
Abstract
Diabetes and cardiovascular diseases (CVDs) are increasing in epidemic proportions globally, with the most marked increase in emerging economies. Among emerging economies, China and India have the highest numbers of people with diabetes and CVD. Over the last two decades, 80% of CVD and diabetes mortality occurred in low- and middle-income countries, suggesting that these disorders have become a leading threat to public health in most of the developing countries. The burden of CVD and diabetes in the developing countries affects the productive younger age group, and this has serious economic implications. Diabetes shares many characteristics and risk factors with CVD, and thus the risk for CVD also escalates with the increase in prevalence of diabetes. Both genetic and environmental factors play a major role in causation of diabetes and CVD. However, the major drivers of this dual epidemic are demographic changes with increased life expectancy, lifestyle changes due to rapid urbanization, and industrialization. To reduce the burden of diabetes and CVD in the coming decades, emerging economies need to set national goals for early diagnosis, effective management, and primary prevention of these disorders. In order to curb the epidemic of diabetes and CVD, population-based, multisectoral, multidisciplinary, and culturally relevant approaches including various departments of the government as well as non-governmental agencies are required.
Introduction
Burden of Diabetes in Emerging Economies
Prevalence and projections
It was estimated that in the year 2011, 366 million people worldwide had diabetes, of whom about 80% (291 million) reside in low- and middle-income countries. If these trends continue, by 2030, 552 million people, or one in 10 adults, will have diabetes, of whom 458 million will reside in emerging economies compared with a mere 94 million in developed countries. 4 In countries classified by the World Bank as upper middle-income, lower middle-income, and low-income countries, the prevalence of diabetes in 2011 was 10.1%, 8.6%, and 5.8%, respectively, among individuals in the age group of 20–79 years. 4
Of the top 10 countries listed by International Diabetes Federation in 2011 in terms of the number of individuals with diabetes, eight are classified as developing countries—namely, China, India, the Russian Federation, Brazil, Mexico, Bangladesh, Egypt, and Indonesia (Fig. 1). The highest number of people with diabetes in the world currently is in China (90.0 million in 2011), and these numbers are expected to swell to 129.7 million by 2030, whereas the corresponding figures for India are 61.3 million in 2011, which is expected to increase to 101.2 million by 2030. 4 Although this burden of greater absolute numbers of diabetes may be partially explained by larger population size, the rates at which diabetes is increasing in the developing economies amid rapid epidemiological and nutritional transition are much steeper when compared with in the more developed affluent countries.
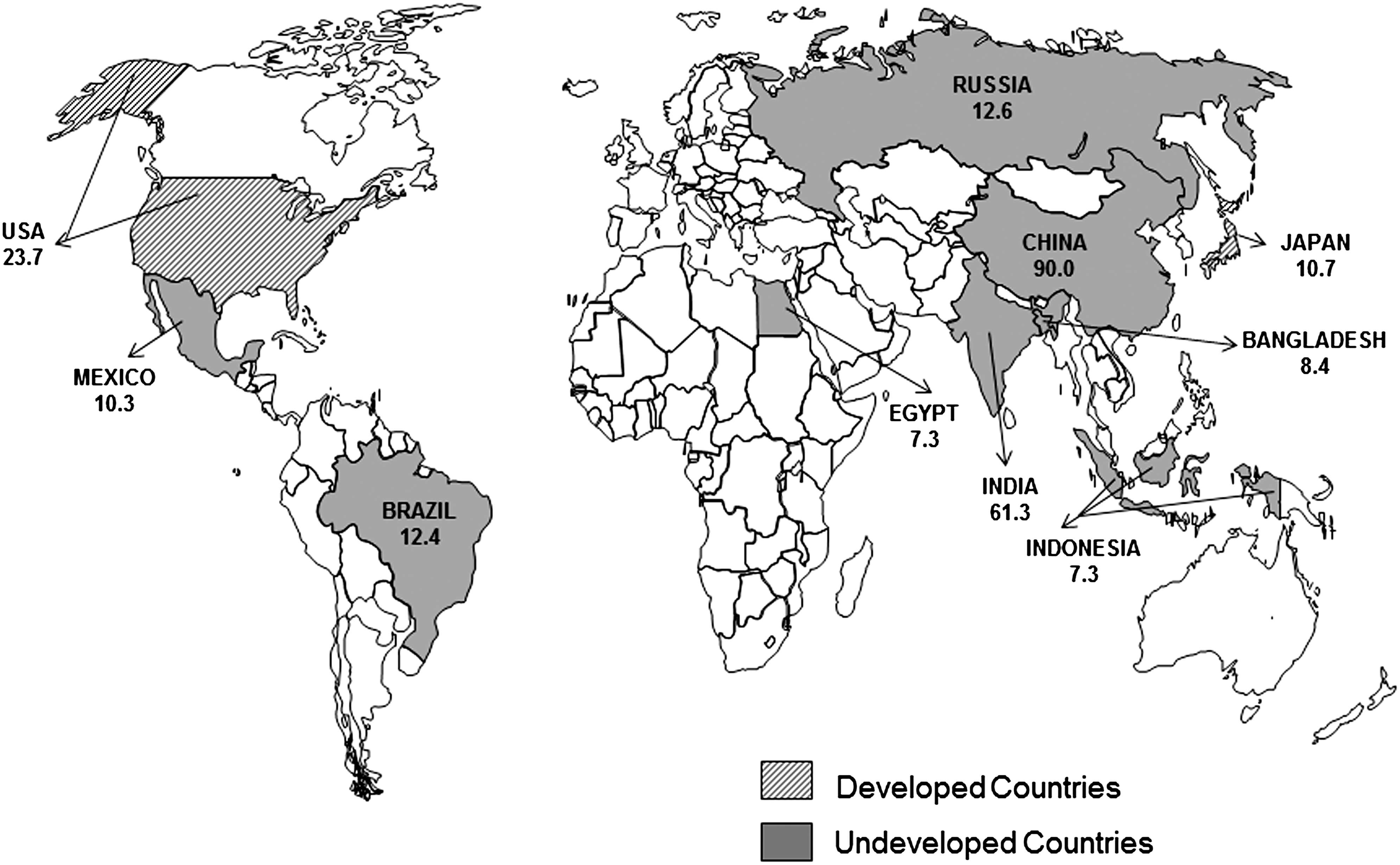
Number of individuals with diabetes (in millions) in the top 10 countries from undeveloped and developed countries in 2011. 4
