
Abstract
Background:
The aim of this report was to develop a dissolving microneedle (DM) application system, where 225–300 insulin-loaded DMs were formed on a chip. After the heat-sealed sheet is removed, the system covered with the press-through package layer is put on the skin. By pressing with the hand, insulin DMs were inserted into the skin.
Materials and Methods:
Factors affecting the penetration depth of DM were studied using applicator in vitro and in vivo experiments. The penetration depth was determined for rat and human skin. Two-layered DM array chips were prepared to obtain complete absorption of insulin and administered to the rat abdominal skin. Plasma glucose levels were measured for 6 h. By comparing the hypoglycemic effect with that obtained after subcutaneous injection, relative pharmacological availability (RPA) was determined.
Results:
The penetration depth increased from 21±3 μm to 63±2 μm in proportion to application speed to isolated rat skin, at 0.8–2.2 m/s. Human skin showed similar results in the penetration depth. The in vivo penetration depth was dependent on the force (0.5–2.5 N) and duration (1–10 min), as the secondary application force. The penetration depth was 211±3 μm with a duration of 3 min in the in vivo rat experiment. DM array chips having an insulin-loaded space of 181.2±4.2 and 209±3.9 μm were evaluated in the rat. RPA values of insulin from DMs were 98.1±0.8% and 98.1±3.1%, respectively.
Conclusions:
These results suggest the usefulness of the two-layered DM application system for the transdermal delivery of insulin.
Introduction
The skin comprises three layers: the stratum corneum, which has a strong primary barrier function and is 10–15 μm thick; the viable epidermis, as the secondary barrier, 100–150 μm thick with no blood vessels that contains living cells; and the dermis, for the third barrier. Regarding skin vaccine delivery systems, antigen-presenting cells, 16 which populate the skin, Langerhans cells, and dermal dendritic cells, are highly distributed in the epidermis and dermis. 17,18 Vaccine antigen is designed to formulate at the distal and the second portion of the DMs. In the case of drugs for which action is dependent on systemic exposure such as insulin, 19 erythropoietin, 20 desmopressin, 21 and leuprolide acetate, 22 drugs were formulated at the acral portion of microneedles. The DMs were inserted into the region of the epidermis and/or epidermal/dermal junctions with fingers. After the microneedle array chip was administered to the skin, the base polymer dissolved immediately, and the formulated drug was released within 5 min. A two-layered DM array chip with insulin showed relative pharmacological availability (RPA) of 33.2–35.2% in rats. 19 To obtain complete absorption of insulin from the DMs, the acral portion must be inserted completely into the skin.
In this study, the factors that affect the penetration depth of the DMs were studied by using a DM applicator to control the collision speed of DMs to the skin. Based on the results obtained, DM array chips of which the insulin-loaded acral portion was designed to be inserted completely into the skin tissue were prepared, and the RPA of insulin was studied in rats.
Materials and Methods
Materials
Insulin sodium salt was prepared in our laboratory using bovine pancreas insulin (28 IU/mg) (Sigma-Aldrich Corp., St. Louis, MO). A Glucose CII-Test kit, cellulose acetate, and sodium chondroitin sulfate were obtained from Wako Pure Chemical Industries Ltd. (Osaka, Japan). Evans blue was obtained from Nacalai Tesque Inc. (Kyoto, Japan). Hydroxypropyl cellulose was obtained from Nippon Soda Co., Ltd. (Tokyo, Japan). Male Wistar–Hannover rats used in the study were given a standard solid-meal commercial food obtained from Japan SLC Inc. (Hamamatsu, Japan). All other materials were of reagent grade.
Preparation of insulin-loaded DM array chips and insulin solution
To 10.0 mg of sodium insulin and 0.5 mg of Evans blue, 100 μL of 0.1 M phosphate-buffered saline (pH 7.4) was dissolved. By adding 40 mg of sodium chondroitin sulfate to this solution, chondroitin glue containing insulin and Evans blue were obtained. After the drug glue was degassed under reduced pressure, it was dispensed into a mold containing 225, 248, or 300 inverted cone-shaped wells with area of 1.0 cm2. Each well was 500 μm deep and 300 μm in diameter at its top. The mold was covered with a 300-g steel plate, and the drug glue was filled into the wells. After the plate was removed, glue consisting of 15 mg of chondroitin sulfate and 25 mL of distilled water was painted over the mold and dried under the pressure of a stainless steel plate for 3 h. The plate was removed, and DMs were obtained by detaching them with a chip that was made of a mixture of cellulose acetate and hydroxypropyl cellulose (10:1 vol/vol) by means of a tabletting machine (model Handtab-100; Ichihashi Seiki, Kyoto). The size of chip was 2.0 mm wide and 17 mm in diameter. An insulin-loaded DM array chip with Evans blue was observed using a digital videomicroscope (model VH-5500; Keyence Co. Ltd., Osaka) under normal light.
Insulin content in the DM array chip
Insulin was extracted from a chip having DMs with 5.0 mL of phosphate buffer (pH 7.4) for 10 min. The extract was obtained after centrifugation at 43,012 g for 5 min at 8°C (Kubota 3700 centrifuge; Kubota Co., Tokyo). Insulin was determined by the high-performance liquid chromatography method as described in our previous report. 23
In vitro and in vivo penetration depth measurement of DMs into rat and human skin
Male Wistar–Hannover rats (weighing 328±23 g) were anesthetized with sodium pentobarbital (50 mg/kg). Hair on the abdominal region was removed with a shaver (model ES7111; Panasonic Inc., Osaka). Dermatomed human skin was kindly provided by a nonprofit organization: Human & Animal Bridging Research Organization (Tokyo). It was used after defrosting at 32°C and 95% humidity in an incubator (Tokyo Rikakikai Co. Ltd., Tokyo) for 30 min. The DM array chip was attached to the applicator (Fig. 1), which was prepared from a disposable syringe (model ss-10ESz syringe; Terumo Corp., Tokyo). The speed of the inner cylinder was measured using a high-speed camera (model EX-FH100; Casio, Tokyo), and the collision pressure was measured using a digital force gauge (model FGN-2; Nidec-Shimpo Corp., Kyoto). The penetration depth of microneedles was measured by subtracting the length before and after application to the skin using a 10× objective videomicroscope (model VH-5500; Keyence Co.). To another group of rats, a DM array chip was administered to their hair-removed abdominal skin by an applicator with the animals under anesthesia. The in vivo penetration depth was also measured by the above method.
