
Abstract
Background:
To optimize insulin dose using insulin pump, basal and bolus insulin doses are widely calculated from total daily insulin dose (TDD). It is recommended that total daily basal insulin dose (TBD) is 50% of TDD and that the carbohydrate-to-insulin ratio (CIR) equals 500 divided by TDD. We recently reported that basal insulin requirement is approximately 30% of TDD. We therefore investigated CIR after adjustment of the proper basal insulin rate.
Subjects and Methods:
Forty-five Japanese patients with type 1 diabetes were investigated during several weeks of hospitalization. The patients were served standard diabetes meals (25–30 kcal/kg of ideal body weight). Each meal omission was done to confirm basal insulin rate. Target blood glucose level was set at 100 and 150 mg/dL before and 2 h after each meal, respectively. After the basal insulin rate was fixed and target blood glucose levels were achieved, TBD, CIR, TDD, and their products were determined.
Results:
Mean (±SD) blood glucose levels before and 2 h after meals were 121±47 and 150±61 mg/dL, respectively. TDD was 31.5±9.0 U, and TBD was 27.0±6.5% of TDD. CIR×TDD of breakfast was significantly lower than those of lunch and supper (288±73 vs. 408±92 and 387±83, respectively; P<0.01).
Conclusions:
CIR has diurnal variance and is estimated from the formula CIR=300/TDD at breakfast or CIR=400/TDD at lunch and supper in type 1 diabetes patients. These results indicate that the insulin dose has been underestimated by using previously established calculations.
Introduction
To optimize the insulin dose using an insulin pump, basal and bolus insulin doses are widely calculated from the total daily insulin dose (TDD). The total daily basal insulin dose (TBD) has been known to be 50% of TDD. 3,4 CIR is widely calculated from the following formulas: CIR=500/TDD 3,4 or CIR=2.8×body weight (BW) (in pounds)/TDD. 5 We recently reported that basal insulin requirement is approximately 30% of TDD. 2 This means that the bolus insulin requirement is more than previously estimated. The aim of this study is to improve the CIR estimation formula. We therefore investigated here the CIR in type 1 diabetes patients who use an insulin pump after adjustment of the proper basal insulin rate. 2
Subjects and Methods
Subjects
The inclusion criterion is that a patient had type 1 diabetes and was admitted to the hospital to adjust or start insulin pump therapy, with no endogenous insulin secretion (serum C-peptide <0.5 nmol/L). Individuals with eating disorders, unstable retinopathy, or pregnancy or those using another medication that affects blood glucose (e.g., steroids) were excluded. Among 61 Japanese patients, 45 were consecutively selected who met the inclusion and exclusion criteria and who signed an informed consent. This study received institutional ethics committee approval. All patients were treated with an insulin pump (Paradigm 712 or 722; Medtronic, Northridge, CA) and rapid-acting insulin such as insulin aspart, lispro, or glulisine. They had been hospitalized in Osaka University Medical Hospital (Osaka, Japan) or Tokushima University Hospital (Tokushima, Japan) for several weeks from July 2007 to November 2011 to adjust insulin pump therapy.
Verification of basal insulin rate
Self-monitoring of blood glucose was performed at least seven times daily (with three meals per day) (premeal, 2 h postmeal, and before sleep) to optimize basal insulin rates. 2 The diabetes meals in all studies were 25–30 kcal/kg of ideal BW, consisting of 50–60% carbohydrate, 15–20% protein, and 20–25% fat, and were prepared by dietitians. Patients' physical activity varied from sedentary to a mildly active state, and moderate to marked activity was limited. Each meal omission test was done to confirm the basal insulin rate. 2,6 In brief, the test was done started at least 4 h after the last bolus shot and also when the premeal blood glucose level was within 80–150 mg/dL. Blood glucose testing was done every hour after the start of the test until the next mealtime or bedtime (when supper was omitted). It was discontinued if the blood glucose level exceeded 200 mg/dL or fell below 70 mg/dL. If blood glucose level changes were within±30–100 mg/dL during the meal omission, basal rates were changed±0.05 U/h from the previous setting. If blood glucose level changes were more than±100 mg/dL during the meal omission, basal rates were changed±0.1 U/h from the previous setting. Tests were repeated until blood glucose levels remained steady during the fasting procedure (within 30 mg/dL of the reading obtained at the onset of the test) of each mealtime.