There are also significant differences between and within developing countries because of the geographical diversity in socioeconomic growth rates, demographic and lifestyle changes, and perhaps differences in genetic susceptibility to diabetes. 5 The prevalence of diabetes in Sub-Saharan Africa ranges from 1% in rural Uganda to 12% in urban Kenya, 6,7 2% in Ethiopia, 8 and 8.1% in urban and 2.3% in rural Bangladesh. 9 In Sri Lanka the prevalence was 10.3%, 10 whereas it was 4.6% in Indonesia, 11 11.6% in Malaysia, 12 and 7.5% in Thailand. 13 In the rural area of the Baluchistan Province of Pakistan there was a twofold increase in the prevalence of diabetes from 7.2% in 2002 to 14.2% in 2009. 14 A recent study from China reported the age-standardized prevalence of diabetes to be 9.7%. 15
In India, the prevalence of diabetes is growing rapidly in both urban and rural areas. 16 The national prevalence of diabetes in India according to the 5th edition of the Diabetes Atlas published by the International Diabetes Federation is estimated at 8.3%, although there are significant differences across geographic areas and socioeconomic classes. 4 The national prevalence of diabetes in India was estimated to be 2.1% from a survey of six cities and adjacent rural areas by the Indian Council of Medical Research (ICMR) in 1972–1975. 17 There have been five other multicenter studies in India. The 2001 National Urban Diabetes Survey showed age-standardized prevalence of 12.1% in India's six largest cities. 18 The Prevalence of Diabetes in India Study, published in 2004, reported urban prevalence of diabetes to be 5.9% and 2.7% in small towns and rural areas, respectively. 19 The World Health Organization (WHO)-ICMR NCD Risk Factor Surveillance Study conducted between 2003 and2005 in urban and rural areas of six different states reported an overall prevalence of self-reported diabetes of 4.5%. 20
Recently the first representative study of four states in the country has been completed. 21,22 This study, called the ICMR-INdia DIABetes (ICMR-INDIAB) study, looked at three states and the Union territory of Chandigarh and reported that the prevalence of diabetes (both known and newly diagnosed) was 10.4% in Tamilnadu, 8.4% in Maharashtra, 5.3% in Jharkhand, and 13.6% in Chandigarh. In Tamilnadu, the prevalence of diabetes in urban areas (13.7%) is almost double the rates found in rural areas (7.8%). In Jharkhand, the prevalence of diabetes in urban areas is fourfold higher than in rural areas (13.5% for urban vs. 3% for rural, P<0.001). In Chandigarh, the prevalence of diabetes in urban is higher than the rates in rural (actually a peri-urban area, as this is a union territory) areas (14.2% for urban vs. 8.3% for rural, P<0.001). Finally, in Maharashtra also, the prevalence of diabetes in urban is higher than the rates in rural areas (10.9% for urban vs. 6.5% rural, P<0.001). The overall number of people with diabetes in India in 2011 based on the ICMR-INDIAB Study was estimated to be 62.4 million, 22 and this was confirmed by the 5th edition of the Diabetes Atlas, which gave a figure of 61.3 million people with diabetes in India in the age group of 20–79 years. 4
Drivers of the diabetes epidemic
