
Abstract
Background:
This pilot trial was designed to determine if an optimal dose of Technosphere® insulin (TI) inhalation powder (MannKind Corp., Valencia, CA) could be used regardless of variation in meal carbohydrate (CHO) content.
Subjects and Methods:
In total, eight subjects (seven men, one woman) with type 2 diabetes were enrolled. Subjects underwent dose optimization meal challenge (MC) visits (100% CHO) and MCs with varied CHO meal contents (50%, 200%, and 0% calculated CHOs). Primary end point was change in postprandial glucose (PPG) excursions. Baseline demographics were 60±7 years of age, diabetes duration of 12.3±4.27 years, hemoglobin A1c (A1C) of 7.82±1.04%, and body mass index of 31.3±5.48 kg/m2.
Results:
Maximum mean PPG excursions for the nominal 100% CHO meals were −13±15 mg/dL for breakfast (B) and −14±15 mg/dL for lunch (L), similar to those after 50% CHO meals (B, −17±16 mg/dL; L, +14±10 mg/dL). The largest excursions occurred during 200% CHO meals and remained below American Diabetes Association targets (B, +19±16 mg/dL; L, +32±29 mg/dL). During 15 of the MCs, subjects took their usual TI dose and then had no meal (0% CHO). For the 0% CHO MCs, the largest mean PPG excursion were −33±9 mg/dL at 60 min (B) and −31±10 mg/dL at 60 and 90 min (L). Mean A1C dropped from 7.82±1.04% at the Week 1 visit to 6.18±0.46% (P=0.00091) at the Week 19 visit.
Conclusions:
Results in eight patients suggest that once an optimal dose of TI is determined, type 2 diabetes patients can ingest meals with a wide range of CHO content or even skip meals without severe hypoglycemia. During this pilot study TI therapy improved A1C by −1.63% (P=0.00091) during 19 weeks of treatment.
Introduction
MannKind Corporation (Valencia, CA) is currently developing Technosphere® insulin (TI) inhalation powder for the control of postprandial hyperglycemia in adults with type 1 and 2 diabetes. TI is composed of recombinant human insulin adsorbed onto Technosphere particles (formed with the excipient, fumaryl diketopiperazine powder). TI particles are sized for inhalation into the deep lung (aerodynamic mass median diameter, 2–3 μm). Once inhaled, TI dissolves upon contact with the lung surface, and the insulin is rapidly absorbed into the systemic circulation with a time to maximum observed concentration of approximately 14 min in subjects with type 2 diabetes mellitus. 4,5 TI formulation has an onset of action profile similar to the physiological first-phase insulin response. Rave et al. 6 compared pharmacokinetics of TI with those of subcutaneously delivered regular human insulin in healthy volunteers and in patients with type 2 diabetes. These studies show that TI has a quick onset of action and short duration (12–17 min, depending on dose) sufficient to cover the meal-related rise in blood glucose. Most of the glucose-lowering effect of TI was delivered in the first 3 h after dosing, thus potentially reducing the risk of late postprandial hypoglycemia.
TI has been shown to be well tolerated by patients unaccustomed to powder inhalation, with only an infrequent incident of mild, self-limiting cough. 7 Few studies have been done comparing TI with subcutaneous standard of care therapy. One large multicenter randomized study compared TI with biaspart (70/30) insulin and with insulin glargine basal regimen in 677 subjects. The study found that the TI group had fewer hypoglycemic events and gained significantly less weight. Both groups had reduced hemoglobin A1c (A1C): −0.68% (TI) and −0.76% (biaspart insulin). 8
We conducted a small pilot study to determine if an optimal dose of TI inhalation powder could be used regardless of variation in meal carbohydrate (CHO) content in patients with type 2 diabetes. The primary objective of the study was to evaluate postprandial glucose (PPG) excursions during optimization and meal challenge visits with CHO contents of 0–200%.
