
Abstract
Background:
Insulin adsorbs to plastic tubing, which decreases the concentration of an insulin solution delivered from an intravenous infusion set. Dwelling insulin within tubing before starting the infusion decreases adsorption but delays treatment initiation and wastes time in infusion preparation. The lack of data on dwell time effects results in wide variability in practice. We aim to determine the effect of dwell time on insulin concentration from intravenous infusion tubing.
Materials and Methods:
In this in vitro study, we used insulin solutions with concentrations of 0.1 unit/mL, 1 unit/mL, and 10 units/mL. Each solution dwelled in intravenous infusion sets for 0, 15, 30, or 60 min. After the dwell, we measured insulin concentrations from the solution bags and tubing. We repeated each insulin concentration–dwell time combination five times. Comparisons were performed using analyses of variance.
Results:
For each of the three insulin concentrations, the mean insulin concentrations from the tubing were not significantly different between dwell times. Duration of dwell time did not affect insulin adsorption in polypropylene intravenous infusion sets.
Conclusions:
We recommend that following a 20-mL flush, insulin infusions can be started without any dwell time. Removal of dwell times may improve clinical practice by minimizing preparation time and will allow faster initiation of insulin infusion therapy.
Background
This study aims to determine the minimum dwell time needed to minimize insulin adsorption losses within intravenous tubing. We hypothesize that adsorption losses will decrease with increased dwell time.
Materials and Methods
We performed an in vitro study simulating continuous insulin infusions. We selected three insulin concentrations to test—0.1 unit/mL, 1 unit/mL, and 10 units/mL—covering the most commonly used insulin concentrations in clinical practice (authors' unpublished data). Registered pharmacists prepared the different solutions by injecting Novolin® R U-100 regular human insulin (Novo Nordisk Pharmaceuticals, Princeton, NJ) into 250-mL polyvinyl chloride bags of 0.9% NaCl.
Separate 100-inch latex-free polypropylene intravenous infusion sets (Lifeshield primary intravenous set with backcheck valve and two clave ports; Hospira, Lake Forest, IL) were attached to the solution bags. Polypropylene is the standard plastic tubing used at our institution for continuous intravenous insulin infusions. The infusion sets were then primed with the insulin solution so that all air bubbles were eliminated within the tubing. Each insulin concentration dwelled within the intravenous infusion sets for 0 min, 15 min, 30 min, or 60 min. After the allotted dwell time, 20 mL of effluent was removed from the infusion set while the tubing was still connected to the solution bag, 14 completely flushing the tubing. After removing the effluent, we collected 1-mL samples from the end of the tubing directly into 12-×75-mm borosilicate glass vials (Fisher disposable culture tubes; Fisher Scientific, Hampton, NH) for analysis. Samples were also collected simultaneously from the insulin solution bags using a 1-mL syringe (BD, Franklin Lakes, NJ) attached to an 18-gauge blunt fill needle (BD) for comparison. We repeated the experiment five times for each insulin concentration–dwell time combination using separate intravenous infusion tubing for each trial.
Certified laboratory technicians from the Core Laboratories at Yale University immediately diluted each sample with a proprietary assay buffer (Millipore, Billerica, MA). The following dilutions were performed: 1:1,000 for insulin at 0.1 unit/mL, 1:10,000 for insulin at 1 unit/mL, and 1:100,000 for insulin at 10 units/mL. Insulin concentrations were measured using a double antibody radioimmunoassay insulin kit (Millipore).
Statistical analysis
Insulin concentration was measured from the tubing and solution bag for each concentration–dwell time combination. Data were presented as mean±SD values of the insulin concentration. Tubing insulin concentration was also normalized to solution bag insulin concentration by expressing the tubing concentration as a percentage of solution bag concentration. Normalized data were presented as mean±SD values of the percentage.
For each insulin concentration, the mean insulin measurements were compared within sampling sites (i.e., bag vs. tubing) and between dwell times using two-way analysis of variance with repeated measures. Mean percentage of solution bag concentration was compared across dwell times using one-way analysis of variance. A value of P<0.05 was considered statistically significant. Statistical tests were performed using SPSS version 19.0 for Windows (SPSS, Inc., Chicago, IL).
