
Abstract
Background:
Self-monitoring of blood glucose (SMBG) is a proven tool to improve glycemic control, even if it might increase direct costs for diabetes management. In Italy, the purchase, prescription rules and responsibilities, and distribution of testing strips per type of patient are managed differently in each of the 20 Italian regions. The Italian scientific societies for diabetes (Società Italiana Diabetologia [SID] and Associazione Medici Diabetologi [AMD]) have issued validated guidelines for SMBG, but not all regions apply them. We investigated whether following SID-AMD guidelines would help decreasing SMBG and diabetes healthcare costs in Italy.
Materials and Methods:
We compared the regions applying and not applying SMBG guidelines for the mean number of testing strips used, number of hospitalizations (with the principal diagnosis of diabetes, excluding diabetes complications), and duration of hospitalization, as indirect measures of SMBG cost.
Results:
Regions applying the guidelines recorded higher SMBG testing strip utilization than regions not applying guidelines, but they recorded fewer hospitalizations for diabetes (36.2±11.3 vs. 79.9±27.8 hospitalizations per 100,000 inhabitants, P<0.002) and fewer days in the hospital (363±106 vs. 685±194 days of hospitalization for diabetes per 100,000 inhabitants, P<0.002).
Conclusions:
Our data suggest that application of guidelines for SMBG prescription and a strict cooperation between health providers and regional health economic deciders were associated with greater utilization of SMBG testing strips. They were also associated with significantly reduced number of hospitalizations and reduced overall duration of hospitalization for patients with diabetes, potentially saving healthcare costs.
Introduction
The above-reported evidence compelled several scientific committees to strongly recommend the practice of SMBG to all diabetes patients. The American Diabetes Association 11 suggested that SMBG should be carried out three or more times daily for patients using multiple insulin injections; for patients using less frequent insulin injections or oral agents or medical nutrition therapy alone, SMBG is considered useful in achieving glycemic goals. The Guideline Development Group for the National Institute for Health and Clinical Excellence, in the clinical guidelines for type 2 diabetes, 12 declared that some studies added "considerable confidence to the view that SMBG was an integral part of effective patient education packages and enabled the effective use of many other therapies and lifestyle interventions." In Italy, the Italian scientific societies for diabetes (Società Italiana Diabetologia [SID] and Associazione Medici Diabetologi [AMD]) issued recommendations for diabetes patients whose blood glucose was consistently within the therapeutic goal, advocating different guidelines for SMBG practice according to the hypoglycemic treatment adopted 13 for its possible consequences. 14 These guidelines include recommendations for the use of structured glucose monitoring, largely proved to be effective. 15 –18
Although effective in maintaining good control of blood glucose, reducing glucose variability, 19 and its cardiovascular effects, 20 SMBG increases direct medical costs. 10 Nevertheless, the main costs related to diabetes are due to hospitalizations and to management of complications, 21 –23 thus suggesting that the prevention of hospitalizations and complications would help decrease the overall costs for diabetes.
Almost all European health services cover expenses for SMBG of diabetes patients. In Italy, the healthcare system is regionalized. Although Italian national law provides medicines and free health services in specialized centers to all diabetes patients (Italian law number 115/87), the costs of diabetes treatments are borne by the individual regions, each of which is governed by different regulations for providing assistance to diabetes patients.
Even though national guidelines were issued, 13 regional laws and treatment recommendations and plans often do not comply with them, thus producing regional differences in the type of care available to patients. A survey on the utilization of testing strips in the European countries, published along with the Italian Guidelines, revealed that the Italian per capita utilization is 25–30% below the European average, which may imply inadequate SMBG in Italian diabetes patients. 24 Simply reducing the capital outlay associated with SMBG may increase overall diabetes healthcare costs because of the resulting diabetes complications and hospital admissions for diabetes patients.
Given that, according to Italian law number 115/87, all Italian diabetes patients should have access to the level of care adequate to their personal condition and that regional laws provide different levels of care, the comparison between different regions may be used to understand how the application of recognized guidelines might affect the major clinical outcomes of the management of the diabetes population. Examining this situation might clarify the actual effect of SMBG guideline application and expose a potential healthcare cost saving for the practice of SMBG.
