
Abstract
Background:
It has been reported that most pump-treated patients with type 2 diabetes require only two or fewer basal rates. Using daily continuous glucose monitoring (CGM)-directed titration, this premise was re-evaluated at near-normal glycemic control.
Patients and Methods:
Thirty subjects who were insulin-naive (n=10), on basal insulin (n=10), or on basal-bolus insulin therapy (n=10) ate a fixed diet. The basal rate was started as a single rate and then adjusted to a basal glucose goal of 70–130 mg/dL. The insulin-to-carbohydrate ratio (ICR) (in g/U) was adjusted to 2–4-h postmeal CGM glucose goal of 80–120% of premeal glucose.
Results:
The mean (SE) CGM basal glucose was 99.9 (4.9) mg/dL, and 4.5% (1.4%) of the readings were <70 mg/dL. The mean 2–4-h postmeal glucose was 113.3% (4.8%) of the premeal glucose. Only six subjects (20%) required two basal rates, while the remainder needed only one. The mean (SE) dosing relationships were as follows: total basal dose (TBD) (in U/day)=0.226(0.018)×weight (in kg); TBD (in U/day)=0.339(0.012)×total daily dose (TDD) (in U/day); ICR (in g/U)=126(8)/TBD (in U/day); and ICR (in g/U)=365(14)/TDD (in U/day).
Conclusions:
This study confirms that one basal rate is adequate for the majority of subjects with type 2 diabetes. The mathematical proportionality between dosing factors closely agrees with those obtained in CGM-titrated pump-treated type 1 diabetes but differs from those derived from clinical studies in which insulin titration was based on infrequent self-monitored plasma glucose testing and while on an unstructured diet.
Introduction
Previous studies have identified the dose parameter interrelationships in pump-treated 4 and in multiple daily injection-treated 5 type 1 diabetes. Such mathematical formulas aid in the establishing and the evaluation of dosing in these patients. The second purpose of this study was to establish those relationships in pump-treated type 2 diabetes.
Research Design and Methods
This single center study was Institutional Review Board approved and conducted according to the Declaration of Helsinki. In total, 37 subjects with type 2 diabetes meeting the inclusion/exclusion requirements were enrolled in the study and were given written informed consent. Of these subjects, six withdrew before beginning the titration, and one withdrew because of local erythematous nodules at the insertion sites. Of the remaining 30, 10 were on noninsulin therapy, 10 were on basal insulin and other noninsulin therapy, and 10 were on basal-bolus insulin and other noninsulin therapy.
The inclusion criteria were the following: duration of type 2 diabetes ≥3 months; >17 years of age; and glycosylated hemoglobin (A1c) level ≤12% but, in addition, ≥7.0% for those on no insulin treatment despite being on two or more of the following agents for ≥2 months—sulfonylurea, metformin, thiazolidinedione, glitinides, glucagon-like peptide 1 agonist, and/or sitagliptin at one-half of the maximal recommended dose or more. Other inclusion criteria included a creatinine level of <1.5 mg/dL, testing negative for glutamic acid decarboxylase 65 antibodies, self-monitored plasma glucose (SMPG) four or more times each day, and willingness and ability to comply with study requirements.
The exclusion criteria were as follows: severe (requiring the assistance of another) hypoglycemia during the last month; severe cardiac, pulmonary, or cerebral disease; presence of physical, psychological, or cognitive impairments that would interfere with adherence to an intensive insulin therapy program or compliance with the diet, diary keeping, or maintenance of a CGM sensor or pump; pregnancy, nursing, or women who could potentially become pregnant.
At Visit 1 patients signed an informed consent and were evaluated for inclusion and exclusion criteria. Those acceptable subjects received 2 h of carbohydrate counting education (Visits 2 and 3). The subjects were then taught (Visit 4) the operation of an Animas 2020 insulin pump (Animas Corp., a Johnson and Johnson Company, West Chester, PA) and started on a saline infusion. At Visit 5, the subjects were started on insulin, and the noninsulin treatment was discontinued except metformin (n=12) and thiazolidinedione (n=7). All subjects began on a single basal rate. In subjects previously on insulin therapy, the single basal rate was determined by 40% of the total daily dose (TDD) (in U/day). In those not on insulin, the rate was determined by 20% of the weight (in kg). During the next week the subjects were seen twice during office visits to adjust the basal rate and bolus dosing factors based on four SMPG per day (before meals and at bedtime) or for hypoglycemic symptoms. In addition, the subjects received telephone calls between these visits for pump problems or dosing questions.
