27 and loss of central dopaminergic mechanisms regulating the autonomic nervous system. 28 Other factors may contribute such as alcohol abuse, renal failure, senile dementia, and eating disorders. 29,30
Variable adherence to insulin treatment contributes to presentation of BD in adolescents and young adults. 31 Direct evidence of poor compliance with insulin therapy in young patients with T1DM is a major factor that contributes to recurrent diabetic ketoacidosis. Insulin requirements exceeding 2.0 U/kg/day frequently are suggestive of BD. Causes of apparent or genuine insulin resistance in patients with T1DM include puberty, 32 overinsulinization, 33,34 chronic diabetes infections, 35 and endocrinopathies. 36 –40 Intestinal malabsorption, including celiac disease, often associated with T1DM (in one in six patients) and easily recognized with antibody measurements (i.e., transglutaminase 41 ), can also cause decreased insulin requirements and provoke unexpected and sometimes severe hypoglycemia. 42
Depression and manipulation represent important factors contributing to instability. 31,32,43 Psychosocial factors include family dysfunction, obsessively rigorous diabetes control, and anorexia nervosa. 31 –33 Suggested motives include escape from hostile situations to hospital security, attention-seeking, self- or family revenge, and suicidal intent. Furthermore, some patients induce hypoglycemia to “feel high.” 30,32 More rarely, cases of factitious overdose whereby insulin was given in excessive doses by a mother thwarted or in need of attention to her child with diabetes, known as “malingering or Munchhausen by proxy,” have been reported as well. 44
Acute and everyday life psychological stress contributes to glycemic instability of patients with BD through an increased secretion of insulin-counteracting hormones. Psychological interviews have shown that most patients with BD perceive a link between life stress and glucose control and have considerably greater difficulty in giving verbal expression to their emotions. 32,33 Patients with BD display distinct cardiovascular and neuroendocrine responses to psychological stress, as well as distinct psychological profiles. 45
Psychosocial parameters interact with metabolic instability even in juvenile BD. Feelings of dominance, depression, anger, and body symptoms are associated with metabolic instability. 31,32 Everyday life can greatly affect blood glucose control. Stressors such as divorce, family arguments, violence, or abuse can lead to elevated blood glucose levels and increase the need for intervention by a supportive healthcare team. 31,32 Schizophrenia has been associated with BD in young female patients with hypothyroidism, in which antipsychotic medication resolves “brittleness.” 46
In autoimmune polyendocrinopathy with candidiasis and ectodermal dystrophy, autoimmune destruction of the pancreatic β-cells with slow development of juvenile BD and early onset of severe complications is possible. 47 Young female patients and their maternal relatives need long-term follow-up in order to evaluate the function of endocrine glands and to initiate early treatment for hormonal deficits, as well as to detect the nonendocrine components of the disease.
The highest frequency of BD is seen at 15–30 years, although a second smaller peak at 60–70 years is also encountered. 48 Causes for this second peak include systemic disease (14%), hypoglycemic unawareness (6%), and memory or behavioral problems (8%). BD in older (≥70 years) patients with a history of human recombinant insulin therapy has been attributed to increased insulin resistance. 49 BD in the elderly is most frequently characterized by recurrent hypoglycemia, and its contributing factors are chronic, non-diabetes diseases. 50 Unrecognized celiac disease causes recurrent hypoglycemia, which is ameliorated by adherence to a gluten-free diet, when coexisting colorectal disease is ruled out. In view of the fact that 19% of patients with adult celiac disease are older than 60 years, the two conditions may be associated with each other in older age as well. 50 Furthermore, in the presence of otherwise unexplained BD, the coexistence of iron-deficiency anemia should give rise to suspicion of celiac disease because it is its commonest extraintestinal manifestation. 50
BD in older patients (>80 years) with diabetes is thought to be a depletion of endogenous insulin secretion due to marked β-cell reduction and/or β-cell exhaustion secondary to long-standing diabetes. Its main feature is frequent profound hypoglycemia without clinical awareness. These patients often present with vascular dementia, visual disturbances, hearing difficulties, and speech and motor disorders. 50 There is increasing evidence for a role of interactions of advanced glycation end-products and their receptor, leading to formation of cerebral amyloid fibrils and early cognitive decline culminating in dementia. 50 Cognitive decline is greater in females than males.
Diabetes after total pancreatectomy is commonly described as “brittle.” 51 BD is also frequently developed in chronic pancreatitis after partial pancreatectomy, and its development is related to reduced pancreatic β-cell area, preoperative glycemic control, and obesity. 51 This is highlighted by the unequal impact of different surgical procedures on glucose control. 51 It has also been attributed to the loss of glucagon secretion and to fat malabsorption in chronic pancreatitis and pancreatectomy. 52 These patients tend to be exquisitely insulin sensitive, and tiny adjustments in insulin dosing may be necessary such as ½ or 1 unit at a time. 53 A patient's malnutrition and inadequate diabetes management also demand attention. 51,52
In some patients, there is no obvious cause. Most patients with “idiopathic” BD have no obvious underlying mechanism. Nonetheless, organic causes of BD are occasionally found and must always be sought. Figure 2 illustrates the different clinical forms of BD and their causes. The most common causes of BD and their respective frequencies are listed in Table 1.