Research Design and Methods
Signed informed consent approved by the Cottage Health Systems Institutional Review Board (Santa Barbara, CA) was obtained from all subjects. Inclusion criteria were age between 18 and 70 years, diagnosis of type 2 diabetes for more than 1 year, no change in diabetes regimen for at least 90 days prior to screening, body mass index of <35 kg/m2, A1C between 6.5% and 9.0%, nonsmoker, and forced expiratory volume in 1 s of >70%. Subjects were allowed to be on oral therapy with or without basal insulin. Exclusion criteria were two or more hypoglycemic episodes in the last 6 months, previous use of any inhaled insulin product, history of chronic obstructive pulmonary disease/asthma, respiratory infection within 30 days of screening, and pregnancy.
Following initial screening and continuous glucose monitoring and MedTone® inhaler (MannKind Corp.) training visits (Visits 1 and 2), patients underwent up to a maximum of four dose optimization visits and up to four meal challenge (MC) visits for each lunch (L) and breakfast (B). To optimize their TI dose, subjects had to achieve a 1-h PPG of <150 mg/dL without 2–3-h PPG hypoglycemia for B and L. Only patients achieving the optimal TI dose proceeded to the MC phase. If subjects experienced hyperglycemia during the initial optimization visit, the dose was increased from 15 U to 30 U of TI, and the MC visit with 100% CHO was repeated. Most subjects were optimized in either one or two visits. Meals were consumed within 10 min after the start of the meal. TI was administered at the start of the meal. If the TI dose was optimized early, subjects could skip the following dose optimization visits. During the dose optimization visits, patients received an MC using 100% CHO content, defined as 50 g of CHOs and a breakdown of calories in a ratio of 40% CHOs, 30% protein, and 30% fat content. Subsequent MC meals consisted of the same protein and fat content with a varying CHO amount (50%, 200%, or 150%). MC with a skipped meal (0% CHO) was done only when deemed safe by the study investigator. Subjects took their usual dose of TI and then had no meal (both B and L MCs). All study visits were 1 week apart with a total of 19 visits/weeks.
During the MC visits, patients received varied CHO content with their optimal dose of TI. Visits 7–10 involved the weekly B MC visits: Visit 7 MC, 50% of the CHO content; Visit 8, MC without a meal (complete meal was skipped), done only if deemed safe by the principal investigator; Visit 9, MC with 200% of the CHO content; and Visit 10, 150% of the CHO content (only if significant hypoglycemia was noted during the 200% meal MC). Visits 11–14 involved equivalent L meal dose optimization visits. Visits 15–18 involved the weekly L MC visits (50%, 0%, 200%, and 150% CHO, respectively). Visit 19 was the follow-up visit.
Patients began taking TI as their preprandial insulin at Visit 3 (dose optimization visit) and took TI with meals on a daily basis throughout the course of the clinical trial. Meal doses were based on optimized dose. Patients came in once weekly for optimization and MC visits. The primary end point was the change in the minimum and maximum PPG from 0 to 240 min, based on venous-drawn blood glucose concentrations measured at −30, 0, 30, 60, 90, 105, 120, 180, and 240 min following each MC. Patients were monitored using DexCom® (San Diego, CA) Seven® continuous glucose monitor sensors throughout the study for 15 weeks. Continuous glucose monitor data were interpreted and reviewed at each visit together with the hypoglycemia diary. A1C values were obtained at Week 1 (Visit 1) and Week 19 (Visit 19).
Statistics were calculated using Student's t test in Excel (Microsoft, Redmond, WA) and the Wilcoxon matched-pairs test.
Results
Seven of the eight enrolled patients (seven men, one woman) with type 2 diabetes completed all eight MCs for L and B. Baseline demographics were 60±7 years of age, duration of diabetes of 12.3±4.27 years, A1C of 7.82±1.04%, and body mass index of 31.3±5.48 kg/m2. One patient completed the first five MCs but exited the study early because of development of sinus bradycardia.