Results
The mean insulin concentrations were similar across dwell times for each solution bag and closely approximated the desired solution concentrations (Table 1). For each solution, dwell time did not significantly affect mean tubing concentration (Table 1 and Fig. 1).
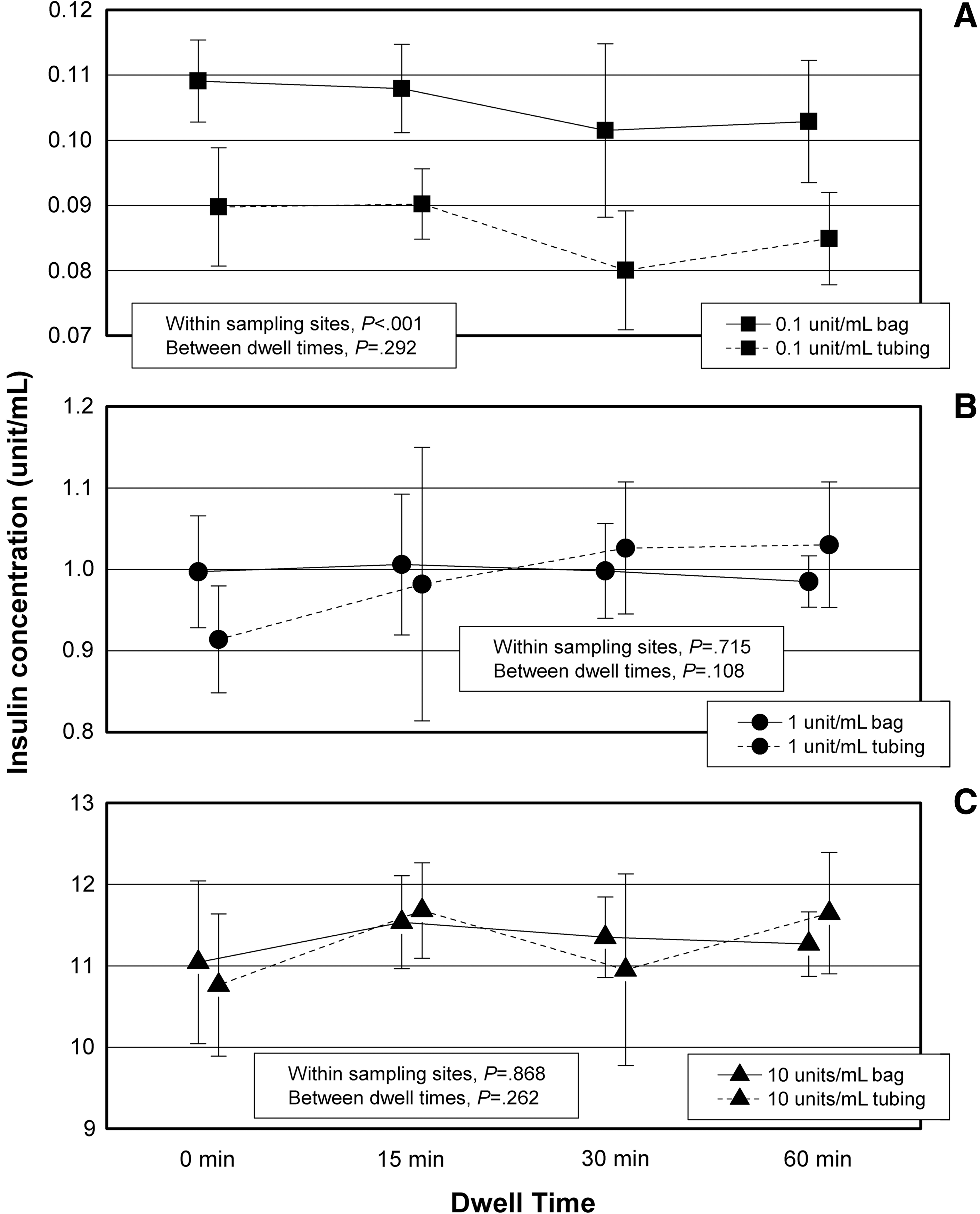
Relationship between insulin concentration and dwell time:
Data in columns 2 and 3 represent the mean±SD values from five experiments. Column 4 represents the mean tubing concentration normalized to the mean solution bag concentration expressed as a percentage±SD.