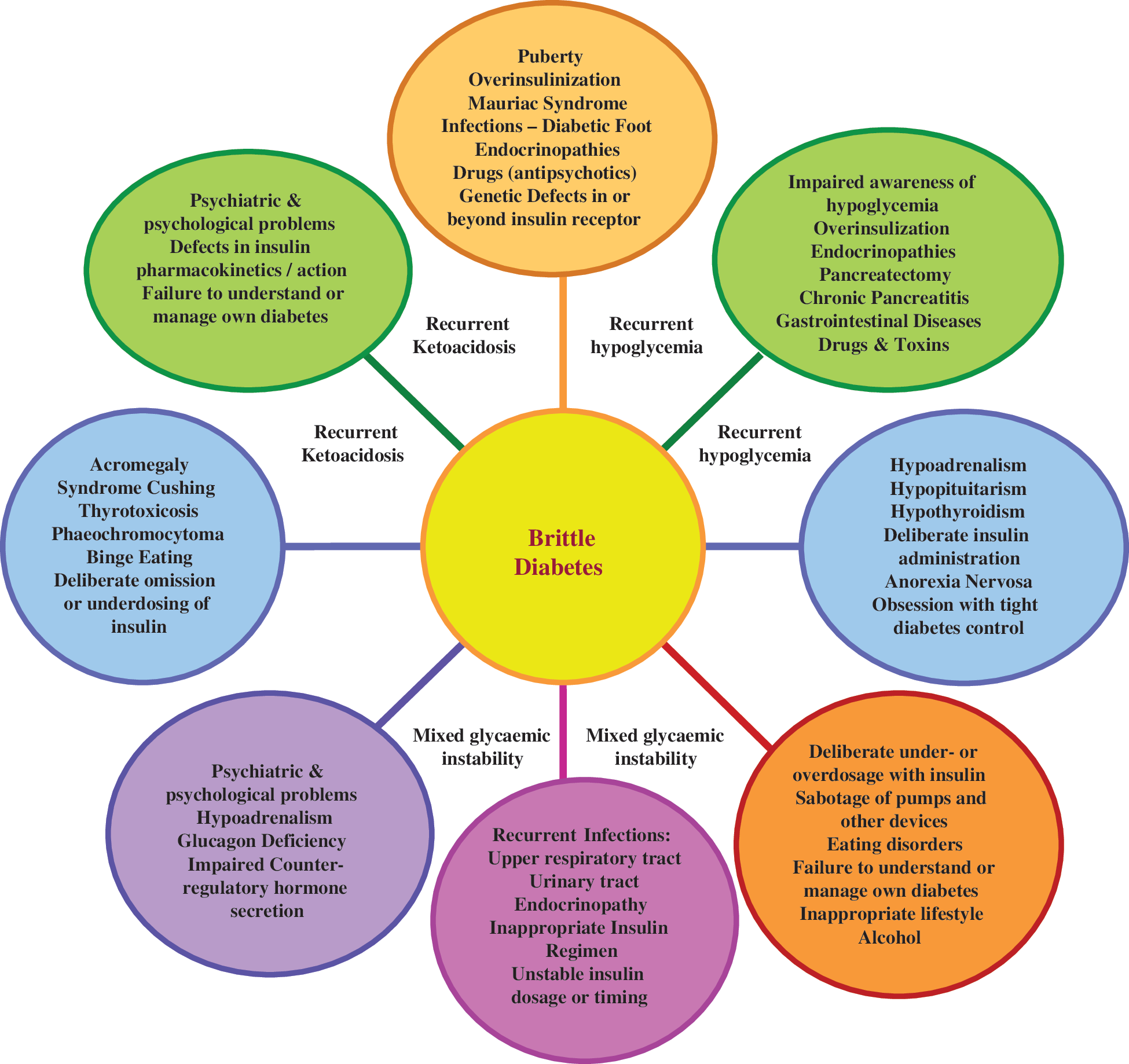
Causes of brittle diabetes. Color images available online at
Diagnosis of BD
There are no universally agreed-upon diagnostic criteria. Three forms of BD have been described: recurrent diabetic ketoacidosis (59% of the total BD spectrum), predominant hypoglycemia (17%), and mixed instability (24%). Previous studies have shown that over 90% of hospital admissions in patients with recurrent diabetic ketoacidosis or hypoglycemia are due to BD. 2,4,48 In comparison with patients with recurrent diabetic ketoacidosis, hypoglycemic BD patients are significantly older and are of approximately equal male:female ratio, compared with a female excess in recurrent diabetic ketoacidosis. 2,4,48 Patients with mixed BD are intermediate in age and sex ratio, compared with the other two groups. Patients with idiopathic BD usually display a pattern of hyperglycemia with wide glycemic swings and recurrent episodes of ketoacidosis. 2,4,48
Several measures have been developed to objectify and, possibly, quantify metabolic instability in BD. These include assessment of mean amplitude of (largest) glycemic excursions, 54 mean of daily differences, 55 and continuous blood glucose monitoring. 56 These are easier evaluated with the computer software for new continuous glucose monitoring (CGM) systems. 57 Typical values for measures of glycemic profiles in BD are shown in Table 2.