The prime drivers of the rapid increase in diabetes (and to a large extent CVD also) are the rapid demographic and epidemiological transitions occurring in developing countries as a consequence of increasing urbanization and industrialization of developing regions. 23 Indeed, diabetes has now reached epidemic proportions, and because of associated factors such as increase in adult population, longevity, behavioral changes, poverty, illiteracy, and lack of access to health care, the social, economic, and human costs of diabetes are likely to be quite formidable in developing countries. This will also result in a parallel growth of diabetes precursors (impaired fasting glucose and impaired glucose tolerance) and the ensuing health consequences. 23,24 In most emerging economies, diabetes exhibits higher prevalence among the higher socioeconomic groups than the lower socioeconomic groups. 25 –28 This pattern is evident in urban Chennai in India, where in the late 1990s, a middle-income group had twice as high a prevalence compared with the lower-income group. 26 Unfortunately, this pattern is now changing, and a more recent report done on the same two residential sites showed a convergence of the prevalence rates of diabetes in the same two residential colonies representing the middle- and lower-income groups. 29
What is more disheartening is the fact that the majority of individuals with diabetes in developing countries are in the productive and economically active population (45–64 years), which is in contrast to developed countries, where the majority of the individuals with diabetes are over 64 years of age. Poorly managed individuals and those who do not have access to proper care are more likely to miss work because of the consequences of the disease, which could adversely affect the productivity and the economy of these countries. Thus it is fair to state that diabetes will be a far bigger health problem in developing, compared with the developed, countries. 30
One of the unfortunate aspects about diabetes is that more than 50% of the people with diabetes are unaware of their disorder. The rate of undiagnosed diabetes is high in most developing countries. In the Screening India's Twin Epidemic (SITE) Study, conducted in 10 Indian states, 7.2% had undiagnosed diabetes. 31 In the ICMR-INDIAB study, conducted in four states of India, the prevalences of undiagnosed diabetes among urban residents of Tamilnadu, Maharashtra, Jharkhand, and Chandigarh were 5.2%, 7.2%, 5.1%, and 7.6% and those among rural residents were 3.8%, 4.9%, 2.3%, and 5.2%, respectively. 22 Undiagnosed diabetes has substantial public health implications as it could lead to higher rates of complications.
Morbidity and mortality due to diabetes
Diabetes exerts a significant burden in developing countries as individuals with diabetes face significant challenges with respect to earlier diagnosis and treatment, which could result in increased morbidity and mortality, decreased life expectancy, and reduced quality of life, as well as individual and national income losses. Although diabetes is often not recorded as a cause of death, diabetes is already the fifth leading cause of mortality globally (4 million deaths annually), outnumbering global deaths from human immunodeficiency virus/AIDS; 80% of this mortality occurs in low- and middle-income countries. 32 Diabetes also leads to other disease conditions and complications, which subsequently become the cause of death. According to the recent Diabetes Atlas, 4 even though the prevalence of diabetes is currently lower in low-income countries compared with high-income countries, the number of deaths due to diabetes in low-income countries (492,000) is nearly as high as in high-income countries (544,000).