In this study, we explored and compared the different Italian regions in terms of the effect of their SMBG guidelines implementation and testing strip prescription on strip utilization and hospitalization of diabetes patients, which were considered direct measures of economic costs of diabetes in the regions.
Materials and Methods
Regional law collection
If available, regional laws were gleaned from regional Websites. When this resource was not available, local diabetes specialists were invited to present the regulations to be followed for SMBG prescription in their region 25 ; each regulation was then directly confirmed via the regional law archives.
Patients' classification
As per the Italian Standards of Care guidelines, 13 diabetes patients were divided into four groups according to their therapy, with specific instructions for the frequency of SMBG: (1) intensive insulin therapy, SMBG at least four times per day; (2) traditional or combined insulin therapy, SMBG equivalent to the number of insulin injections plus 20%; (3) oral hypoglycemic therapy with hypoglycemia-prone secretagogues, SMBG at least four times per week (at different hours); and (4) diet therapy and/or therapy with insulin-sensitizing drugs, SMBG only if requested by the diabetes specialist.
Outcome measures
Official SMBG usage data in Italy are not available. For this measure, we used reliable 2010 market data from IMS Health Inc. as developed by the Italian National Observatory of Medicine Use and the Italian Drug Agency. However, SMBG testing strip usage does not fully represent the real cost of SMBG because each region or province can purchase reagent strips from the market at different prices. The actual price of strips is the result of a commercial negotiation, independent of guideline application. Hence, the mean number of reagent strips per person per year was chosen as the most representative measure of SMBG cost.
Number and duration of hospitalizations were gathered from the official database published online from the Italian Ministry of Health, 26 and the mean number of hospitalizations (normalized per 100,000 regional inhabitants) multiplied by the mean duration (days) of hospitalizations was used as a measure of the cost of hospitalization. We only included hospitalizations with a principal diagnosis of diabetes, according to ICD-9-CM 285-294-295, 27 which is representative of diabetes decompensation. We included only this diagnosis because hospitalizations for diabetes complications are often improperly reported.
Data analysis
Regions were divided into two groups, according to whether Italian SMBG guidelines were applied or not. Four regions were excluded because Italian guidelines for SMBG prescription were applied differently in each province within the same region. One other region was excluded for missing data on hospitalizations. Thus data from 15 regions were finally analyzed. Student's t test was applied to estimate statistical significance; P<0.05 was considered as statistically significant.
Results
In Italy, the mean number of reagent strips used for SMBG in diabetes was 252 strips per patient per year (about 0.69 strip per day per patient).
Eight of the 15 regions analyzed (53%) (Fig. 1) were following SID-AMD Italian SMBG prescription guidelines. The annual usage data for reagent strips for SMBG was available for six of those eight regions (Fig. 1); it ranged from 225 to 468 strips per year per person, with a mean±SD of 342±81 strips per year per patient, corresponding to less than 1 strip per day per patient (approximately 0.94 strips per day per patient). Annual number of hospitalizations for diabetes in these regions was 36.2±11.3 per 100,000 inhabitants, with a mean duration of 10.2±2.4 days per hospitalization (Fig. 1). Total duration of hospitalization for diabetes (number of hospitalizations×days of hospitalization) per 100,000 inhabitants was therefore 363±106 days.