BD, brittle diabetes; BG, blood glucose; BGM, blood glucose meter; CGM continuous glucose monitoring.
Accurate and reliable CGM systems may facilitate specific therapeutic adjustments that need to be made to avoid hypo- and hyperglycemic excursions, thereby improving metabolic control. 58 Those patients with BD who are motivated to participate in their diabetes care and are familiar with technology may benefit from CGM systems. 59 In addition, CGM systems can serve as a tool to predict impending glucose excursions, thus providing alarm signals of hypo- and/or hyperglycemic values and warning the patient to take preventative actions. 60 Quality of life may also improve by using CGM systems via reducing the fear of hypoglycemia and promoting self-confidence. 60
However, to successfully implement CGM systems in daily practice, these devices must be accurate and reliable, and one must be aware of the limitations of currently available systems. These limitations originate from physiological differences (i.e., differences between glucose variations) in the interstitial tissue, where CGM device measuring is done, compared with blood, where calibrations are performed, and technical aspects such as defects in the reproducibility and the premature curtailments of recordings. 60 New closed-loop devices in which CGM systems are integrated with pump therapy in order to more closely mimic the human pancreas may significantly improve patient acceptance of intensive therapy, glycemic control, and quality of life in patients with BD. 61
Diagnostic work-up
A scheme for investigating patients suspected for BD is suggested in Figure 3. Diagnostic work-up should initially include a thorough history and examination that may reveal drug-induced causes, infections (i.e., diabetic foot, periodontitis and odontogenic infections, pneumonia and asthma, and acquired gastric and bacteremic urinary tract infections), or endocrine conditions, including puberty. Before resorting to more detailed investigations, it is vital to assess the patient's awareness of diabetes monitoring and treatment. Clinicians should further inspect for defective diabetes equipment and for hypertrophic or atrophic cutaneous sites of insulin administration. If necessary, insulin antibodies and insulin receptor antibodies should be measured. A hormonal profile and measurement of C-peptide to evaluate residual β-cell function are warranted. Should no cause for insulin resistance or sensitivity emerge, the possibility of factitious “insulin resistance” needs to be explored, and an “insulin challenge” test should be performed. Rises in plasma