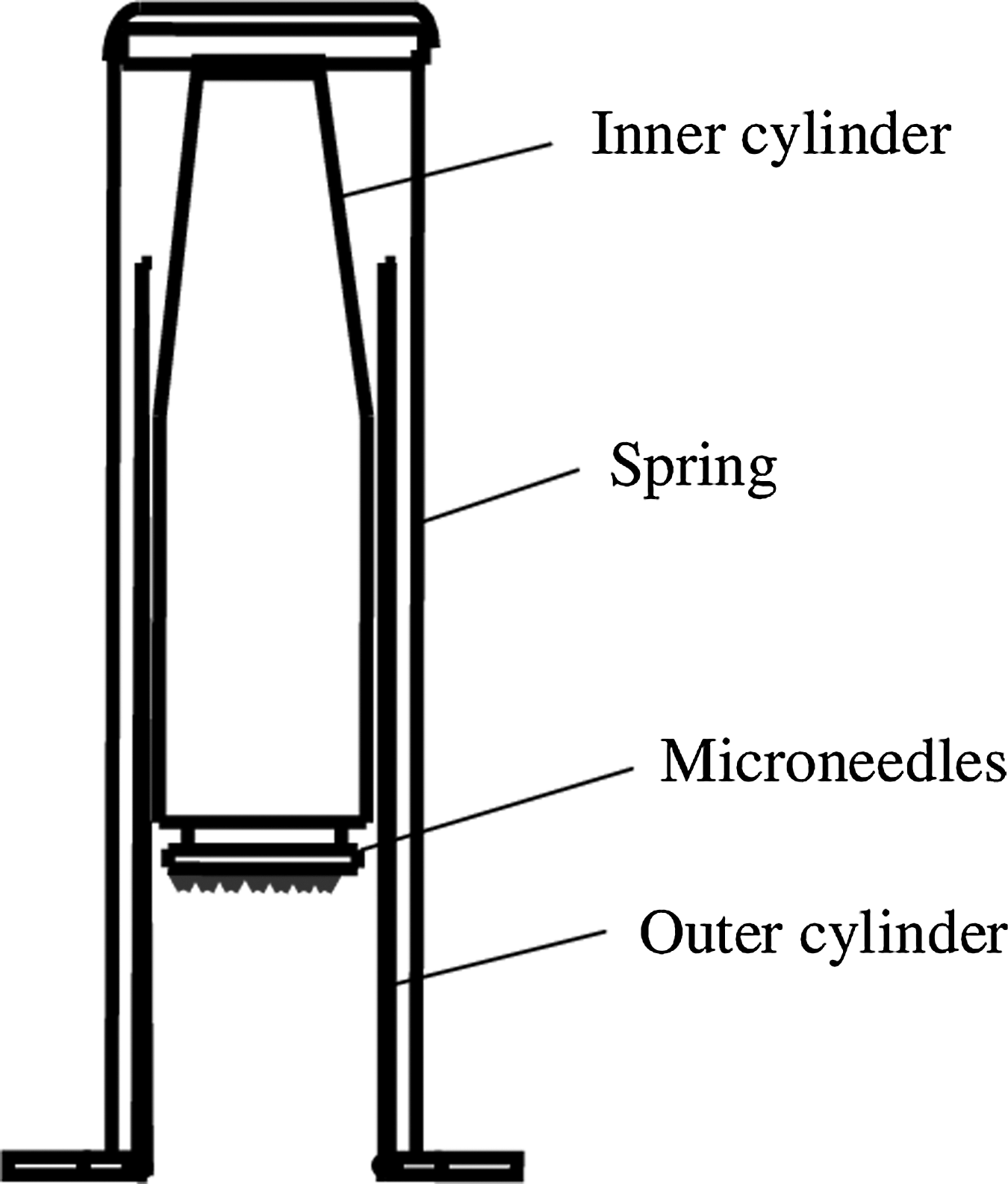
Dissolving microneedles applicator used for the administration of the dissolving microneedles array chip to the skin.
Pharmacodynamic study in rats
Male Wistar–Hannover rats (weighing 331±18 g) were anesthetized with sodium pentobarbital (50 mg/kg). One group consisted of three or four rats. At 5 min before drug administration, 0.25 mL of blank blood samples was obtained. Hair on the abdominal region was removed. The DMs were administered to the skin using the applicator and were pressed for 3 min. At 0.5, 1, 1.5, 2, 2.5, 3, 4, 5, and 6 h after administration, 0.25-mL blood samples were collected from the left jugular vein. For the subcutaneous injection experiment, an insulin solution (14.0 IU/mL) was injected into rats (1.0 IU per rat). By centrifugation at 43,012 g for 10 min at 4°C in the Kubota model 1700 centrifuge, 100-μL plasma samples were obtained and stored at −80°C until analysis. All animal protocols were approved by the institutional animal care and use committee. All experiments were conducted in accordance with the Guidelines for Animal Experimentation of Kyoto Pharmaceutical University.
Plasma glucose assay
The plasma glucose concentration was determined using a Glucose CII-Test kit. Hypoglycemic effect was expressed as a percentage of the predose level. The cumulative percentage change in the plasma glucose level was calculated by summing the areas above the plasma glucose levels in the percentage change versus time curves (AAC) for 0–6 h using the trapezoidal method.