Bolus insulin determination
Upon verification of the basal insulin rates, bolus insulin was determined by physicians using carbohydrate counting. The CIR in each meal was titrated to adjust premeal and bedtime blood glucose levels to 100 mg/dL and 150 mg/dL at 2 h after each meal. The average of seven-point glucose testing for the final 3 days of study period was collected. Hypoglycemia was defined as blood glucose readings below 70 mg/dL, and the percentage hypoglycemia rate was obtained. Subcutaneous infusion sites were changed every 3 days before a meal. All meals were consumed within 20 min; no additional food or drink was consumed unless required to treat symptomatic hypoglycemia.
Statistical analysis
Demographic data are presented as mean±SD values. Univariate analysis between BW and TDD was analyzed using Pearson's product-moment correlation coefficient. To evaluate BW-based calculation of CIR, 5 (2.8×BW)/TDD was calculated for each patient. Differences in CIR and CIR×TDD between the meals were examined for statistical significance using the Steel–Dwass test because these data were not normally distributed. A P value of<0.05 was considered statistically significant. Statistical analysis was performed on Statcel3 for Excel (2010) (The Publisher OMS, Saitama, Japan)
Results
Characteristics of the study subjects were as follows: gender, 13 males/32 females; age, 39.3±10.9 years (mean±SD) (range, 19–69 years) (range); BW, 124±23 pounds (range, 80–178 pounds) (55.8±10.2 kg [range, 36–80 kg]); body mass index, 21.7±2.9 kg/m2 (range, 14.6–28.7 kg/m2); duration of diabetes, 22.1±12.3 years (range, 2–48 years); duration of pump therapy, 1.5±4.7 years (range, 0–29 years); and hemoglobin A1c, 7.8±1.6% (range, 5.4–12.4%). TDD was 31.3±9.0 U/day (range, 18–50 U/day). TDD was significantly correlated with BW (r=0.527, P<0.0005).
Seven-point blood glucose level averages are shown in Figure 1. The hypoglycemia rate was 8.6±8.9 % (range, 0–38.0%). According to the meal omission, TBD was 8.5±3.0 U/day (range, 3.3–15.3 U/day) and accounted for 27.0±6.5% (range, 15.5–43.8%) of TDD. CIR values of breakfast, lunch, and supper were 9.8±3.2 g/U (range, 5–20 g/U), 13.9±4.5 g/U (range, 7–23 g/U), and 13.3±4.9 g/U (range, 7–25 g/U), respectively. Average CIR was 12.3±3.9 g/U (range, 7.0–21.3 g/U). CIR of breakfast was significantly lower than those of both lunch and supper (P<0.01). The products of CIR and TDD at breakfast, lunch, and supper were 288±73 (range, 162–600), 408±92 (range, 245–675), and 387±83 (range, 198–660), respectively. More than 90% of CIR×TDD values were less than 500, and CIR×TDD of breakfast was significantly lower than that of lunch or supper (P<0.01) (Fig. 2). According to the BW-based calculation, 5 2.8×BW (in pounds)=347.0±63.5 (range, 224–500), and CIR=2.8×BW (in pounds)/TDD=11.7±2.9 (range, 6.6–19.5), respectively. Average CIR was not significantly different from BW-based calculations; however, average CIR was significantly more than CIR of breakfast (P<0.01) and less than CIR of lunch (P<0.01) and tended to be less than CIR of supper (P=0.06).

Seven-point blood glucose profile during the final 3 days of hospitalization in type 1 diabetes patients using an insulin pump: before breakfast (B0), 2 h after breakfast (B2), before lunch (L0), 2 h after lunch (L2), before supper (S0), 2 h after supper (S2), and before sleep (BS). Data are mean±SD values.