insulin concentrations and corresponding falls in blood glucose should be determined following test doses of insulin (0.1 U/kg) injected subcutaneously or intravenously by doctors under conditions that guarantee the patient's cooperation. Autonomic function tests should be performed 62 and in most instances should be accompanied by a solid or nutrient liquid meal gastric emptying study, as a surrogate for gastroparesis. 63,64 Most patients who remain undiagnosed at this stage probably have factitious disease and may be adept in manipulating their treatment, families, and physicians. Hospital admission in such cases can provide formal psychological and psychiatric assessment of the patient and family, without which investigation and management are incomplete. An etiological work-up of confirmed BD is presented in Figure 4.
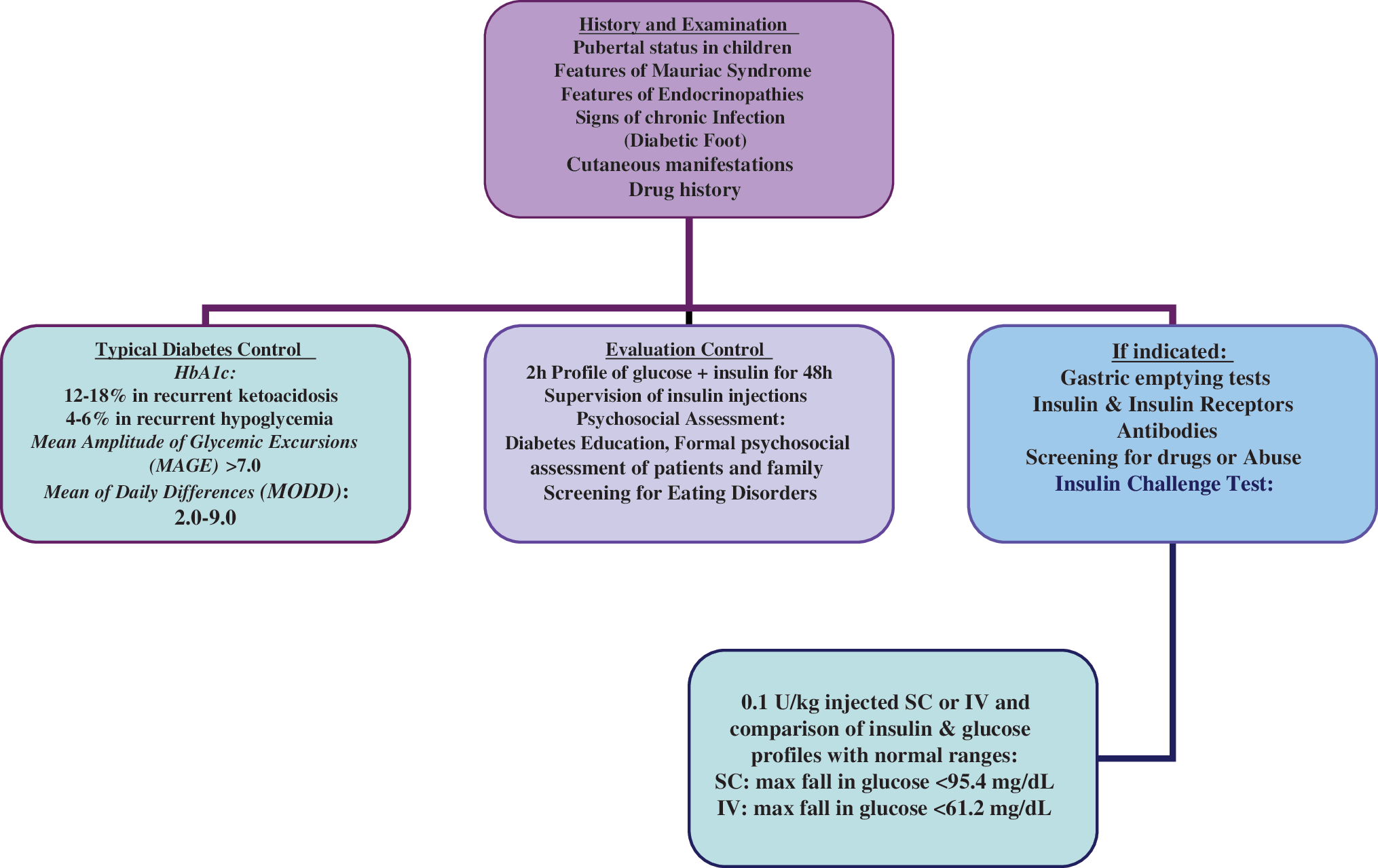
Scheme for investigation of brittle diabetes. HbA1c, glycated hemoglobin; IV, intravenously; SC, subcutaneously. Color images available online at
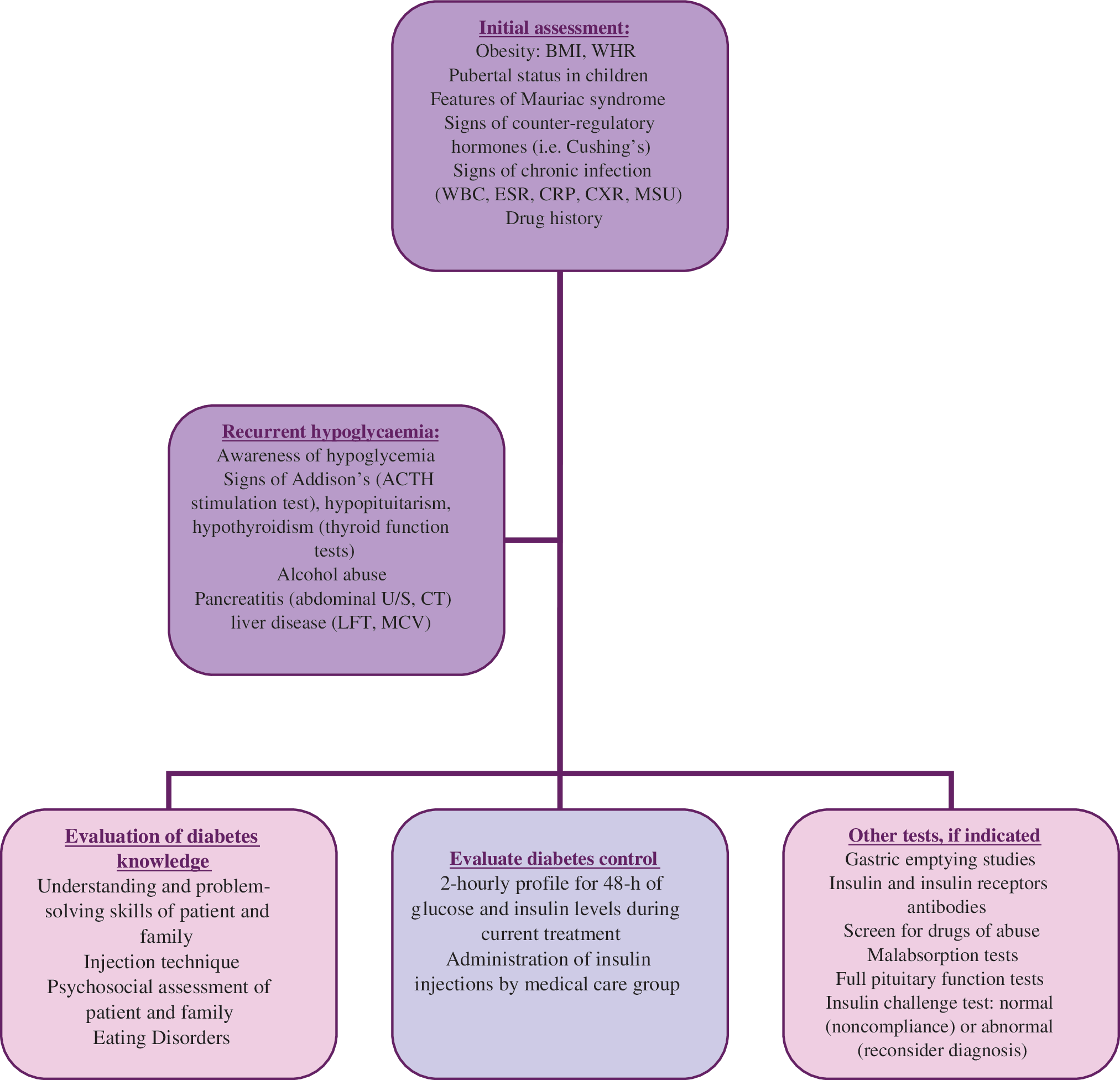
Etiological work-up of confirmed brittle diabetes. ACTH, adrenocorticotrophic hormone; BMI, body mass index; CRP, C-reactive protein; CT, computerized tomography; CXR, chest X-ray; ESR, erythrocyte sedimentation rate; LFT, liver function tests; MCV, mean corpuscular volume; MSU, midstream urine culture; U/S, ultrasound; WBC, white blood cell count; WHR, waist-to-hip ratio. Color images available online at
Complications of BD
Complications of BD include persistent hyperglycemia and ketoacidosis (59%), recurrent hypoglycemia (17%), and mixed glycemic instability (24%). Proteinuria occurs in 20% of patients with BD leading to renal impairment (30%) and end-stage renal failure (10%). Retinopathy and laser treatment are more frequent (60%) in BD compared with T1DM patients (25%). 4 Patients with BD and retinopathy are more often visually impaired compared with those without BD (20% vs. 10%). 5 Furthermore, painful and autonomic neuropathy is five times more common in the BD group. 5
A rare complication of long-term diabetes that, however, occurs more commonly in BD is spontaneous muscle infarction. Diabetic muscle infarction is more frequent in young (≤30 years) women with brittle T1DM of short duration (≤5 years) (61.5%). 65,66 Diabetes complications are often present: 71% of patients with BD have nephropathy, 57% have retinopathy, and 54% suffer from autonomic neuropathy. 66 Spontaneous diabetic muscle infarction is usually acute, with pain and swelling localized to the thigh in most instances, and the diagnosis is suggested by magnetic resonance imaging. Management consists of resting the muscle, analgesics, and gradual mobilization. Recurrence is common and may be seen in more than 50% of the patients with BD. 66