After approximately 10 days the subjects reported to the clinic where an iPro® sensor (Medtronic, Northridge, CA) was inserted per the manufacturer's recommendations. In addition, the subjects were started on an isocaloric diet (each meal of equal calories and 50% carbohydrate, 30% fat, and 20% protein). Food eaten, timing, glucose tablets taken, SMPG results, and bolus insulin taken were recorded in a self-diary.
Each day thereafter, the subjects returned to the clinic at which time the CGM data were downloaded. The download, diary, and subject exam were reviewed by an investigator, and the basal rate and bolus-dosing factors were adjusted to achieve a basal glucose level of <130 mg/dL, with fewer than 10% of the readings during the 24-h period <70 mg/dL. With each visit, the insulin-to-carbohydrate ratio (ICR) (in g/U) was adjusted by the investigator, if needed, to achieve a CGM glucose concentration of 80–120% of the premeal glucose within 2–4 h postmeal. The starting ICR was determined by the formula: ICR=100/total basal dose (TBD). With each ICR adjustment, the correction factor (CF) (in mg/dL/U) was also changed according to the following formula: CF=4.5×ICR. 4 The CF was not independently evaluated. Glucose tablets (4 g per tablet) were taken for symptomatic hypoglycemia associated with an SMPG <70 mg/dL.
The basal glucose during a meal period, beginning with the usual mealtime and ending after 4 h, was ascertained by omitting a meal each day in the sequence of dinner, lunch, and then breakfast. Prior to all meals that were eaten, a dose of insulin lispro was given based on the premeal SMPG and meal carbohydrates to be consumed. Because the subjects consumed the same amount at each meal, the investigator set the dose of insulin for the meal carbohydrates.
The duration of each visit was about 30 min. The basal day was selected when the subject had obtained the basal glucose goal for ≥2 days on a constant basal rate, <5% of the CGM glucose readings were missing, and the correlation between the SMPG and the CGM glucose readings was >0.80. The full 24-h basal glucose tracing was obtained by substituting a 4-h omitted meal period for a meal eaten during the selected basal day.
The total duration of the study was approximately 4 weeks. Subjects were on pump treatment for approximately 2 weeks. The pump dosing adjustments were guided in the first week of this latter period by SMPG and in the last week by CGM.
For all results the mean, SD or SE, and range were determined. Tests of significance were one-tailed, two-samples of equal variance t test.
Results
Of the 30 subjects studied, 15 were female. The mean (SD) age was 55.9 (12.7) years, the duration of diabetes was 12.4 (7.0) years, A1c level was 7.97% (1.02%), random C-peptide level was 2.47 (1.21) ng/mL, body mass index was 34.6 (6.6) kg/m2, and weight was 96.6 (19.4) kg. Noninsulin treatment consisted of metformin (n=18), sulfonylurea (n=9), thiazolidinedione (n=7), and glucagon-like peptide 1 agonist (n=4).
Missing data during the 24-h selected tracing were <1%. The correlation coefficients for data comparing SMPG to CGM readings were >0.80. Other than mild hypoglycemia (SMPG of <70 mg/dL with symptoms of hypoglycemia but not requiring the assistance of another person), there were no adverse events except the local insertion site reaction noted in one excluded subject. The weight at the end of the study—96.7 (18.1) kg—was not significantly different from that at the beginning (P=0.433).
The 24-h basal glucose target was <130 mg/dL with fewer than 10% of the readings <70 mg/dL. This goal was achieved in all subjects with a single basal rate except six (20%). In these, two basal rates were required. The 24-h mean (SE) CGM basal glucose was 99.9 (4.9) mg/dL. Of the 30 subjects' basal day, 4.5% of the readings were <70 mg/dL, and 12.4% of the readings were >129 mg/dL. Thus, 83.1% of the readings were within the target range of 70–130 mg/dL. The mean 2–4-h post-meal glucose was 113.3% (4.8%) of the premeal glucose. The final TDD was 64.1 (27.6) U/day, the final TBD was 22.3 (11.7) U/day, the final ICR was 6.5 (2.2) g/U, and the final CF was 29.3 (10.0) mg/dL/U.
Of the six subjects who required two basal rates, the time period of the rate increase averaged 2400 h–0700 h with a mean increase of 42% over the baseline basal rate (i.e., a mean rate of 0.98 U/h increased to 1.38 U/h). Even after the basal glucose goal was achieved, a dawn phenomenon could still be seen as a slight increase (20 mg/dL) but statistically significant (P=0.00126) in the basal glucose from 0400 h to 1000 h (Fig. 1). Because of the small number of subjects in the two-rate group, meaningful baseline comparisons with the one-rate group were not possible.