Pharmacodynamic analysis
The RPA of insulin from DMs was calculated as follows:
where AACper and AACsc, respectively, signify AAC values after percutaneous and subcutaneous administrations of, respectively, Doseper and Dosesc. The time at which plasma glucose level showed the minimum concentration was determined.
Statistics
All data are expressed as mean±SE values. Statistically significant differences were assumed to be significant when P<0.05 (by Student's unpaired t test).
Results
Penetration depth and diffusion kinetics of DMs in the skin
An applicator was prepared by modifying the conventional disposable syringe as shown in Figure 1, where a Terumo 20-mL syringe was used. Before the experiment using skin samples, the relation between the application speed and collision force of the applicator was studied, and a good linear relation was obtained. Chips having 225 DMs were loaded on the top of the piston of the applicator, and the effect of the application speed on the penetration depth into the skin tissue was studied using both rat and human isolated skin samples. As seen in Figure 2A, the penetration depth of DMs into the skin tissue increased from 21±3 (mean±SE) μm to 63±2 μm according to the application speed of 0.8–2.2 m/s. At the application speed of 4.2 m/s, the penetration depth was 72±3 μm. The same results were obtained with the isolated human skin samples, and no significant difference was found in the penetration depth of DMs into the skin between rats and humans. As the application speed in the in vivo rat experiment increased from 0.8 m/s to 2.2 m/s, the penetration depth of DMs increased from 23±3 to 57±5 μm in proportion to the application speed as shown in Figure 2B. Therefore, no significant difference was found between in vitro and in vivo experiments in the penetration depth of DMs into rat skin. Figure 3 shows the effect of the number of DMs, from 225 to 300, in the array chip on the penetration depth into rat and human skin in the in vitro experiment. To evaluate whether the penetration depth increased along with the time during the secondary application force, 0.5–2.5 N, 225 DMs were administered to isolated rat skin and human skin at the application speed of 2.0 m/s. Figure 4A shows the penetration depth was increased to 125±5, 138±4, 180±8, and 195±10 μm depending on the interval of the secondary force duration of 2, 3, 5, and 10 min. The maximum penetration depth was 250±7 μm at 2.5 N for 10 min. Figure 5 shows images of rat and human skin before and after application of array chip having 225 DMs, of which the acral portion contained insulin and Evans blue under the secondary force of 2.5 N for 3 min. At 10 min, blue spots attributable to the insertion of DMs were diffused into the skin and did not disappear at 2 h.
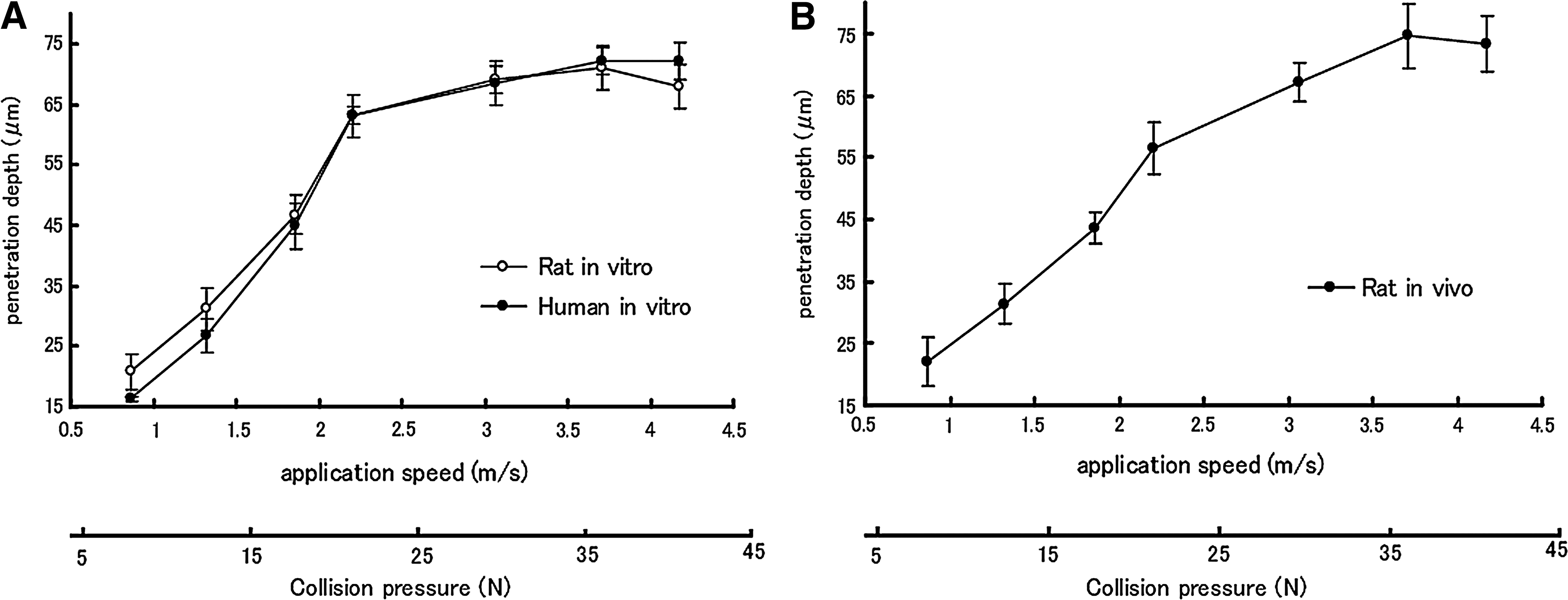