Among people with diabetes, the majority of deaths worldwide are due to CVDs and cerebrovascular diseases and end-stage renal diseases. 33 One of the studies conducted in south India, called the Chennai Urban Population Study (CUPS), provided some evidence on the effect of type 2 diabetes on mortality rates in a population. 34 The overall mortality rates were nearly threefold higher in subjects with diabetes compared with individuals without diabetes (18.9 vs. 5.3 per 1,000 person-years). The hazards ratio for all-cause mortality for diabetes was found to be 3.6 compared with subjects without diabetes. The study also showed that the leading cause of mortality in subjects with diabetes was cardiovascular (52.9%) and renal (23.5%) complications. In another study done by Zargar et al. 35 of the 234,776 admissions to their center, 16,690 (7.11%) died, of whom 741 had diabetes mellitus, as recorded in the death certificate. The causes contributing to death were infections (40.9%), chronic renal failure (33.6%), coronary artery disease (16.9%), cerebrovascular disease (13.2%), chronic obstructive pulmonary disease (6.9%), acute renal failure (6.2%), malignancy (4.2%), hypoglycemia (3.5%), and diabetic ketoacidosis (3.4%).
Diabetes increases the risk of both macrovascular diseases (CVDs, which comprise coronary heart disease and cerebrovascular disease or “stroke,” and peripheral vascular disease) and microvascular (retinopathy, nephropathy, and neuropathy) diseases. These complications are associated with considerable morbidity, reduced quality of life, disability, premature mortality, and high economic costs. There are geographic differences in both the magnitude of these problems and their relative contributions to overall morbidity and mortality. In white populations, macrovascular complications such as coronary artery disease and amputations are major causes of disability. In contrast, end-stage renal disease and stroke are prevalent among Chinese and Asian ethnic groups. The increased vulnerability of Pacific Island populations to neuropathy and metabolic problems and of South Asians to coronary artery disease has also been reported. 32 Population-based data on diabetes complications in India, from the Chennai Urban Rural Epidemiology study (CURES) and the CUPS, have reported interesting differences in the patterns of complications seen in Asian Indians. For instance, the prevalences of retinopathy, 36 nephropathy, 37 and peripheral vascular disease appear to be lower, 38 the prevalence of CVD was higher, 39 and that of neuropathy was similar 40 to that reported in the West.
In the least developed countries, diabetic ketoacidosis continues to be the commonest emergency in diabetes, often precipitated by infections, and its contribution to mortality rates ranges from 3.4% in India 34 to 25% in Tanzania and 33% in Kenya. 5 The Diabcare Africa project, which was conducted across six Sub-Saharan African countries, reported that background retinopathy (18%) and cataract (14%) were the most common eye complications and that 48% had neuropathy, although macrovascular disease was rare in that population. 41
Burden of CVD in Emerging Economies
Prevalence and projections
CVD, which is the major contributor to the global burden of disease among the NCDs, encompasses a spectrum of diseases including coronary heart diseases, cerebrovascular disease, rheumatic heart disease, congenital heart disease, and peripheral artery disease. Of the 57 million global deaths in 2008, 36 million (63%) were due to NCDs, of which 17.3 million (48%) were due to CVDs. 42 During the last century, CVD has increased rapidly from a relatively minor disease globally to a leading cause of morbidity and mortality, with more than 80% of all CVD-related mortality now occurring in low- and middle-income countries. 43,44 The Global Burden of Disease Study projects a 55% increase in disability-adjusted life years (DALY) loss attributable to CVD between 1990 and 2020 in developing countries in contrast to the developed nations, which will witness a 14.3% reduction in the proportion of DALY loss attributable to CVD during the same period. 45 Thus, in the next two decades the increasing burden of CVD would be borne mostly by the developing countries.