The trajectories of the tubing concentrations, compared with the solution bag concentrations, were different for each insulin solution concentration (Figs. 1 and 2). For insulin at 0.1 unit/mL, the mean tubing concentration was 82±5% of the bag at all time points (P=0.557). The difference between tubing and solution bag concentration was significant (P<0.001). At 60 min of dwell time, the tubing concentration remained significantly different from the solution bag concentration. For insulin at 1 unit/mL, the mean tubing concentration was 92±10% at 0 min, increasing to 97±12% at 15 min and 103±9% at 30 min. The difference in tubing concentrations across dwell times was not significant (P=0.207). Finally, for insulin at 10 units/mL, the mean tubing concentration was 100±9% of the solution bag at all time points, and there was no significant difference in the tubing concentration across dwell times (P=0.625).
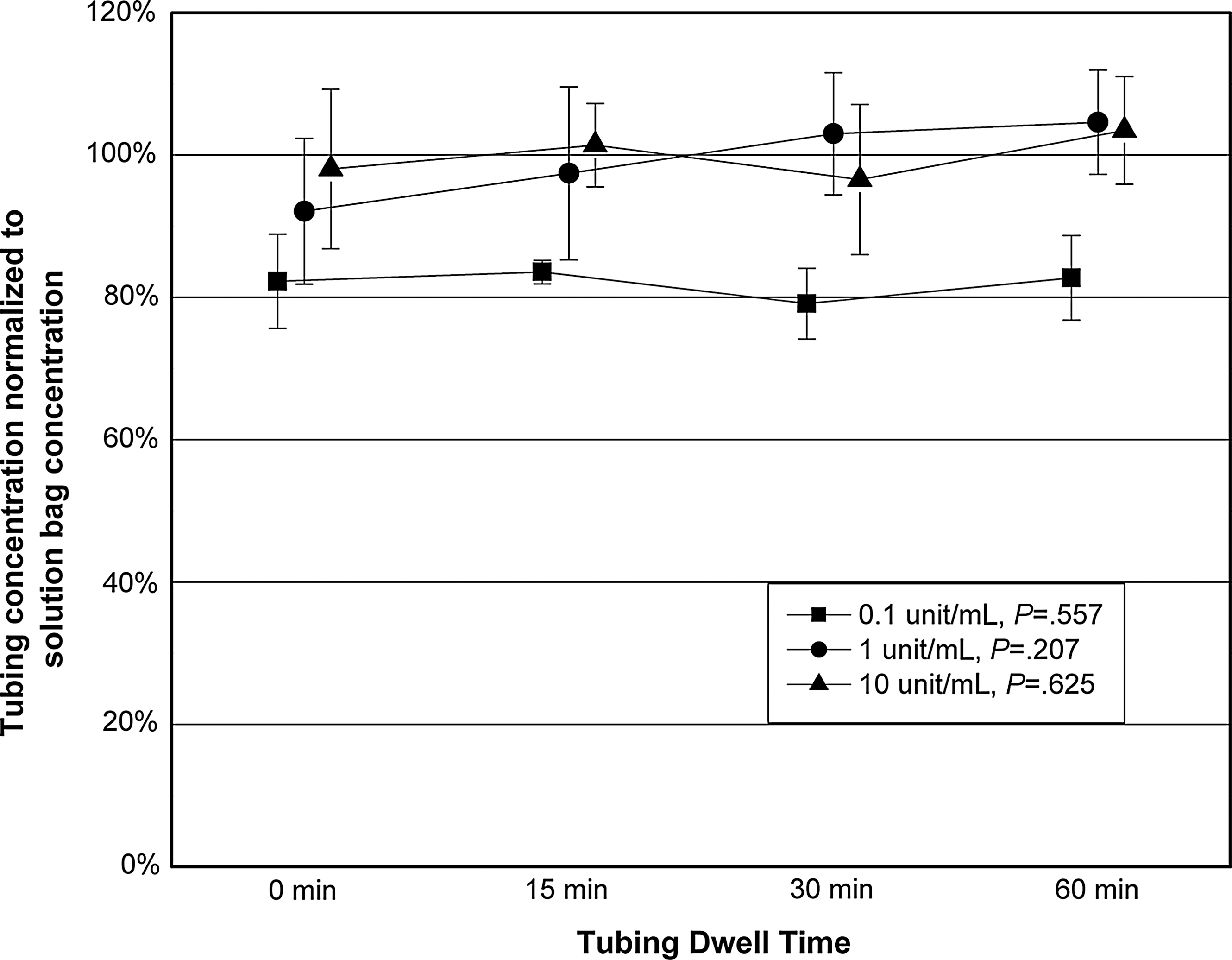
Relationship between the normalized mean tubing insulin concentration to solution bag insulin concentration and dwell time.