Patients with BD are terrified and resist with psychotic-type defense reactions the common psychotherapeutic experiences, which are important parts of the integration of an individual's mental organization. These reactions are always activated by separation and may appear prior to any developmental step (i.e., in recognizing self-boundaries, sexual identity, and facing the oedipal conflict). On all these occasions, deep regression, suicidal feelings, and mistreatment of diabetes usually appear. 3,4,32,43,48
Patients with long-standing BD with numerous episodes of diabetic ketoacidosis and hypoglycemia may exhibit significant pathological changes in the gastric wall that affect all major components, including muscle, neurons, and interstitial Cajal cells. Gastroparesis and severe malnutrition may occur, in association with vagal, central, or hormonal perturbations. 67 Recent studies have demonstrated a loss in neuropeptides and nitrergic innervation in the stomach 68 and alterations in circulating levels of motilin and pancreatic polypeptides involved in gastric motility 69 and have resulted in novel treatments, including the use of cyclic GMP phosphodiesterase inhibitors as well as ghrelin, which is now approved for intravenous use in severe gastroparesis. 22
Inhibition of periodontal ligament cells is the key explanation for delayed periodontal regeneration and healing in patients with BD with recurrent diabetic ketoacidosis. 70 As a result, patients develop more frequent infections extending to more distant structures via direct and distant spread (i.e., intracranial, retropharyngeal, and pulmonary pleural infections). Further hematogenous dissemination may lead to primary rheumatic fever, arthritis, and secondary deposits on the heart valves (i.e., endocarditis). 70
Pulmonary edema, cerebral edema, and multiple brain and/or cervical spinal cord infarctions develop frequently in BD during diabetic ketoacidosis, despite appropriate treatment. This may result in spastic quadriparesis and permanent disability. 71 Finally, cutaneous manifestations of BD include fat hypertrophy, diabetic dermopathy, scleroderma adultorum, and acanthosis nigricans. 72 These manifestations are also common in poorly controlled diabetes and insulin-resistant states. As mentioned earlier, injection of insulin into a hypertrophic or atrophic site may indeed be the cause of BD.
BD: Endless Struggling Toward Improved Quality of Life?