Effect of application speed of a 225 dissolved microneedles array chip on the penetration depth into
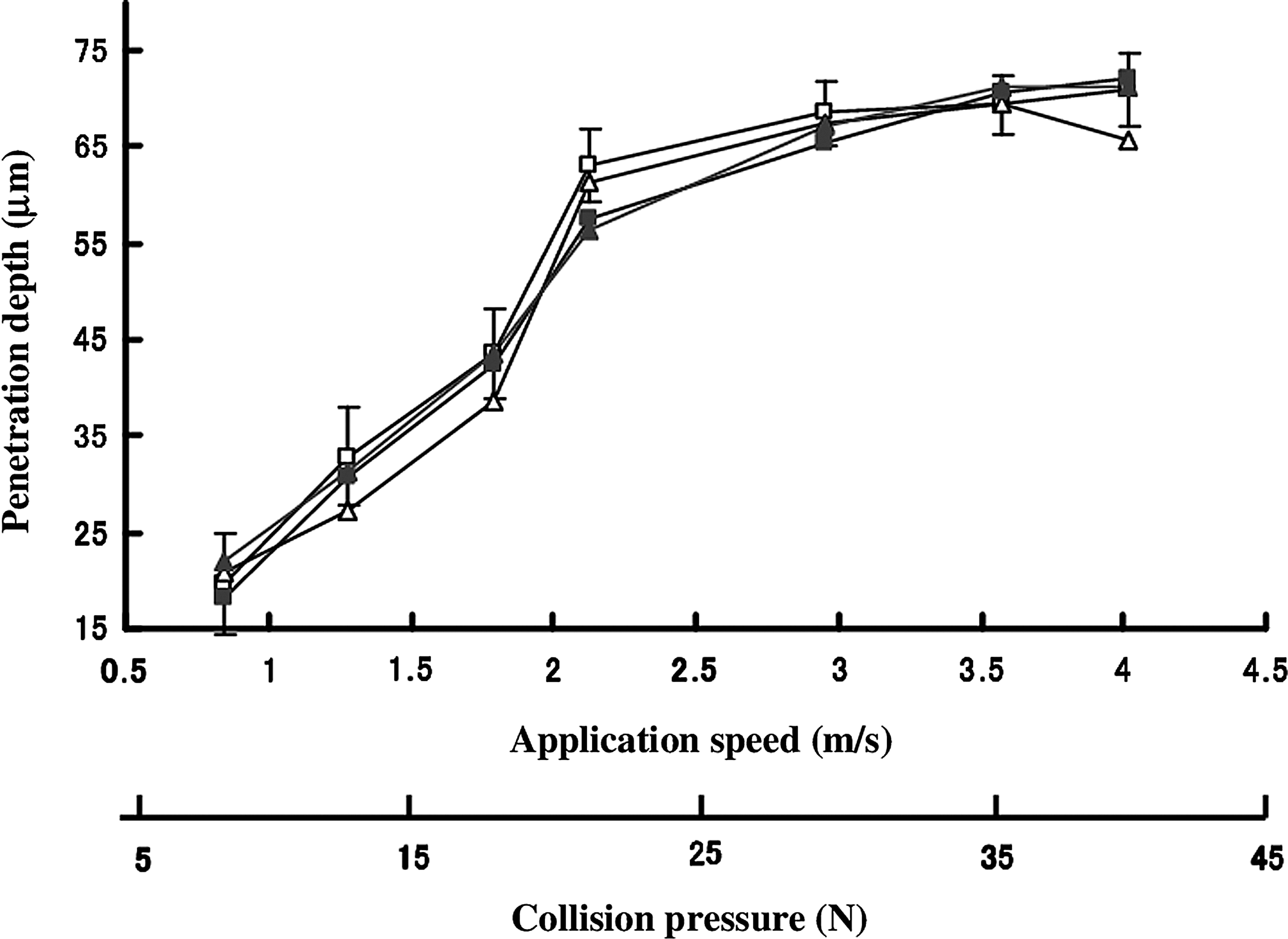
Effect of number of dissolving microneedles on the penetration depth of dissolving microneedles into isolated rat and human skin: 248 dissolving microneedles, rat skin (□); 300 dissolving microneedles, rat skin (Δ); 248 dissolving microneedles, human skin (■); and 300 dissolving microneedles, human skin (▲). Data are mean±SE values (n=3–5).
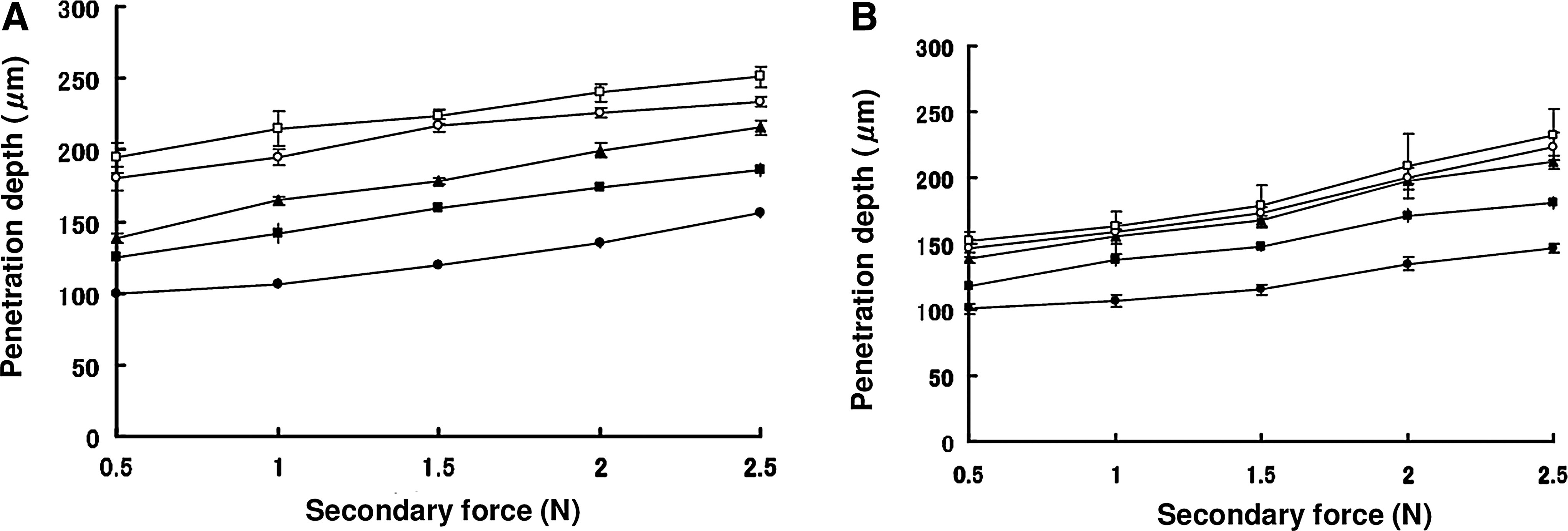
Effect of secondary application force and duration on the penetration depth of dissolving microneedles into
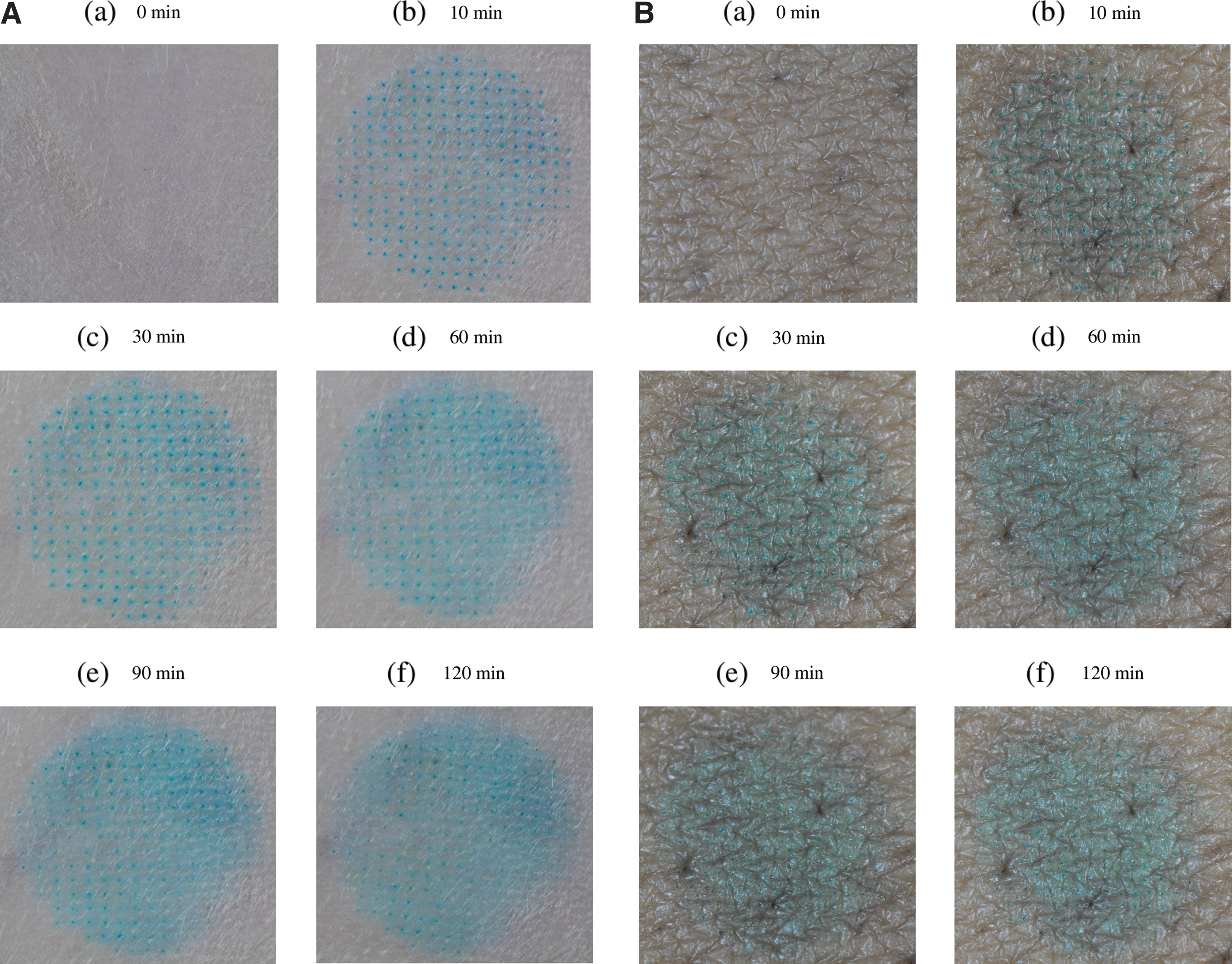
Images of the isolated
On the other hand, in the in vivo condition, the effect of the penetration depth increased along with the time during which the secondary application force was studied. Figure 4B shows that as the secondary application force increases from 0.5 N to 2.5 N, the penetration depth of the DMs increased. When the duration of the secondary application force, 2.5 N, was increased to 5 and 10 min, the penetration depth was not further increased. Therefore, we may state that the duration of 3 min for the secondary force was practically enough. Figure 6 shows the diffusion kinetics of Evans blue in the in vivo rat experiment. Blue spots lost their color as the time passed. This suggested that both Evans blue and insulin were cleared gradually from skin tissue into the systemic circulation.