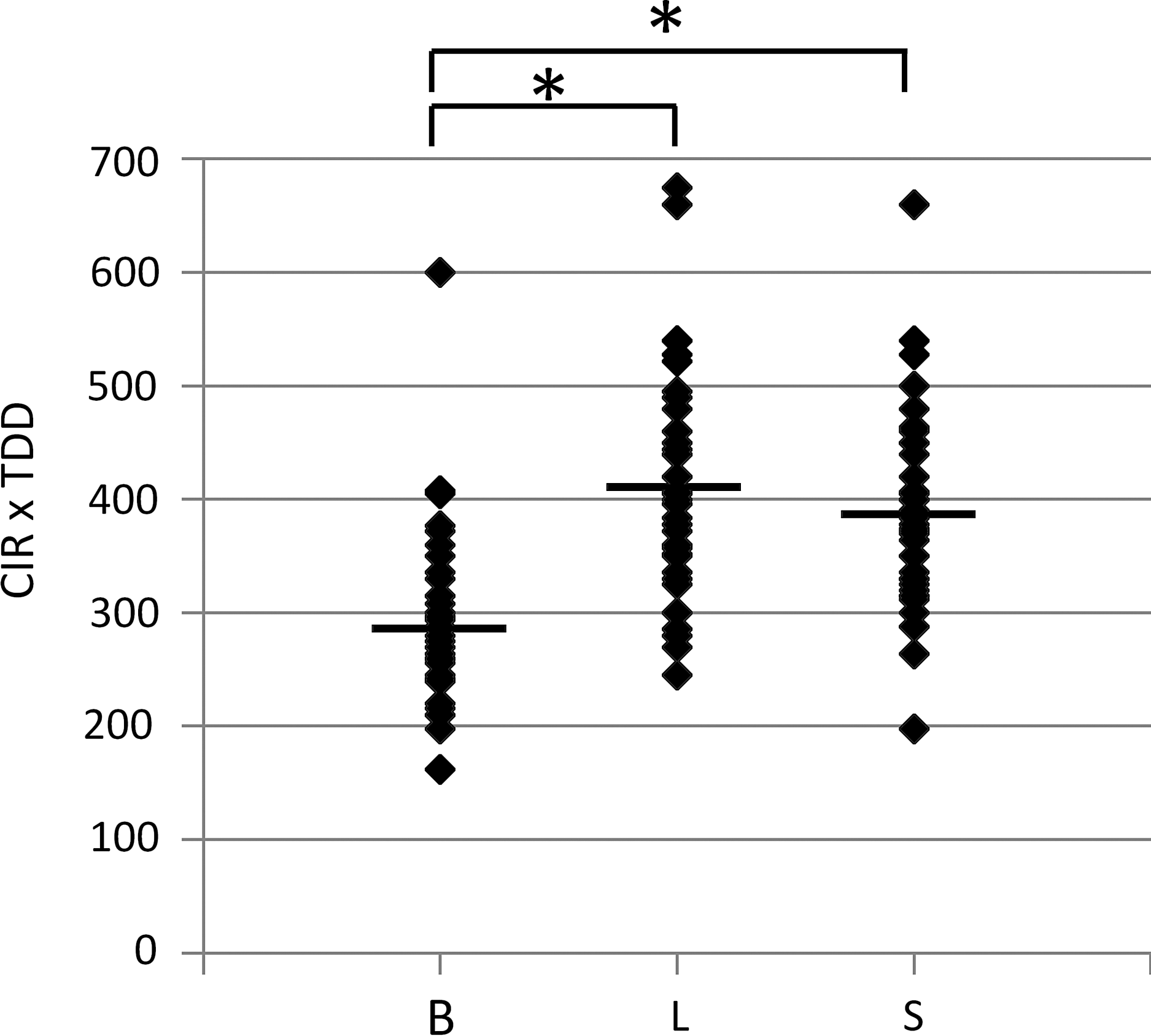
Carbohydrate-to-insulin ratio (CIR)×total daily insulin dose (TDD) in each meal for breakfast (B), lunch (L), and supper (S). Horizontal lines indicate the averages. *P<0.01.