Discussion
In this in vitro study comparing insulin concentrations with different dwell times, we report that dwell time did not affect insulin adsorption in polypropylene intravenous infusion sets. Mean insulin concentrations from the infusion set tubing, compared with solution bag concentrations, were not significantly different from 0 to 60 min of dwell time.
Our study investigated the effect of dwell time, in addition to flushing, on insulin adsorption. Prior studies have not investigated the effect of the duration of dwell time on insulin adsorption. For example, Hewson et al. 5 showed improved insulin delivery from tubing prepared by flushing with either 20 mL of solution or dwelling solution for 60 min followed by a flush compared with “control” tubing that was not prepared in any fashion. Our results suggest that flushing alone achieves maximal tubing concentration and that dwelling does not have any additional benefit.
The trajectories of the tubing insulin concentrations were different across the three concentrations. In contrast to the higher concentrations, we only achieved approximately 80% of the solution bag concentration for insulin at 0.1 unit/mL. This suggests continued adsorption losses even after a 60-min dwell. It is likely that polypropylene tubing, like other plastics, has a finite number of binding sites that are not saturated after 60 min with insulin at 0.1 unit/mL. 8,12,13 Saturation of all binding sites may be achieved with dwell times longer than 60 min; however, this is not practical in clinical practice. Solutions with higher insulin concentrations can saturate all binding sites within tubing with shorter dwell times. 8,12,13 Flushing the tubing with a higher concentration before using insulin at 0.1 unit/mL may decrease insulin adsorption as described by Fuloria et al. 12 However, we are concerned this practice may lead to medical errors with the use of two different concentrations of insulin solution and did not test this method in this study.
In this study, we recreated clinically applicable conditions by using insulin concentrations most often used in practice. We accounted for errors in solution preparation by measuring solution bag concentrations. Dilutions with proprietary buffer were also performed immediately upon sample collection and were performed in glass vials that prevent further insulin adsorption. Certain limitations should be considered. We examined adsorption effects on polypropylene intravenous infusion sets. Other infusion sets and solution bags, made of different types of plastics including polyvinyl chloride, polyethylene, or polyurethane, may have different adsorption properties. We examined the adsorption effects of Novolin R insulin, which is the standard insulin preparation of our institution. Other insulin preparations may have different adsorption properties. Our results are only applicable to the solution concentrations and for the range of dwell times we tested. Based on the trajectories of the tubing concentration, dwell times may be important for solutions of insulin between 0.1 unit/mL and 1 unit/mL. These concentrations are not commonly used clinically and not tested in this study.
Conclusions
In this in vitro study, we conclude that for insulin concentrations of 1 unit/mL and 10 units/mL, tubing dwell time has no effect on insulin adsorption with polypropylene tubing. For insulin concentration of 0.1 units/mL, tubing dwell time of up to 1 h also has no effect on insulin adsorption with polypropylene tubing. However, the amount of insulin delivered is consistently lower than the solution bag concentration, which may have clinical implications. We recommend that following a 20-mL flush, insulin infusions can be started without any dwell time. Removing dwell times will minimize preparation time and will allow for faster initiation of insulin infusion therapy.
Footnotes
Acknowledgments
The authors are grateful to Yale Core Laboratories, specifically Aida Grozsmann, Codruta Todeasa, and Ralph Jacob, for technical support and assistance. They are also grateful to Veronika Northrup for statistical support. This research is partially supported by Training Grant NIH T32 HL07272, The Development of Cardiovascular and Pulmonary Function (CT), from the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.