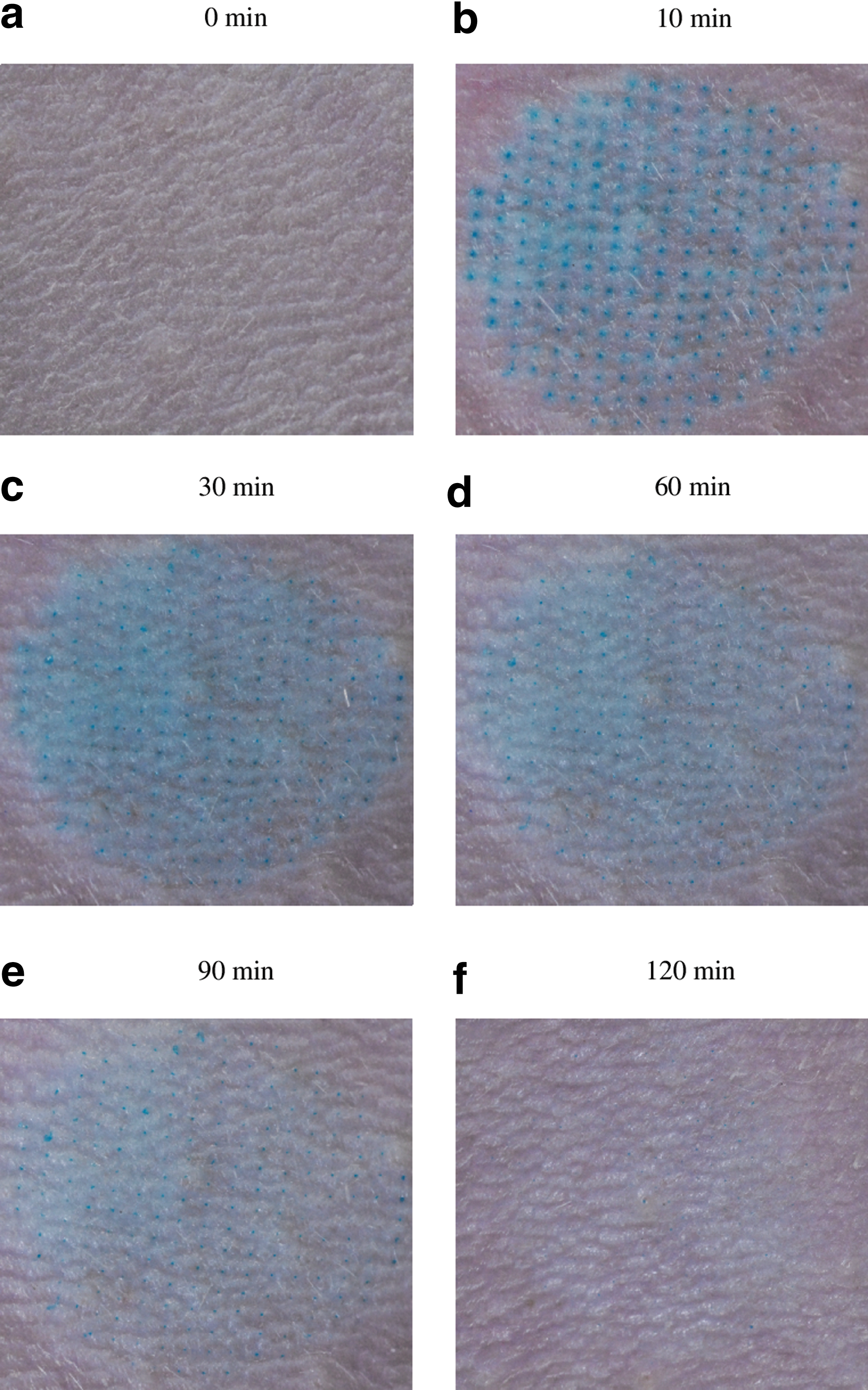
Images of rat skin
Evaluation of DM array chips having high absorption efficiency of insulin
Based on the results of the penetration depth of DMs, two-layered DM array chips of two kinds, termed DM-180 and DM-210, having lengths of the insulin-loaded space at the acral portion were prepared. The physicochemical properties of the prepared two-layered DM array chips are shown in Table 1. The insulin contents were 1.58±0.03 and 1.72±0.13 IU. The insulin-loaded two-layered DM array chips were administered with an applicator to rat skin with an application speed of 2.2 m/s and a secondary force of 2.5 N for 3 min. Figure 7 shows the time course of the hypoglycemic effect of insulin after administration to rats. The plasma glucose concentrations reached to the minimum level at 2 h and returned to normal levels at 5 h. As a reference, insulin solution was injected subcutaneously to the other group of rats at 1.0 IU per rat. By comparing the AACs obtained from the percutaneous administration, the RPA was calculated (Table 2T2). The RPAs of insulin from DM were 98.1±0.8% and 98.1±3.1%, respectively. Figure 8 shows photographs of DM array chip before and after administration to the rat skin. The insulin-loaded space disappeared completely after administration.