Seven of the eight subjects required one visit for dose optimization for both B and L MCs; one subject required a second optimization visit prior to L MCs. Seven of the eight patients were treated with 15 U of TI (approximately 4 U of subcutaneous rapid-acting insulin) for B and five of the eight with 15 U of TI for L. The remaining patients used 30 U of TI for B and L. Mean PPG excursions for the L and B MCs are depicted in Figures 1 and 2, respectively.

Mean postprandial glucose excursions: breakfast meal challenges. Technosphere insulin and meals were given simultaneously at time 0. CHO, carbohydrate.

Mean postprandial glucose excursions: lunch meal challenges. Technosphere insulin and meals were given simultaneously at time 0. CHO, carbohydrate.
Overall, the range of PPG excursions for all L and B MCs was −33 mg/dL to +32 mg/dL. Maximum mean PPG excursions for the nominal 100% CHO meals were −13±15 mg/dL for B and −14±15 mg/dL for L, similar to those for 50% CHO meals (B, −17±16 mg/dL; L, +14±10 mg/dL). The largest excursions occurred during 200% CHO meals, which remained below American Diabetes Association targets (B, +19±16 mg/dL; L, +32±29 mg/dL). 9 During 15 of the MCs, subjects took their usual TI dose and then had no meal (0% CHO). For the 0% CHO MCs, the largest mean PPG excursions were −33±9 mg/dL at 60 min after B and −31±10 mg/dL at 60 and 90 min after L. One patient began with a fasting plasma glucose of 97 mg/dL, and the blood glucose level fell to 54 mg/dL at 90–120 min. No episodes of severe hypoglycemia (blood glucose of <50 mg/dL) were observed. Mild episodes of symptomatic hypoglycemia were self-treated. Mean A1C dropped by 1.63%, from 7.82±1.04% at Week 1 to 6.18±0.46% (P=0.00091) at the Week 19 visit (follow-up visit). A1C changes for each patient are depicted in Figure 3. A1C change was significant, calculated using the Wilcoxon matched-pairs test showed W=36 and P=0.005. The continuous glucose monitor tracing of a patient before and after starting TI is shown in Figure 4. After initiation of TI (on February 9), reduction of glucose excursions is noted over the course of several days.

Hemoglobin A1c (A1C) change during the study from Week 1 (screening) to Week 19 (follow-up) visit.
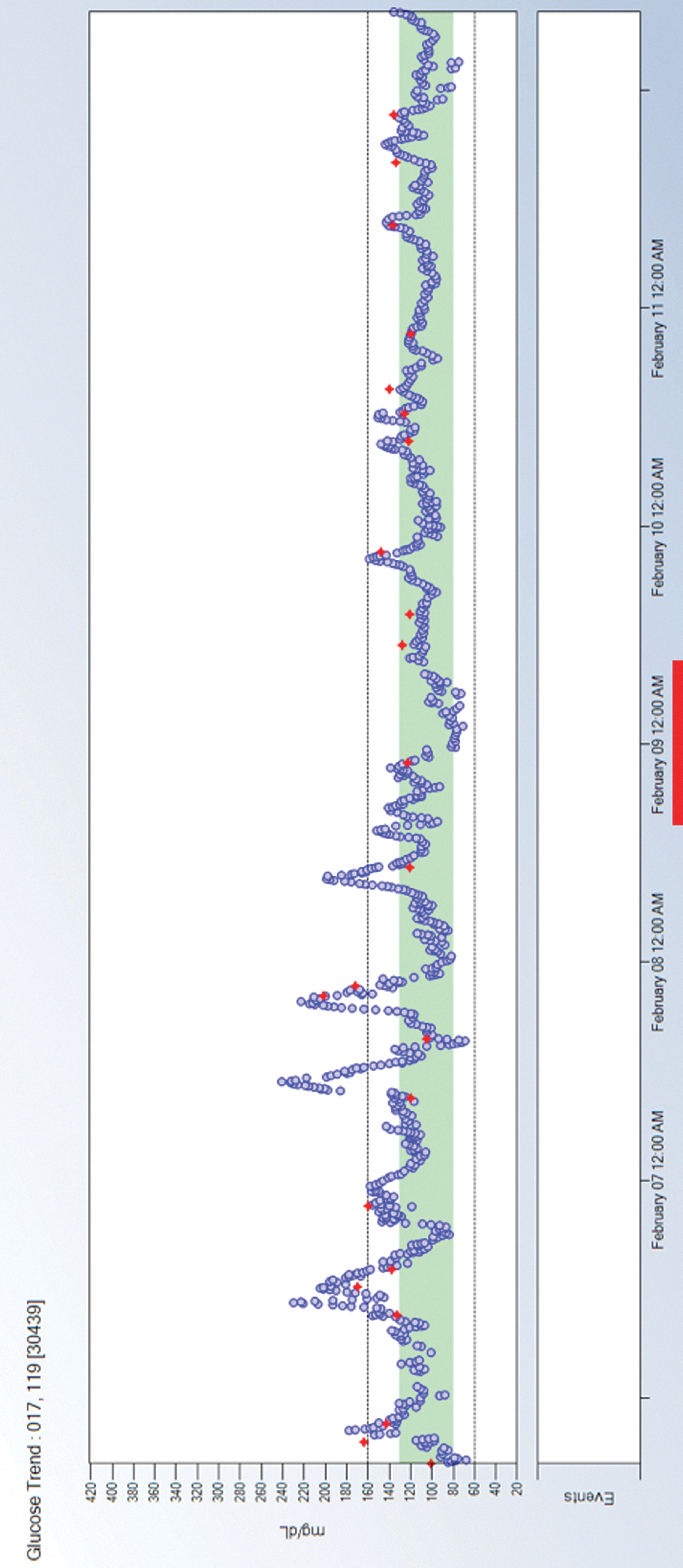
