
Abstract
CME Certification — 1.0 AMA PRA Category 1 Credit(s)™
There is a need for greater caution in interpreting glycated hemoglobin (A1C) results, which can be inaccurate in individual patients for a wide variety of reasons beyond the patient's control. In addition, A1C alone may not reflect critical aspects of glycemia. A panel of clinical experts from Europe and North America was convened to reexamine our glucose measuring tools and determine ways in which they can better be applied toward more purposeful processes of glycemic management. Among the main issues addressed were the clinical situations in which A1C should not be used, the role of alternative biomarkers in identifying aspects of glycemic dysregulation not captured by A1C, and the value of using patients' own glucose data to consolidate therapeutic, educational, and behavior-change objectives.
This activity has been designed to meet the educational needs of physicians and registered nurses involved in the management of patients with diabetes.
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Postgraduate Institute for Medicine, Mary Ann Liebert, Inc., and The Diabetes Education Group. Postgraduate Institute for Medicine is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Postgraduate Institute for Medicine designates this journal-based CME activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
This educational activity for 1 contact hour is provided by Postgraduate Institute for Medicine.
Postgraduate Institute for Medicine is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's Commission on Accreditation.
Initial Release Date: October 15, 2012
Expiration Date: October 15, 2013
Estimated Time to Complete Activity: 1 hour
There are no fees for participating and receiving CME credit for this activity. During the period October 15, 2012 through October 15, 2013, participants must read the learning objectives and faculty disclosures and study the educational activity.
Postgraduate Institute for Medicine supports Green CME by offering your Request for Credit online. If you wish to receive acknowledgment for completing this activity, please complete the posttest and evaluation available online at
This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the Food and Drug Administration. Postgraduate Institute for Medicine, Mary Ann Liebert, Inc., The Diabetes Education Group, and Bayer HealthCare, Diabetes Care do not recommend the use of any agent outside of the labeled indications.
The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of Postgraduate Institute for Medicine, Mary Ann Liebert, Inc., The Diabetes Education Group, and Bayer HealthCare, Diabetes Care. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient's conditions and possible contraindications on dangers in use, review of any applicable manufacturer's product information, and comparison with recommendations of other authorities.
Postgraduate Institute for Medicine assesses conflict of interest with its instructors, planners, managers, and other individuals who are in a position to control the content of CME activities. All relevant conflicts of interest that are identified are thoroughly vetted by Postgraduate Institute for Medicine for fair balance, scientific objectivity of studies utilized in this activity, and patient care recommendations. Postgraduate Institute for Medicine is committed to providing its learners with high-quality CME activities and related materials that promote improvements or quality in healthcare and not a specific proprietary business interest of a commercial interest.
Consulting: Roche Diagnostics, Johnson & Johnson, Abbott Diabetes Care
Contracted Research: sanofi-aventis, Halozyme Therapeutics
Consulting: Roche Diagnostics, Medtronic, Janssen Pharmaceuticals
Consulting: AstraZeneca, Bayer Diabetes Care, Bristol Myers Squibb, Eli Lilly, GlaxoSmithKline, Novo Nordisk, Medtronic, sanofi-aventis
Consulting: Bayer HealthCare Pharmaceuticals
Consulting: Bayer HealthCare Pharmaceuticals, LifeScan, Abbott Laboratories, DexCom, Roche Diagnostics
Consulting: Abbott Diabetes Care, Bayer HealthCare Pharmaceuticals
No relevant financial relationships to disclose
Consulting: Bayer HealthCare Pharmaceuticals
The following Postgraduate Institute for Medicine planners and managers—Trace Hutchison, PharmD; Samantha Mattiucci, PharmD; Jan Schultz, RN, MSN, CCMEP; Laura Excell, ND, NP, MS, MA, LPC, NCC; and Patricia Staples, MSN, NP-C, CCRN—hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
The staff at Mary Ann Liebert, Inc. and The Diabetes Education Group hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
This activity is jointly sponsored/co-provided by Postgraduate Institute for Medicine, Mary Ann Liebert, Inc., and the Diabetes Education Group.