This can be attributed partly to the exploding population, because of high birth rates. 46 Moreover, CVD occurs at a younger age in emerging economies, which may have personal and macroeconomic implications for the workforce and national productivity. 47 The Global Burden of Disease Study projected that in 2020, 6.4 million deaths would occur due to CVD in the developing countries in the age group of 30–69 years. 45 Furthermore, the leading causes of death in the world in 2030 are predicted to be ischemic heart disease (IHD) and cerebrovascular disease (stroke), both components of CVD. 48
According to recent estimates in India, cases of CVD may increase from about 29 million in 2000 to as many as 64 million in 2015; the number of deaths from CVD accounted for an estimated 2.3 million deaths in 2010 (excluding stroke), and this is projected to increase to 2.9 million in 2015. 49 There are also data to suggest that although the prevalence rates of CVD in rural populations will remain lower than that of urban populations, it will continue to increase, reaching around 13.5% of the population in the age group of 60–69 years by 2015. The prevalence rates of CVD among younger adults (age group of 40 years and above) are also likely to increase, and the prevalence rates among women will keep pace with those of men across all age groups. 49
Drivers of the CVD epidemic
What is driving this increase of the CVD epidemic in the developing countries? CVD is usually associated with one or more risk factors that explain the current burden and the projected increase of CVD, and many of these are in common with diabetes as outlined above. CVDs stem from a combination of modifiable and non-modifiable risk factors. The risk factors for CVD include biological (hypertension, dyslipidemia, and diabetes) and behavioral (diet, physical activity, and tobacco) factors, which are influenced by factors such as globalization, demographic change, sociopolitical determinants, social inequality, education, and cultural norms. 50 Developing societies are faced with a high burden of conventional risk determinants and risk factors, in addition to exposure to potential novel risk factors and perhaps a genetic or programmed fetal vulnerability to CVD in later life. 51 According to Levenson et al., 44 the three factors that have led to increases in risk factors for CVD are (1) the projected 60% increase in population between 1990 and 2020, (2) increasing life expectancy, thanks to improvements in public health and medical care that are reducing rates of communicable disease, malnutrition, and maternal and infant deaths, and (3) economic, social, and cultural changes. A survey conducted in migrant factory workers and their spouses from four cities in India together with their rural-dwelling siblings reported that urban living is associated with an increase in cardiometabolic risks. 52 The findings from this study suggest that body fat increases rapidly when one first moves to an urban environment, whereas other cardiometabolic risk factors evolve gradually. Newly emerging CVD risk factors, such as low birth weight, folate deficiency, and infections, are also more frequent among the poorest segments of the population in low- and middle-income countries. 48
The INTERHEART study conducted in 52 countries demonstrated that over 90% of the population-attributable risk of acute myocardial infarction (AMI) were accounted for by nine modifiable risk factors, which included smoking, diabetes, hypertension, abdominal obesity, the apolipoprotein B/apolipoprotein A1 ratio, psychosocial stress, decreased fruit and vegetable intake, physical inactivity, and alcohol consumption. 53 –56 Although high intakes of fat, salt, and refined sugar have not typically been a concern for developing countries, recent shifts to unhealthy fast-food trends in eating practices globally have resulted from socioeconomic changes that make these problems increasingly relevant for countries in transition. A study from China showed that changing to a “Western diet” was linked to the dramatic increase in the IHD mortality rate. 57 The INTERHEART study reported that an unhealthy dietary intake increases the risk of AMI globally and accounts for approximately 30% of the population-attributable risk. 58 Use of all forms of tobacco is one of the most important causes of AMI globally, especially in men. 59 The INTERHEART study also found that poor education was associated with increased risk for AMI, largely through its association with modifiable risk factors, especially in those countries designated as high income. 60 This study also reported that the least physically active regions were the Middle East, Africa, and China. 56 Figure 2 summarizes the main drivers of diabetes and CVD epidemic in emerging economies.

Drivers of the diabetes and cardiovascular disease (CVD) epidemic in emerging economies.