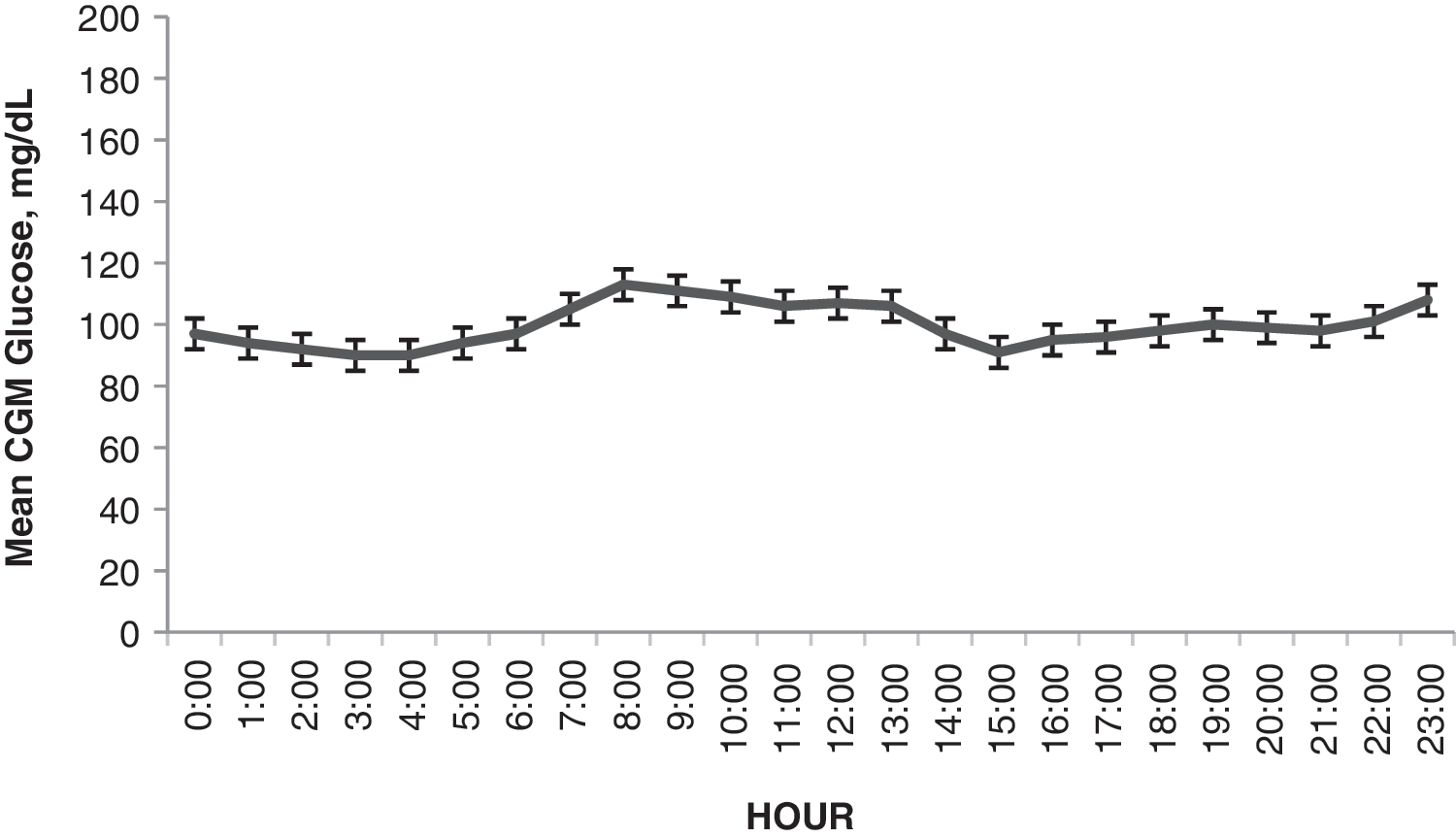
Hourly mean and SE of the continuous glucose monitoring (CGM) basal glucose in 30 type 2 diabetes subjects treated with an insulin pump by one (n=24) or two (n=6) basal rates. The full 24-h basal glucose readings were obtained by once-daily meal omissions and then cutting and pasting the omitted meal periods onto the chosen basal day.