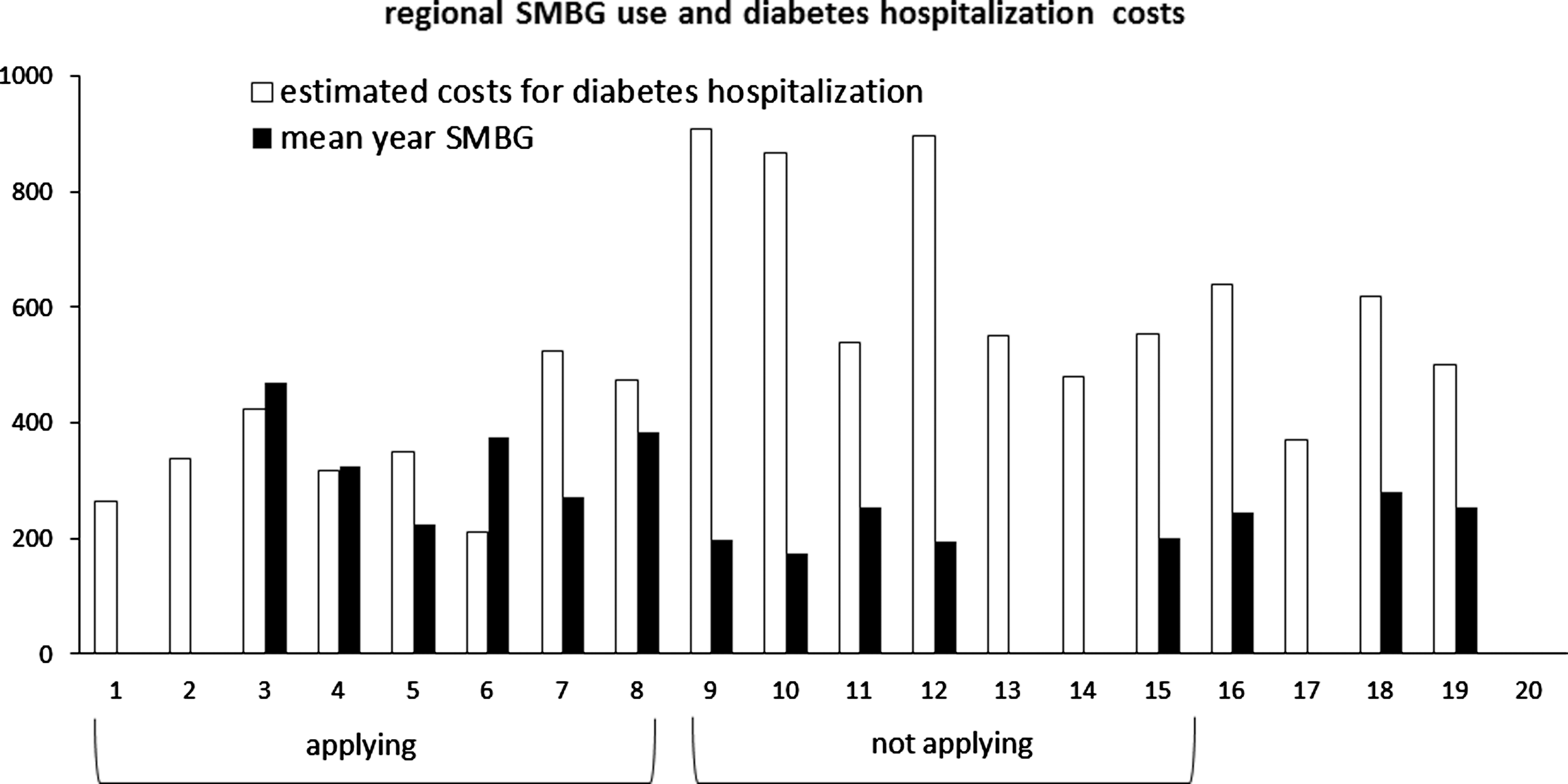
Regional comparison of the application of Italian guidelines for self-monitoring of blood glucose (SBMG): hospitalization duration (open columns) and mean number of SMBG strips per person per year (solid columns).