Patients' usual lifestyle and admission policy of diabetes care providers are the main factors influencing the impact on quality of life. Emergency admissions due to poor metabolic control are much more common and prolonged, and it is not unusual for patients with BD to spend several months per year in hospital. Lifestyle disruption is mainly induced by frequency and duration of hospitalization, more frequent psychosocial disruptions, pregnancy complications, and a higher risk of death due to diabetes complications. 5,73
Epidemiological studies in patients with BD have established higher prevalence rates of psychiatric disorders, in particular, mood and anxiety disorders. 3,4,43,48 Health-related quality of life is among the benefits of islet cell transplantation (ICT) because of a significant improvement in the dimensions of satisfaction and impact of diabetes. 74 Indeed, recent studies report up to 56–60% resolution of BD by ICT. 74 Therefore, its assessment may help in the selection of candidates with BD for islet transplantation.
Treatment Options
Therapy of BD is based on education, glycemic control, intensive treatment, and close collaboration among physicians, healthcare providers, and patients. Once psychogenic problems have been excluded, therapeutic strategies should have two main aims. First, they should address underlying organic causes of BD whenever possible, and, second, they should optimize standard insulin therapy using analogs, multiple injections, and even continuous subcutaneous insulin infusion (CSII), as individually required. 75 However, a minority of BD patients are resistant to therapy, and new algorithms are needed. 5,61 As previously mentioned, in such patients, pancreas or islet transplantation represents an effective therapeutic option, entailing good expected outcomes.
Lifestyle and education
Reduction of the rate of severe hypoglycemia has been noted with the Dose Adjustment for Normal Eating approach, resulting in improved long-term metabolic control and better adherence to treatment goals. 76
The patient's ability to manage his or her own diabetes should be evaluated, and guidelines should be created with the patient's agreement for future treatment targets and follow-up. Any clinically meaningful suggestions should be discussed in depth with the patient and family. Patients should be educated on self-management and insulin dose adjustments because a main cause of BD is failure of the patient to understand or manage his or her own diabetes. Effective education should provide knowledge in a conceivable way, respecting both the unpredictability and complexity of actual life and the patient's individuality. 77 Ideally, education should not merely reproduce information, but endeavor to offer assimilated knowledge and promote behavior changes. 77 The doctor assigned to investigate and treat the patient should be easily available by telephone to advise the patient and his or her family because on-demand consultation may be able to avert hospital admissions. 78 Especially for low-income families, limited access to health providers and high costs of healthcare affect diabetes control and family stability. 78
Glycemic control is significantly correlated with the patient's well-being, 79 and contributing factors to glycemic instability should be carefully evaluated and addressed. In recurrent hypoglycemia, all patients and their families should be educated on prevention and treatment of hypoglycemia. Moreover, appropriate information about hypoglycemia unawareness should be provided on diagnosis and regularly thereafter. Patients should be constantly reminded to avoid usual activities that may contribute to hypoglycemia, such as taking excess insulin, delaying or missing meals, wrong timing of insulin/food intake in the event of exercise, not monitoring before bed, etc. Patients should be educated to avoid excessive feeding after a hypoglycemic episode leading to rebound postmeal hyperglycemia, which would require a higher administered insulin dose for correction, directing to yet another hypoglycemic swing with the hypersecretion of counterregulatory hormones inducing a vicious circle. 80 Alcohol consumption can also lead to hypoglycemia and impair recovery from a hypoglycemic episode; all patients should be emphatically reminded not to omit food when drinking. Additionally, patients should be advised to have a glucagon injection close by for any severe hypoglycemia episode. 78
Management of gastroparesis has several goals, including restoration of hydration, nutrition, preferably by the enteral route, correction of electrolyte, glycemic imbalances, reduction of vomiting with anti-emetic agents, enhancing of gastric emptying with prokinetic agents, and pain relief without narcotics. Recently, new algorithms have been provided on the use of treatments based on severity of symptoms, degree of delay of gastric emptying, and ability to maintain hydration and nutrition by the oral route. 81 Gastric electrical stimulation by the delivery of high-frequency electrical stimulation to the stomach has showed improvement in symptoms, reduced need for nutritional support, and increased quality of life, 82 whereas in patients with significant upper gastrointestinal motility disorders, surgically placed venting gastrostomy reduced the hospitalization rate during the year after placement. 83 In seriously affected patients where risk of subsequent renal failure is high and where life expectancy is poor, major gastric surgery can effectively relieve distressing vomiting from severe gastroparesis and improve quality of life. 84
Although hypoglycemia avoidance restores awareness, it is difficult to maintain. Hypoglycemia unawareness increases severe hypoglycemia risk. When adherence to treatment changes is adjusted to awareness status, there is evidence that unawareness can be linked even with only one severe hypoglycemic episode that impairs hormonal counterregulation or with the acclimatization to a chronically hypoglycemic milieu. 85 Hypoglycemia unawareness in T1DM is largely secondary to recurrent hypoglycemia in the context of strict metabolic control. 86 Reduced awareness of hypoglycemia in some patients with overzealous glycemic control may be partially restored by reducing insulin dosages, even if this occurs at a slight increase of mean blood glucose and glycated hemoglobin. 87 Fortunately, hypoglycemia unawareness in T1DM is largely reversible. Indeed, appropriate insulin therapy along with education may ameliorate hypoglycemia without endangering glycemic targets in BD. Therapies aimed at reversing repetitive harmful behavior may also be useful to restore hypoglycemia awareness. Hypoglycemia awareness training has been used successfully. 88
Psychotherapy