Morbidity and mortality due to CVD
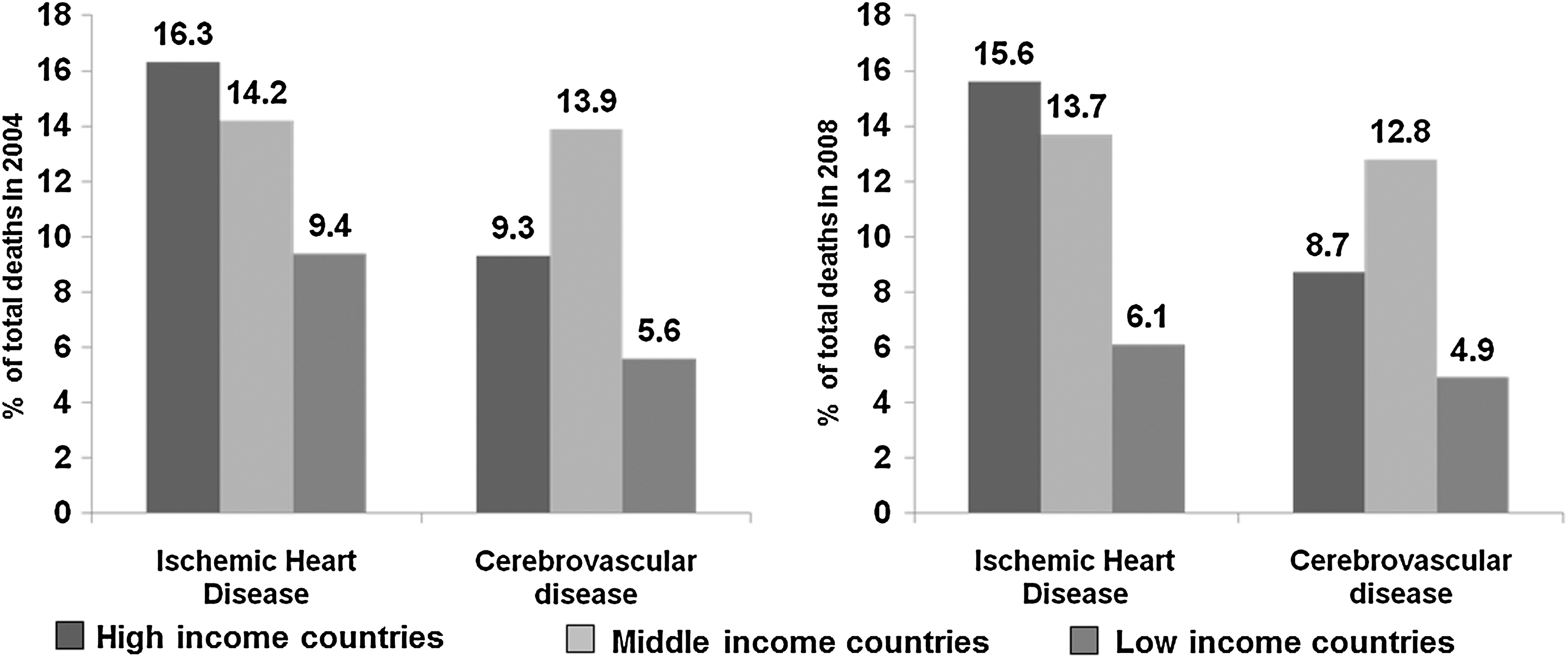
CVDs and their risk factors are major contributors to global morbidity and mortality. 42,61 Figure 3 shows the percentage of deaths due to IHD and cerebrovascular disease by income group in the years 2004 and 2008. 42,43 Heart disease is one of the five leading contributors to years living with disability in elderly people in emerging economies; however, stroke is also reported as a leading cause of disability, second only to dementia. Ten percent of the global disease burden (DALYs) is attributed to CVD. 62 According to the WHO, CVDs are responsible for 151,377 million DALYs, of which 62,587 million are due to coronary heart disease and 46,591 million to cerebrovascular disease. 43,61
In the developing economies, including China, India, other Asian countries, Sub-Saharan Africa, and Latin America and the Caribbean, 23% of deaths were due to CVD (IHD, 9%; stroke, 7.5%; rheumatic heart disease, 0.7%; and other CVDs, 5.7%) in 1990. However, in 2020 this is predicted to increase to 33.8% (IHD, 14.3%; strokes, 10.9%; rheumatic heart disease, 0.8%; and other CVDs, 12.1%). 44
A study conducted in five countries (Brazil, South Africa, Russia [with specific reference to the autonomous republic of Tatarstan], India, and China) emphasizes that much higher proportions of deaths occur in the working age population in Brazil, India, and South Africa in contrast to the United States and Portugal. 47 This study reported that in India, 28% of the deaths occurred among people less than 65 years of age, and that in South Africa, despite the predominance of human immunodeficiency virus/AIDS, the proportion of deaths occurring among people 35–44 old due to chronic disease, mainly CVD, was 12% for men and 17.2% for women. It has also been reported that CVD affects patients in low- and middle-income countries some 10–15 years earlier than in high-income countries, reducing workforce capacity and potential economic growth in these countries. The number of potentially productive years of life lost (PPYLL) due to CVD between 35 and 64 of age was estimated to be 9.2 million (3,572 per 100,000) in India and 6.7 million (1,595 per 100,000) in China in 2000. These estimates are projected to rise to 17.9 million PPYLL in India (3,707 PPYLL per 100,000) and 10.5 million PPYLL in China (1,863 per 100,000), by 2030. 57
The economic burden study carried out by the WHO and World Economic Forum reported that over the period 2011–2025, the cumulative lost output in low- and middle-income countries associated with CVD is projected to be more than US$ 2.52 trillion in upper-middle-income countries and US$ 1.07 trillion in lower-middle-income countries compared with US$ 0.17 trillion in low-income countries. The burden is lowest in the low-income countries, in part because the value of lost earnings in this group is low and in part because the total population of these countries is much smaller than that of the middle-income countries (which include China and India). 63
Health care for diabetes and CVD
In countries where access to health care is not limited and people often need to pay for their own health care, it is the economically backward people on whom diabetes and CVD have the greatest social and economic impact. Currently, public health services in emerging economies are overstretched by increasing demands to manage chronic disease, including diabetes and CVDs. Hospitals consume enormous amounts of resources, and health ministries may spend more than half their budgets on treatment services that depend on hospitals. As a result, a large proportion of people with high cardiovascular risk remain undiagnosed, and even those diagnosed have insufficient access to treatment at the primary healthcare level. 61 Despite the substantial burden of chronic diseases, data from the World Health Survey conducted in India show that a large proportion of the population (52.7%) receives no treatment for diabetes. 64