Seven of the 15 regions analyzed (47%) (Fig. 1) were not following Italian SMBG prescription guidelines. The annual usage of reagent strips for SMBG was available for five of those seven regions; it ranged from 175 to 250, with a mean±SD of 205±29 strips per year per patient (Fig. 1), which correspond to much less than 1 strip per day per patient (approximately 0.56 strips per day per patient). Annual number of hospitalizations for diabetes in these regions was 79.9±27.8 (per 100,000 inhabitants), which was significantly higher (P<0.002) than in the regions following the Italian guidelines. Mean hospitalization duration was 8.8±1.6 days per hospitalization; the difference in hospitalization duration between regions following or not following the Italian SMBG guidelines did not reach statistical significance. Total duration of hospitalization for diabetes (number of hospitalizations×days of hospitalization) per 100,000 inhabitants was therefore 685±194, which was significantly higher (P<0.002) than in the regions following the Italian SMBG guidelines.
Discussion
Our data strongly suggest that the application of guidelines for the prescription of SMBG strips to diabetes patients is associated with a significant reduction in the hospitalization of these patients. Guidelines application led also to an increased use of SMBG reagent strips and SMBG-related costs. Because the main costs for diabetes are related to hospitalizations and management of complications, the increase of SMBG-related costs is largely compensated for by the hospitalization decrease, which would likely translate into reduced healthcare costs of diabetes.
Although it is now clear that use of SMBG reagent strips can reduce the burden of hyperglycemia 28 and complications in patients with diabetes, their cost compels health administrators to regulate their prescription. Therefore, several scientific societies, including the American Diabetes Association, 11 the British National Institute for Health and Clinical Excellence, 12 and the SID-AMD, 13 issued guidelines recommending SMBG prescription according to the scientific evidence, as well as a patient's therapy, while taking into account the necessity to reduce strip prescription to the minimum.
Precise statistics on diabetes treatment in Italy are not available, but it has been estimated, from a large Italian database, 29 that ≤30% of patients are insulin treated. Guidelines recommend a mean of 4 strips per day for insulin-treated patients and 4 strips per week for non–insulin-treated patients, which would give a mean utilization of 1.6 strips per day. Although this represents a limited number of glucose determinations, the guidelines suggest this is adequate and efficient. This estimate is actually slightly lower than the number of strips directly measured in Norway. 30
Despite the guideline recommendations, several Italian regions provide a maximum number of SMBG testing strips per patient per day, without taking into account a patient's treatment regimen. This results in an excessive number of SMBG strips being provided, with the risk of cost excesses, for the majority of patients (i.e., non–insulin-treated), whereas a minority of patients (i.e., insulin-treated diabetes patients) would not have enough strips to adequately monitor their blood glucose levels. Hence, in these patients, the frequency of complications and hospitalizations might increase, thus contributing to overall increased costs.
Our data suggesting that regions not applying SMBG guidelines had a trend toward shorter hospitalization duration, but a higher number of hospitalizations of diabetes patients (patients discharged with a principal diagnosis of diabetes), warrant further explanation.
First, it might be argued that discharges with a diagnosis of ICD-9-CM 285-294-295 do not represent all discharges of diabetes patients. They nevertheless imply that the only cause for the admission of the diabetes patient was glucose decompensation 31 (either hyper- or hypoglycemia), possibly due to the absence of prior adequate SMBG. For example, a patient hospitalized for the treatment of a diabetic foot would be categorized with a diagnosis of ICD-9-CM 271 (skin ulcer), which is a diabetes-related diagnosis. Because chronic complications of diabetes (from diabetic skin ulcers to cardiovascular diseases) require a prolonged period of time to develop, a clear relationship between inappropriate glucose control (i.e., lack of application of SMBG guidelines) and diabetes complications cannot be easily detected. Although these data were not included in this analysis, it could be hypothesized that the inclusion of “diabetes-related” (e.g., diabetic nephropathy or diabetic retinopathy) diagnosis and not merely “diabetes” would increase the differences in outcomes between regions applying and those not applying guidelines.
Second, although the difference did not reach statistical significance, it might appear surprising that regions not applying guidelines actually reported shorter hospitalization durations. However, these regions had a higher number of hospitalizations than regions applying guidelines, and therefore overall hospital duration (a product of the number of hospitalizations and duration of each) was higher, which translates into higher potential costs as well. In addition, it might be speculated that these shorter hospitalizations are likely due to acute glucose decompensation episodes, which are rapidly (and easily) resolved within the hospital but are preventable with adequate SMBG.