Proven noncompliance to treatment requires careful handling. 4,48 Inpatient problem-oriented psychotherapy of patients with BD and psychic reactions significantly stabilizes and improves glycemic control and noncompliance to treatment, leading to patient rehabilitation. 3,4,32,48 Although the ambulatory psychological treatment of BD is less encouraging, 89 frequent (three or four times a week) psychoanalytic therapy is highly effective in improving diabetes management. 90
Family plays the key role in the adjustment of children and adolescents to diabetes, and the impact of diabetes depends on both the patient's and the family's perceptions and knowledge of self-care and self-management. In younger patients with BD, family psychotherapy is recommended and should further focus on specific conditions (i.e., involvement of the patient in parental conflict and physiological vulnerability that encourages somatization). 91
When factitious BD is suspected, long-term psychiatric follow-up is often necessary before the motives that the patient prefers to remain in a “patient” status rather than return to a normal lifestyle are revealed. 92 Cognitive analytical therapy is further promising than more conventional approaches in the exclusion of disease manipulation motives such as avoiding work, school, or the responsibilities of life, which are common in patients with BD. 92 Successful cases with cognitive analytical therapy have been reported in the management of depression and anxiety that may affect diabetes self-care by reducing the patient's ability to carry out the necessary day-to-day adjustments for good control. Cognitive analytical therapy was successful also in the resolution of adolescent psychological conflicts regarding life dependency and day-care autonomy, which can be played out against diabetes control. 93
Because diabetes is often the perfect vehicle through which unresolved conflicts and relationship difficulties are channeled, psychotherapy should attempt to change self-care behavior in ways that also consider fundamental experiences and will enable patients to use what they know, after contact with the therapist has ceased.
Insulin therapy
Several different methods of insulin administration have been attempted but have failed to achieve metabolic control in the long term in patients with BD. 94 Although failure to respond to CSII has been used as a diagnostic criterion for BD, 94 CSII may, however, improve diabetes control in patients disabled by recurrent hypoglycemia. 95 –97 Single cases of brittle T1DM in which recurrent hypoglycemia and peripheral edema were relieved after conversion from the rapid-acting insulin analog insulin lispro to insulin aspart have been reported. 98 Fewer symptomatic episodes of hypoglycemia with insulin aspart than with insulin lispro administered by CSII have also been demonstrated. 99 Finally, emergency admissions with ketoacidosis have been virtually abolished in some cases of BD with implanted pumps delivering insulin to either a central vein or the peritoneal cavity. 100 Metabolic control may even be restored to the point where the patient can return to normal daily activity (i.e., work or school). 101
Nonetheless, patients with BD do not always reach this objective, and factors influencing glycemic instability in BD appear to be independent of treatment modality. 102,103 In addition to the usual reasons affecting all patients with diabetes, in BD the main obstacle preventing patients from reaching optimal glycemic targets is often related to difficulties in self-regulation, denial of diabetes, or phobia of hypoglycemia with resultant dose reduction and/or avoidance of insulin. 4,104 Physicians may also contribute by assigning too strict glycemic targets, which may be inaccessible for the patient, and so promote hypoglycemia episodes or even a sense of guilt in case of failure to achieve them. 104
Insulin pump therapy
Insulin pumps are now being increasingly used because of their unique ability to continuously infuse insulin, closely mimicking that of physiological pancreatic secretion. Unlike insulin shots with syringes, pump infusion sites need to be changed less frequently. Insulin pump therapy (IPT) is reported to improve glycemic control, reduce glycemic swings, and the dawn phenomenon. 105 Fewer hypoglycemic episodes and a reduction in daily insulin requirements are reported with IPT as well as an improvement in sexual function, libido, and a significant relief of the intractable pain of peripheral neuropathy. 10 –12 Quality of life is ameliorated by the reduced chronic fear of severe hypoglycemia, the more flexible and free lifestyle, and easier participation in social and physical activity. 61 In BD, IPT has been shown to yield favorable results in terms of metabolic control when used in young subjects, including children ≤6 years. 106 Finally, in both adults and children with brittle T1DM, sensor-augmented IPT resulted in significant improvement in glycated hemoglobin levels compared with injection therapy. 107
Pancreas transplantation
The current annual rate of pancreas transplants performed worldwide is about 1,500. 108 The survival of functional grafts with complete insulin independence is better with simultaneous pancreas–kidney grafts (approximately 85% at 1 year) compared with pancreas-alone transplant (approximately 60% at 1 year), although the latter can be improved with selected patients and appropriate immunosuppressive regiments. 108,109 Recent advantages that have reduced the morbidity of pancreas transplantation are enteric exocrine drainage, primary portal-venous graft drainage and immunosuppression with combined tacrolimus and mycophenolate, and post-transplant monitoring for rejection with serum amylase and lipase measurements. 110
Patient survival improves by at least 10% by 5 years and by up to 59% at 10 years following combined pancreas–kidney transplantation, compared with kidney-alone transplantation in brittle T1DM patients. 111,112 Freedom from insulin, blood glucose monitoring, and dietary restriction improve the overall quality of life for the BD patient undergoing successful pancreas transplantation. 113 Simultaneous pancreas–kidney transplantation is protective to the kidney and prevents recurrence of diabetic nephropathy. 114 Progression of peripheral and autonomic neuropathy may be completely reversed by successful pancreas transplantation, even if polyneuropathy is advanced. 115,116 Recovery of gastroparesis and restoration of hypoglycemia awareness have also been demonstrated. 117 The course of diabetic retinopathy is less favorably influenced by pancreas transplantation, as proliferative change and macular scarring have already occurred. 118 The impact of pancreas transplantation on atherogenesis, cerebrovascular disease, and cardiovascular mortality, when applied earlier in the course of diabetes, remains to be established.