Discussion
We investigated here bolus insulin requirement in C-peptide-negative type 1 diabetes patients who use an insulin pump after the basal insulin rate was properly set. As in our previous report, 2 the basal insulin requirement was 27.0±6.5% of TDD. After the basal insulin rate was adjusted, postprandial glucose variation is mainly dependent on carbohydrate intake and the bolus insulin amount given.
In the present study, we found that CIR was estimated from 300 or 400 divided by TDD at breakfast or at lunch and supper, respectively. CIR determined from our study was lower than that estimated from the commonly used formula, CIR=500/TDD. 3,4 Lower CIR means higher demand for bolus insulin. The reason why CIR was lower than that in the previous common estimation of CIR might be the difference of basal insulin dose. TBD is widely estimated as 50% of TDD, 3,4 whereas it was less than 30% of TDD in our observation. 2 The higher rate of basal insulin rate to TDD might underestimate the bolus insulin rate to TDD. On the other hand, when one starts calculating CIR, using the previous formula CIR=500/TDD seems to be safe because overestimating CIR might prevent hypoglycemia.
Recently, King 1 proposed a formula for CIR in which CIR equals 300 divided by TDD. We agree that CIR of the morning is close to being calculated with this formula. Davidson et al. 5 reported BW-based calculation of CIR in which CIR equaled the product of 2.8 and BW (in pounds) divided by TDD. 5 In this formula, they replaced “500” with “2.8×BW (in pounds),” which takes BW into account for the calculation. If 2.8×BW equals 500, BW is 179 pounds (80.4 kg), which is more than our patients' BW and also more than that of the participants of the Diabetes Control and Complications Trial. 7 Because TDD was significantly correlated with BW, the BW-based formula seems to be more reliable rather than the simple formula of CIR=500/TDD. In fact, the averaged CIR in this study was similar to the CIR calculated from the formula of Davidson et al. 5 However, CIR has diurnal variance, as shown in Figure 2. The product of CIR and TDD at breakfast was significantly less than that at lunch and supper. Such diurnal variance of CIR may be caused by nocturnal elevation of plasma cortisol concentration. 8 Therefore, the formulas proposed by both King 1 and Davidson et al. 5 could not be applied to patients simply. A similar diurnal tendency of CIR was reported in type 1 diabetes patients given a multiple daily insulin injection regimen. 9 Taken together, it is better to calculate the CIR in each meal individually, or we have to think about the fact that the CIR in the morning is lower than that of lunch and supper.
Our results were investigated in only adult Japanese type 1 diabetes subjects who used an insulin pump. It is possible that the difference of the basal and bolus insulin infusion dose may be influenced by the difference of ethnicity and food between Japanese and other races. Although macronutrient contents of Japanese food are close to the dietary reference intake recommendations of the Institute of Medicine, 10 Japanese food contains more carbohydrate and less fat compared with Western foods. In addition, hospitalization and strict diet might affect the diurnal variance of CIR. In pediatrics, pregnancy, and type 2 diabetes with multiple daily insulin injections, these formulas may not apply. Also, this study is small in size and is not designed as a randomized study comparing different CIR×TDD.
In conclusion, CIR has diurnal variance and is estimated from the formula CIR=300/TDD at breakfast or CIR=400/TDD at lunch and supper in type 1 diabetes patients. These results indicate that the insulin dose has been underestimated by using previously established calculations.
Footnotes
Acknowledgments
This study is supported by grants from the Japan Diabetes Foundation. We acknowledge Kazumi Hata, Tomomi Hirano, and Chikayo Yokogawa for excellent secretarial work.
Author Disclosure Statement
No competing financial interests exist.