At near normal glucose control, the dosing relationships are seen in Table 1 and are compared with similar studies done with pump-treated and multiple daily dose–treated type 1 diabetes and once-nightly detemir-treated type 2 diabetes.
Data for pump-treated subjects with type 1 diabetes (T1D), multiple daily injection (MDI)-treated T1D patients, and type 2 diabetes (T2D) patients treated once-nightly with insulin detemir were derived from King, 4 King et al., 5 and King, 9 respectively.
ICR, insulin-to-carbohydrate ratio; NA, not applicable; TBD, total basal dose; TDD, total daily dose.
Conclusions
An insulin pump has advantages over multiple daily injections of depot insulin. It delivers accurate amounts of insulin at a continuous rate to control glucose when meals are skipped and during sleep. When the patient enters accurate information, it provides accurate dosing for meals and corrections for episodic hyperglycemia. It has the added advantage of having insulin always with the patient.
In contrast to type 1 diabetes, the onset of type 2 diabetes occurs at an older age when complicated dose setting may be more difficult. In addition, practitioners who care for these patients may not have the sophistication for setting a complex basal rate or insulin bolus doses.
In a 16-week, multicenter study, Edelman et al. 1 demonstrated that 88% of type 2 diabetes subjects could be treated with the simpler basal pattern of only one or two basal rates. During seven visits the basal rate was adjusted to an episodically measured basal SMPG goal of 70–130 mg/dL and a bolus goal of <180 mg/dL at 1.5–2 h postmeal. However, the mean glucose achieved was 139 mg/dL fasting and 201 mg/dL postmeal. Fifty-nine percent of their subjects had at least one episode of hypoglycemia. With very similar baseline subject characteristics but a different study design, including a controlled diet and only 2 weeks on insulin pump treatment, we achieved a basal glucose of 99.9 mg/dL and a 2–4-h postmeal glucose of 113% of the premeal glucose. Only 4.5% of the CGM glucose readings during fasting were <70 mg/dL. Nevertheless, the outcomes of the two studies were the same. Most patients' type 2 diabetes can be controlled by only one or two basal rates. In contrast, pump-treated type 1 diabetes requires two to five basal rate changes per day. 3
A major reason for the need for more than one basal rate is the dawn phenomenon. This phenomenon is predominantly due to liver insulin resistance and increased hepatic gluconeogenesis. 6 The resulting hyperglycemia begins around 0400 h and peaks at 1000 h, thus requiring an increase in the basal rate before its onset. 7 We did detect a slight rise in the glucose during these hours in our subjects but were able to maintain the mean goal glucose <130 mg/dL with a single basal rate in the majority of patients. In those subjects who did require a second basal rate, the rate increase coincided with the timing of the dawn phenomenon. We would hypothesize that most type 2 diabetes patients have an advantage over type 1 diabetes patients in that their residual beta-cell function can match this earlier morning insulin resistance demand.
In contrast to Edelman et al., 1 our dosing relationships were much different. In their study, TBD (in U/day)=0.51×weight (in kg), and TBD (in U/day)=0.55×TDD (in U/day). In a very similar study population of pump-treated type 2 diabetes patients, Raskin et al. 8 reported TBD (in U/day)=0.3×weight (in kg), and TBD (in U/day)=0.5×TDD (in U/day). In both of these studies the dosing was titrated by intermittent SMPG, and the subjects were on an unstructured diet. With a structured diet and careful and intense titration with CGM, we find markedly different dosing relationships (see Table 1). Even in a nonstructured diet but no food after 1800 h and with CGM daily titration of once-nightly basal analog insulin in type 2 diabetes, TBD=0.27×weight (in kg). 9 Recently published studies of hospitalized type 1 diabetes patients 10 and closely monitored outpatient children 11 support TBD (in U/day)=< 0.4×TDD (in U/day). Clearly, with the higher insulin resistance in type 2 diabetes, the absolute dose levels will be greater, but the dosing proportionality remains similar between type 1 and type 2 pump-treated diabetes patients.
In the majority of patients with type 2 diabetes, one basal rate can provide near normal basal glucose control. This would make pump design simpler and give greater ease in setting dosing parameters for practitioners.
Footnotes
Acknowledgments
This study was funded by Animas Corporation and the Diabetes Care Center, Salinas, CA.
Author Disclosure Statement
A.B.K. has received speaking fees and research funding from Animas Corporation, Lilly Corporation, Sanofi, Novo Nordisk, Medtronic, and Dexcom. D.C. and G.S.W. have no competing financial interests.