This activity is supported by an unrestricted educational grant from Bayer HealthCare, Diabetes Care.
After completing this activity, the participant should be better able to: • Recognize the potential limitations of A1C when evaluating individual patients • Identify nonglycemic factors, other than methodical inaccuracies, that can falsely raise or lower A1C levels • Enumerate current methods for measuring short-term variations in blood glucose • Utilize patients' own self-monitoring of blood glucose data as a tool for diabetes education • Provide appropriate care and counsel for patients and their families
Media: Online and Print Journal article
By the year 2030, the diabetes pandemic will likely affect more than 10% of the world's population. The personal, public health, and economic crises implicit in this trend call for decisive action. Yet, escalating dilemmas thwart full realization of current therapies. First, controversial studies, such as the Action to Control Cardiovascular Risk in Diabetes (ACCORD) Trial, have amplified calls to individualize glycated hemoglobin (A1C) targets in the absence of adequate infrastructures for supporting personalized care. Second, costlier medications and technologies addressing more nuanced aspects of metabolic dysfunction are expanding options for diabetes management amidst growing disparities between “affordable” and “best” care. Third, common clinical quandaries, such as discrepancies between A1C and self-monitoring of blood glucose data, as well as misconceptions about long-term glycemic assessment, compound entrenched cycles of inadequate self-care, delayed intervention, and suboptimal glycemic outcomes. Because individual, clinical, and public policy responses to these conflicting forces are based largely on methodologies for glucose measurement, a panel of clinical experts from Europe and North America was convened to reexamine our glucose measuring tools and determine ways in which they can be better applied toward more purposeful processes of glycemic management. Among the main issues addressed were the need for caution in interpreting A1C for individual patients, the role of alternative biomarkers in identifying aspects of glycemic dysregulation not captured by A1C, and the value of using patients' own glucose data to consolidate therapeutic, educational, and behavior-change objectives.
Introduction
The Diabetes Control and Complications Trial (DCCT) 4 and the United Kingdom Prospective Diabetes Study 5 marked the ascendancy of A1C as the “gold standard” of glycemic management. Published in the 1990s, these trials confirmed the hypothesis that complication risk in type 1 and type 2 diabetes, respectively, increases exponentially with elevations of mean blood glucose (assessed using A1C). Although numerous treatment guidelines have since codified the finding that improving diabetes outcome is a continuum, with benefit accruing for any reduction in A1C, the path toward optimal glucose control is becoming increasingly ambiguous for the following key reasons. 6 –12 First, controversial studies, such as the Action to Control Cardiovascular Risk in Diabetes (ACCORD) Trial, have amplified calls to individualizing A1C targets, but without the necessary infrastructures for supporting patient-particular care. 13,14 Second, costlier medications and technologies addressing subtler aspects of metabolic dysfunction are expanding options for diabetes management amidst growing disparities between “affordable” and “best” care. 15 Third, common clinical quandaries, such as discrepancies between A1C and self-monitoring of blood glucose (SMBG) data, as well as oversimplified expectations of methodologies for long-term glucose assessment, compound entrenched cycles of inadequate self-care, delayed intervention, and suboptimal glycemic outcomes. 16,17
Because individual, clinical, and public policy responses to these conflicting forces are based largely on traditional views of glucose measurement, a panel of clinical experts from Europe and North America was convened to reexamine our glucose measuring tools and determine ways in which they can be applied to encourage decisive processes of glycemic management across healthcare systems. Among the main issues addressed during the February 2012 conference in Barcelona, Spain, were the need for caution in interpreting A1C for individual patients, the role of alternative biomarkers in identifying aspects of glycemic dysregulation not captured by A1C, and the value of using patients' own glucose data to consolidate therapeutic, educational, and behavior-change objectives. A summary of the discussion and ensuing recommendations follows.