Continuous glucose monitor tracing of a subject before and after starting prandial Technosphere insulin on February 9. The shaded area represents a blood glucose range of 80–130 mg/dL.
Conclusions
A need exists for new treatments for patients with type 2 diabetes that will improve glycemic control and lower the risk of weight gain and hypoglycemia. During this pilot trial in eight subjects, PPG excursions were minimal with an acceptable TI dose and were generally similar across a wide range of CHO content, with the exception of the 200% CHO load, which was higher for the B MC. TI therapy improved mean A1C by −1.63% at Week 19. Preliminary results suggest that once an optimal dose of TI is determined, some patients could take their TI dose, ingest meals with a wide range of CHO content, or even skip meals without severe hypoglycemia.
Footnotes
Acknowledgments
This study was sponsored by MannKind Corporation, Valencia, CA.
Author Disclosure Statement
H.Z. has served as a consultant/advisor for Animas, CellNovo, Insulet, MannKind, and Roche and has received research grant/product support from Animas, Abbott, DexCom, Eli Lilly, GluMetrics, Insulet, LifeScan, Medtronic, Novo Nordisk, Roche, and Sanofi. L.J. has served on an advisory board and/or received honoraria and grant/research support from DexCom, Lilly & Company, Insulet, LifeScan, Medtronic MiniMed, MannKind, Novo Nordisk, Sensys, Amylin, and Pfizer and has receive grant/research support from Bristol-Myers Squibb, Merck, and Sanofi. K.M. declares no competing financial interests exist. R.P. and A.B. are employees and stockowners of MannKind Corporation. P.R. is a previous employee and stockowner of MannKind Corporation. A.M. is an employee, stockowner, and board member of MannKind Corporation. H.Z. is the guarantor of this work and researched data, wrote the manuscript, reviewed/edited the manuscript, and contributed to the discussion. L.J. researched data, wrote the manuscript, reviewed/edited the manuscript, and contributed to the discussion. K.M. wrote the manuscript, reviewed/edited the manuscript, and contributed to the discussion. R.P. researched data, reviewed/edited the manuscript, and contributed to the discussion. A.B. researched data, reviewed/edited the manuscript, and contributed to the discussion. P.R. researched data and reviewed/edited the manuscript. A.M. reviewed/edited the manuscript.