ICT
ICT is an attractive concept for the treatment of brittle T1DM. Recent studies have demonstrated that it is a relatively noninvasive alternative to pancreas transplantation for restoring endogenous insulin secretion, resulting in a marked reduction in hypoglycemic episodes in patients experiencing hypoglycemic unawareness, and improving glycemic control as well as glucose variability. 119,120 ICT should be considered in cases of hypoglycemic unawareness (i.e., onset not felt with glucose <54 mg/dL) and/or metabolic lability (i.e., two or more severe hypoglycemic or ketoacidosis episodes requiring third-party assistance within 1 year). Moreover, patients with T1DM duration of >5 years and progression of diabetes complications (i.e., retinopathy, early nephropathy, and neuropathy that persisted despite optimization of insulin regimen) should also be considered for ICT. 113 ICT should be considered in cases of BD patients <65 years old with a body mass index ideally <25 kg/m2, without reported psychiatric disease or nonadherence to therapy, with normal renal function and preferably no plans for pregnancy. 113
In ICT patients, health-related quality of life was significantly improved at 6 months and remained so at 12 months post-transplantation because of a significant improvement in the dimensions of satisfaction and impact of diabetes, including physical and social functioning, role-physical, bodily pain, and general health. 74 The main limiting factor of ICT is the potentially severe side effects of the immunosuppressant therapy necessary to avoid graft rejection and recurrence of autoimmunity and the burden of maintaining or resuming insulin therapy. 120,121 However, an increased percentage (>55%) of insulin independence at 1-year post-transplant and a decreased percentage of new-onset cardiovascular events have been achieved with corticosteroid-sparing protocols in ICT and BD. 122 Although only a minority (10%) of BD patients remain insulin-free after 5 years, more than 80% of them had still detectable levels of C-peptide and substantially improved glycemic control without episodes of hypoglycemia. 122
Other limitations to the widespread application of ICT in patients with BD include the need for several donors for sufficient islet yield and the loss of islet function over time due to incompletely defined reasons. 123 Recently, in patients with BD, allogeneic islet transplantation was performed with the addition of exenatide and a short course of tumor necrosis factor-α blockade. This protocol was successfully associated with a significantly lower number of islets required initially to achieve insulin independence. Although further studies are needed, exenatide improved islet graft function and facilitated achievement of insulin independence with fewer islets, thus decreasing the need for multiple donors. Nevertheless, it did not lead to a measurable increase in functional islet mass over time. 124
Even though currently the islet graft is still not a remedy for every patient with BD, 122,125 ICT is close to having a biological license status approved by the Food and Drug Administration in the United States that would further stimulate progress in the field. 126 Finally, β-cell regeneration from naive pancreas and from embryonic stem cells or induced pluripotent stem cells is poised as the next-generation treatments for BD. 120,125 In this context, the effects of islet neogenesis-associated protein pentadecapeptide on proliferation and secretion function of β-cells were recently evaluated with most promising results. Islet neogenesis-associated protein pentadecapeptide increased the insulin secretion, enhanced the proliferation, and reduced the apoptosis of β-cells. 127
Conclusions
BD has been defined as metabolic instability sufficient to disturb the patient's life. Poor diabetes control and recurrent episodes of hyperglycemia with ketoacidosis and/or hypoglycemia are the main features. Female predominance, insulin resistance, obesity, hypoglycemia unawareness or insulin sensitivity, eating disorders, and related psychological and social behavior problems often coexist. Investigations of BD should exclude infections, endocrine diseases, and inadequate diabetes education and treatment techniques, as well as noncompliance or manipulation motives. Quantification of autonomic function, gastric emptying, and hormonal counterregulation may be necessary to arrive at a diagnosis.
There are many complexities involved in treating patients with BD and helping them to achieve and maintain normoglycemia. Adopting a team approach involving a broad range of disciplines is essential. Depending on circumstances and available resources, the multidisciplinary team should include the patient, diabetes specialist, primary care physician, nurse, nutritionist, podiatrist, and psychologist/psychiatrist, as well as family and friends. All members of the team should work together to ensure continuity of care. Communication and coordination within the team are also imperative to ensure that all members share and work toward the same treatment targets.
Footnotes
Author Disclosure Statement
No competing financial interests exist.