The economic consequences of diabetes and CVD to the individual and society are multifold. Direct costs to people with diabetes and CVD and to their families and to the healthcare sector include consultation, investigation, medication, management, hospitalization, treating complications, and transportation and time utilized for care in case of non-medical expenses. Indirect costs to society and government, which are related to productivity costs, include work days lost, low productivity, disability payment, social security, and depression.
An individual with diabetes spends around twice as much on medical care compared with his or her contemporary without diabetes. In India, nationally representative sample surveys estimate that the total direct cost for diabetes treatment is INR 7,158 per person per year, much of which is paid for by the patient out of pocket; indirect costs are a further INR 12,756 per person per year ($1 USD=50 INR approximately). 65
For the developing world, a U.S. Institute of Medicine report on the macroeconomic impacts of CVD and chronic diseases in several countries suggests that the economic impact of CVD and related chronic diseases is huge. Estimates ranged from an annual US$ 3 billion for direct medical costs of obesity-related diabetes, coronary heart disease, hypertension, and stroke in China to US$ 72 billion for treatment of and productivity losses due to five chronic conditions in Brazil. 66 In India, a World Bank study showed that 25% of families with a member with CVD experience catastrophic expenditure, and 10% are driven into poverty. 67 Catastrophic health spending was present in 50% of respondents in China, India, and Tanzania. Distress financing and lost income were more common in low-income respondents. 68 Huffman et al. 68 concluded that individuals in Argentina, China, India, and Tanzania bear significant financial burdens following CVD hospitalization, with substantial variation across and within countries.
Summary
The burden of type 2 diabetes and CVD in emerging economies is summarized in Table 1. Ongoing challenges for healthcare delivery in many developing regions are the lack of resources, the low priority of NCD in systems geared toward acute care and infectious diseases, and the lack of an integrated infrastructure involving communities, health services, local, and regional institutions. 69 Thus prevention of diabetes and CVD should mainly be addressed first through primary prevention by creating awareness and an enabling environment for adoption of healthy living habits by the community, early detection of persons with risk factors, and cost-effective interventions for reducing risk and cost-effective secondary prevention measures to prevent complications. Second, prevention should be at the societal and policy levels to address the social determinants of health (e.g. altering the tobacco, food, and activity environment and policy-level measures by means of legislation and regulatory approaches on the agriculture and food industry, tobacco use, or physical activity). In addition, development of comprehensive and integrated health systems that are based on primary healthcare needs is of great importance. Thus if the epidemic of NDCs is to be curbed in emerging economies, it requires a multisectoral approach including several departments of the government, encompassing health, agriculture, urban planning, transportation, finance, broadcasting, and education, in addition to the food and pharmaceutical industry and non-governmental agencies and civil society to reduce the burden due to diabetes and CVD in emerging economies. The time to act is NOW!
CVD, cardiovascular disease.
Footnotes
Acknowledgments
Dorairaj Prabhakaran is supported by research grants from the National Heart Lung and Blood Institute, United States of America (HHSN286200900026C) and National Institute of Child Health and Disease (NICHD), United States of America (1D43HD065249).
Author Disclosure Statement
No competing financial interests exist.