Third, it might be argued that the actual prevalence of the different types of diabetes and their different treatments, and therefore the usage of SMBG, could interfere with the results obtained and influence the data on hospitalizations. Several databases, 13 however, clearly demonstrate that the prevalence of the different types of diabetes and diabetes treatment are virtually identical between regions, excluding Sardinia. 32 In addition, diabetes outpatient centers are homogeneously distributed in Italy, as their presence and accessibility are given by law. Differences in hospitalizations might therefore be due to the regional regulations on SMBG guideline application. It is interesting that one region, neither applying guidelines nor imposing SMBG restrictions, posted the highest costs. If the availability of SMBG strips, rather than guideline application, was the cause of reduced hospitalizations, this region would be expected to have lower, not higher, costs. This result, conversely, may confirm that guideline application, rather than SMBG testing strip availability, is the key factor for the reduced hospitalizations and potential costs, possibly through the application of structured glucose monitoring.
Although outside the scope of this study, the stipulation of a mean national strip utilization per diabetes patient per day (0.69) much lower than the one proposed by the Italian guidelines (1.6) deserves some consideration.
First, several regions not following Italian guidelines stipulate a maximum number of strips per diabetes patient per day, regardless of diagnosis or treatment. This allowance might be too low for some patients (e.g., insulin-treated) and too high for others (e.g., metformin-treated); those having too few testing strips for their needs risk acute glucose decompensation, and patients having strips in excess of their needs do not fully use their allowance. Fewer strips are used, and therefore the national mean strip utilization per patient per day (0.69) is less than the guideline-proposed 1.6 strips per patient per day.
Second, the setting of a universal maximum number of strips per patient per day in some regions does not take into account fragile patients, including pregnant women with diabetes, children with diabetes, or patients suffering from acute decompensation from diabetes. These patients represent a small portion of the overall population with diabetes, and temporarily increasing their testing strip allowance to accommodate their condition should not significantly impact on the total SMBG costs.
This study has some limitations. First, it is cross-sectional. Clearly, an interventional study with guidelines application in regions not applying them would be more conclusive, and we suggest that such a study be performed on the basis of this article. Second, increased costs (hospitalizations) in regions not applying guidelines might be influenced by other confounding factors. Diabetes center accessibility (ruled by law) or hospital and drug availability (Italian laws include universal insurance for all diabetes patients) should not represent bias; nevertheless, poor interaction between regional rulers and diabetes (and other) specialists, absence of diabetes patient registries, and other nonrecognizable factors could independently influence both hospitalization costs and SMBG availability. Third, regional guidelines application on SMBG might not represent a really structured (and effective) SMBG approach. 15 However, Italian guidelines 13 include strong recommendations for collaborative (patient–health provider) use of structured SMBG. We might therefore suppose that health providers allowed by (and collaborating with) their own regional rulers were applying both Italian guidelines and the recommended structured glucose monitoring, once again reinforcing the need for regional health ruler–provider cooperation.
Data presented here, although based on the Italian regulations, could be interesting for healthcare organizations outside Italy because this analysis focuses on a situation in which different regional regulations are used for a single population, with identical genetic background and lifestyle habits, as well as identical hospital organization, with full national insurance coverage.
In conclusion, our data strongly suggest that although the application of guidelines for the prescription of SMBG testing strips increased the utilization of testing strips per patient per day, hospitalizations for acute glucose decompensation were reduced, which may result in overall decreased costs for diabetes health care. Guidelines application, with recommended structured glucose monitoring, and strict cooperation between health providers and regional health economic deciders are necessary to reach a sustainable assistance for diabetes.
Footnotes
Acknowledgments
Editorial assistance for the drafting of this article was provided by Sara Marceglia, Ph.D., on behalf of Content Ed Net. The authors received a grant from LifeScan, a Johnson and Johnson Company, to prepare this manuscript.
Author Disclosure Statement
The authors declare that they have no commercial associations that might create a conflict of interest regarding the submitted manuscript.