Overcoming Uncertainties of A1C: The Role of Complementary Biomarkers
A1C, or the fraction of hemoglobin bound (glycated) to glucose, has been the standard laboratory assessment of glycemic control and the premier marker of short- and long-term diabetes complication risk for more than 30 years. The test serves as a practical method for estimating average glycemia over the preceding 60–90-day period. Although recommended targets are generally 6.5–7.0%, the question of why certain patients under “good” metabolic control, as indicated by A1C, develop complications while certain others with ostensibly poorer control remain complication-free has yet to be answered. 18 Indeed, although random allocation to intensified glycemic therapy in the DCCT reduced the risk of sustained retinopathy progression by 73%, A1C and duration of diabetes (glycemic exposure) explained only about 11% of the variation in retinopathy risk for the entire study population, leaving the remaining 89% open to conjecture. 19,20
The pitfall of extrapolating from such population-based assessments of glycemic control when advising individuals “in the exam room” is exemplified by a recent chart review in which 9% of 600 consecutive patients had conditions that would preclude the use of A1C. 21 This evidence quite possibly represents the tip of the iceberg considering that 80% of subjects were white, and variances of hemoglobin known to unpredictably interfere with A1C occur more typically among African Americans, Hispanics, and Asian/Pacific Islanders. 22 Upwards of 700 hemoglobin variants, such as sickle cell, have been identified to date. Other known (and less well-known) factors that can falsely raise or lower A1C levels, apart from methodological inaccuracies, include hematologic conditions (e.g., variable red blood cell life span, iron-deficiency anemia, reticulocytosis, and hemolysis), the use of certain medications (vitamin C, erythropoietin, or dapsone), differential rates in hemoglobin glycation, liver disease, splenomegaly of any etiology, untreated hypothyroidism, cardiac valvulopathy, and pregnancy (Table 1). 23,24 In addition to these specific nonglycemic sources of variability in A1C levels, the following general issues must be more widely considered to guard against unreasonable expectations of glycemic control in individual patients or false reassurance leading to inappropriate therapy.
HIV, human immunodeficiency virus.
Variations in the relationship between mean glucose and A1C
Unexplained variations in the relationship between A1C and mean blood glucose are more clinically relevant than generally appreciated. An analysis by the A1c-Derived Average Glucose (ADAG) Study Group in which A1C values were mathematically converted to the same units of measurement as those used for SMBG (integrating continuous glucose monitoring [CGM] and capillary fingerstick measurements) provides an important lesson. Over 2,500 glucose values obtained from 500 subjects, stratified according to baseline A1C, were assessed over a 3-month period via fingerstick blood glucose testing, A1C, and CGM. 25 Excluding circumstances known to interfere with A1C, the 95% predictive interval, or range of corresponding average glucose, increased at each successive A1C level. Thus, as shown in Table 2, a patient with an A1C of 8% (95% confidence interval [CI], 147–217 mg/dL) could have a lower average glucose than another with an A1C of 7% (95% CI, 123–185). These and emerging CGM datasets, while affirming the performance of A1C on a population level, underscore its potential unreliability when comparing individuals. 26
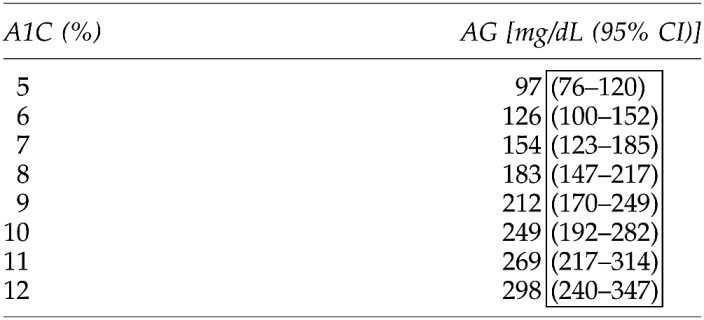
Adapted from Nathan et al. 25
A1C, glycated hemoglobin; AG, average glucose; CI, confidence interval.