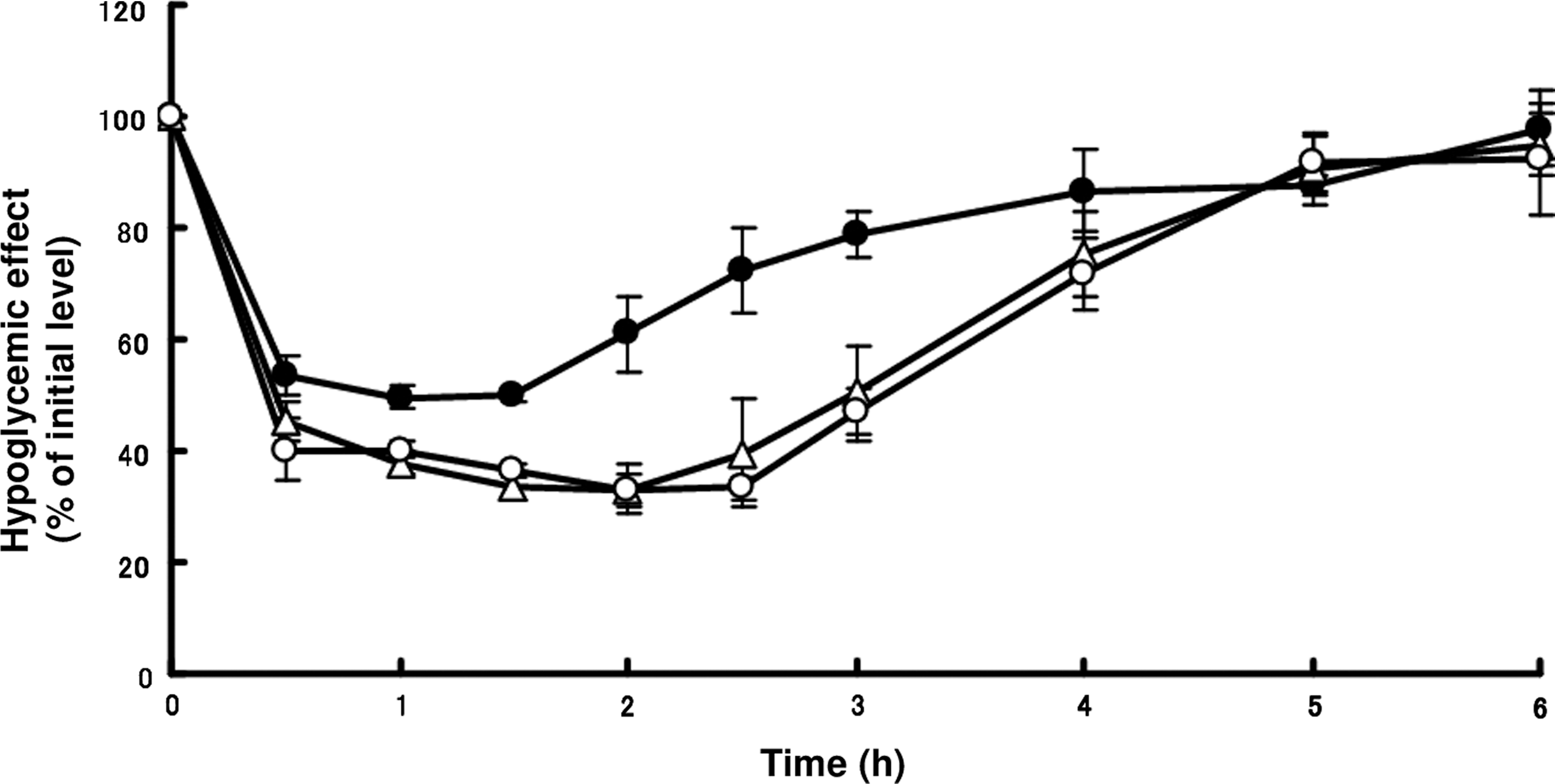
Hypoglycemic effect–time curves after percutaneous administration of insulin-loaded chips having 225 dissolving microneedles with an insulin-loading space of 180 μm and 210 μm in length (1.58±0.03 IU [◯] and 1.72±0.13 IU [▵], respectively, per rat) and subcutaneous injection of insulin solution (1.0 IU per rat) (●) to rats. Data are mean±SE values (n=4).
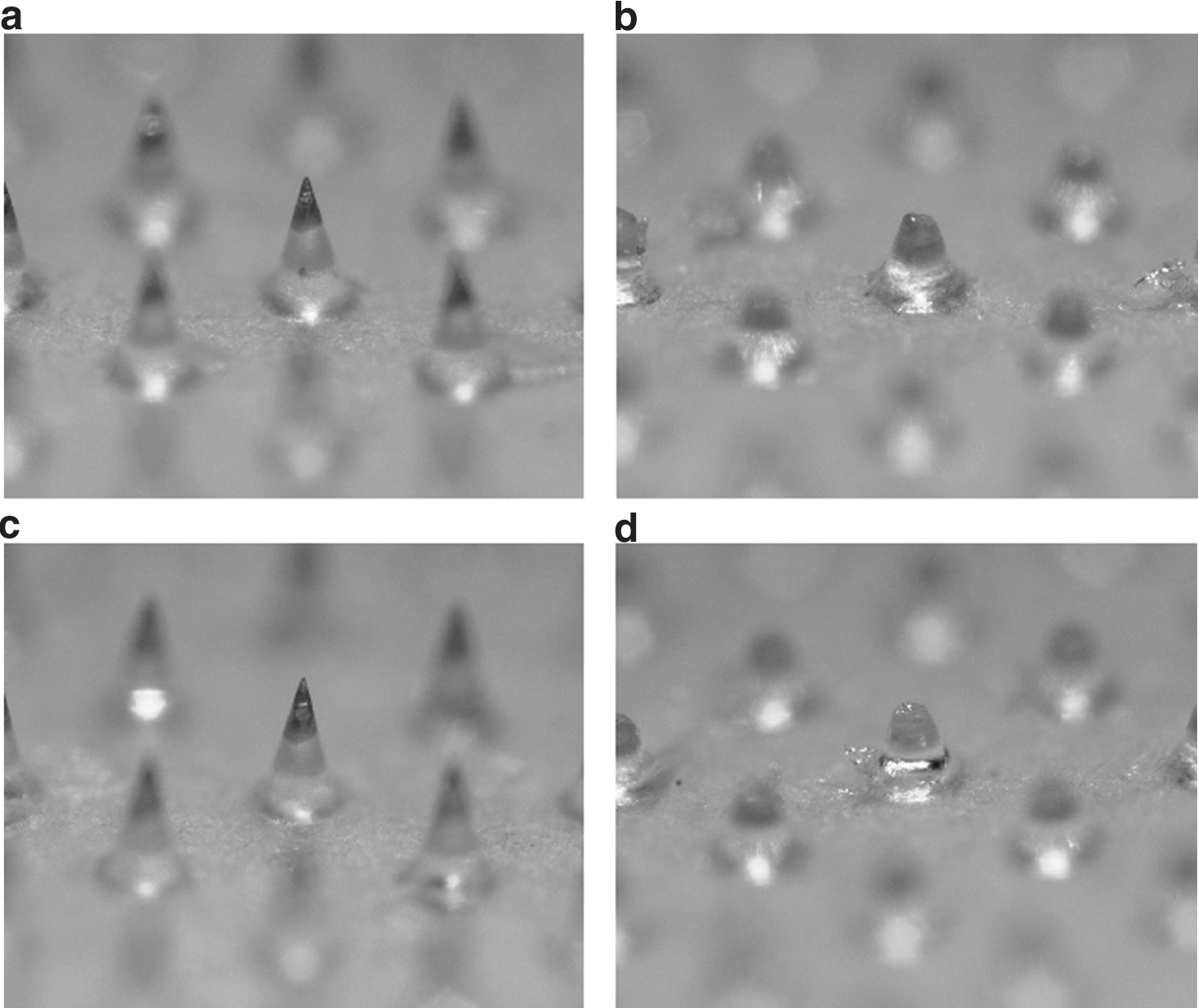
Microscopic photographs of two dissolving microneedles array chips having insulin-loading space lengths of 180 and 210 μm:
Data are mean±SE values (n=4–5).
DM-180 has a loading space length of 180 μm; DM-210 has a loading space length of 210 μm.
DM-180 has a loading space length of 180 μm; DM-210 has a loading space length of 210 μm.
AAC, area above the plasma glucose level versus time curve; C min, minimum concentration of plasma glucose; RPA, relative pharmacological availability; T min, time when the plasma glucose concentration reaches its minimum.
Discussion
Microneedles are applicable to local therapy and systemic drug therapy. In the case of insulin-loaded DMs, the bioavailability of the formulated insulin is an important factor. Our previous studies showed the effect of molecular weight on the extent of bioavailability of fluorescein isothiocyanate–dextrans having molecular sizes of 10–70 kDa; the extent of bioavailability was dependent on molecular size. 24,25 When the molecular size of fluorescein isothiocyanate–dextran became higher than 40 kDa, the extent of bioavailability became lower than 50% because of the limited permeability through the microcapillary wall in the skin. As the molecular size of insulin is 6 kDa, the permeability through the microcapillary wall in the skin tissue is not the rate-limiting step for the systemic circulation. In our other previous study on the percutaneous delivery of insulin, the length of the insulin-loaded space was 300 μm. 19
This report describes the first study of the penetration depth of insulin DMs in the skin. The application speed showed no difference on the penetration depth of DMs between rat and human skin in the in vitro experiment because this was not living tissue. Therefore, the penetration depth increased along with the time during which the secondary application force increased. Some scientists introduced optical coherence tomography to estimate the penetration depth of DMs into the skin. 26,27 Donnelly et al. 26 reported that the penetration depth increased as the application force increased. However, by using hair-removed rat abdominal skin, the penetration depth increasing with the application force was detected as saturation in our in vivo penetration experiment. This evaluation method is thought to supply more detailed information. In the pharmacodynamic studies, almost 100% RPA against subcutaneous injection of the insulin solution was obtained after administration of different-length DMs of 180 or 210 μm at 3 min of secondary application force in rat experiments. Moreover, no bleeding after percutaneous administration suggested that DMs could not reach to the dermis. Therefore, this device is expected to be a nonpainful preparation.
A morphological experiment was also performed, yielding results suggesting that there was neither damage nor irritation on the skin after administration of the DMs (Figs. 5 and 6). Chondroitin sulfate used as a water-soluble thread-forming polymer is a peptidoglycan that exists in biological tissues. 28 –30 Therefore, no safety problem exists when it is used for DM array chips.
Insulin is a representative peptide/protein drug that is very useful for therapy of diabetes patients. However, delivery systems must be developed for more comfortable clinical use. The usefulness of the applicator used here has been confirmed. To provide DMs as a pharmaceutical preparation, the DM array chip must be packaged under sealed conditions. The prototype of the insulin application system with DMs was prepared as shown in Figure 9. After the aluminum-sealed film is first removed, the system is put on the skin. Thereafter, the patient pushes the top of the press-through package and keeps it on for 3 min before removing the whole system. Thus, the system is easy to use for elderly patients and children.

Press-through package (PTP) insulin dissolving microneedles (DM) array chip. Color images available online at
The proposed transdermal insulin application system with DMs presents a superior solution to several clinical problems because the percutaneous administration of insulin has the following advantages: (1) no degradation by hydrolytic enzymes in the gastrointestinal tract, (2) no pain compared with injection, and (3) better convenience of administration. Therefore, DMs are a safe and useful TDDS for insulin, compared with numerous TDDSs such as chemical enhancers, electric fields, ultrasound, and thermal methods. 31 –34 Our findings support the development of percutaneous insulin therapy.
Conclusions
The penetration depth of DMs was studied using an applicator, revealing two important factors: the application speed and force and the duration of the secondary application force. The penetration depth was dependent on both the secondary application force, 0.5–2.5 N, and its duration, 1–10 min. Linearity was obtained between the penetration depth and a duration of 1–3 min. When the secondary application force of 2.5 N was applied to the chip for 3 min, the penetration depth was 211±3 μm. After DMs having the length of insulin-loading space of 181±4 μm and 210±4 μm were administered to rat skin, RPAs of insulin were 98.1±0.8% and 98.1±3.1%, respectively. Those results suggest the usefulness of a two-layered DMs application system for transdermal delivery of insulin.
Footnotes
Acknowledgments
We appreciate the kindness shown by the Human & Animal Bridging Research Organization, Tokyo, Japan, in providing us human skin preparations. This study was supported by a strategic fund of the Ministry of Education, Culture, Sports, Science and Technology during 2008–2013 for establishing research foundations at private universities in Japan.
Author Disclosure Statement
No competing financial interests exist.