Inherited “glycation gaps”
A plausible explanation for consistent within-patient discrepancies between A1C and mean blood glucose is that certain patients have naturally higher or lower A1C relative to expected average mean glucose, owing at least in part to genetic factors that determine the relative rate of intracellular glycation or deglycation. A useful concept for evaluating these so-called high and low glycators is the “glycation gap,” based on comparisons of A1C with glycated serum proteins, such as fructosamine. 27,28 Fructosamine, which reflects an approximate 21-day history of glycemia, provides an empirical reference point for detecting the presence of a glycation gap in situations where SMBG averages and A1C conflict. Using the rough correlations in Table 3, together with a fructosamine test, clinicians and patients can conveniently compare fructosamine with A1C and average blood glucose to help discover which metric is more consistent with mean blood glucose. 29,30 So, for example, a fructosamine level of 399 μmol in a patient with an A1C in the 7.4–7.8% range and a blood glucose meter average of 220–240 mg/dL (typically correlating with an A1C around 10%) would suggest that the patient has a negative glycation gap—that is, the A1C reads lower than the average glucose confirmed by fructosamine. In this case more aggressive antihyperglycemic treatment guided by SMBG values might be warranted. Conversely, an average A1C level higher than indicated on the basis of average blood glucose and fructosamine generally signifies a positive glycation gap. Less clear-cut but common scenarios might include, for example, a patient with an A1C usually near 9%, a fructosamine level of 300 μmol, and a blood glucose meter average of 140–160 mg/dL. In this situation, depending on the individualized glycemic targets, one could reasonably decide not to change diabetes therapy. Finally, when there is complete disagreement among glucose meter readings, fructosamine, and A1C, glucose readings should be the prime driver of antihyperglycemic therapy provided there is enough home testing to guide decision-making. Currently, glycation gap which strongly correlates with determinants of A1C, is not a confirmed independent predictor of complication risk. 31
Adapted from Bartol. 29
A1C, glycated hemoglobin.
Undetected glycemic variability
A1C does not differentiate between patients who reach target average glucose levels with frequent glycemic excursions from those who do so more steadily. Mounting evidence suggests, however, that short-term glycemic peaks and nadirs, known as glycemic variability, not only predict hypoglycemia but may be an independent risk factor for long-term vascular complications. 19,32,33 Regarding the latter, experimental evidence indicates that transient hyperglycemic spikes trigger increases in pro-inflammatory gene expression, which, in turn, cause increased intracellular superoxide production amplifying the original damaging effect of hyperglycemia. 19 In one study of patients with poorly controlled type 2 diabetes, glucose variability strongly correlated with the oxidative-stress biochemical marker 8-iso-prostaglandin F2α. 34 Subsequent analysis of DCCT data did not confirm a relationship between day-to-day variability and microvascular complications in type 1 diabetes but did show that an absolute 1% increase in A1C variability resulted in at least a doubling of retinopathy risk and an 80% increase in nephropathy risk. 35
With respect to hypoglycemia, follow-up analysis of publicly available DCCT quarterly A1C and seven-point capillary glucose profile data showed that mean blood glucose and glycemic variability (within-day standard deviation [SD]), together or separately, signal severe risk independent of A1C. Of the three measures, only end-of-day glucose variability predicted nocturnal hypoglycemia. 32 More recently, an observational study using CGM analysis over a 48-h period in patients with type 2 diabetes showed that the risk of asymptomatic hypoglycemia was virtually eliminated when the SD around the mean glucose value was reduced below a threshold of <1.7 mmol/L (approximately 30 mg/dL). 33 These data associating glycemic variability and hypoglycemia risk are timely because, although glycemic variability was not measured in the aforementioned ACCORD trial, excess mortality risk associated with intensive therapy to achieve near-normal glycemia occurred among subjects whose average A1C remained >7%. It has been speculated that over-aggressive and difficult intensification of treatment in this refractory subgroup could have induced hypoglycemia with attendant deleterious cardiovascular outcomes. 36 More vigilant monitoring of glycemic variability (as a predictor of hypoglycemia) may therefore be warranted in patients with diabetes at high risk for cardiovascular disease. Alternatively, use of non–hypoglycemia-producing agents, such as glucagon-like peptide-1 agonists instead of mealtime insulin, may reduce both variability and hypoglycemia risk. 37
Inability to distinguish fasting from postprandial hyperglycemia
A1C inadequately distinguishes between fasting and postprandial hyperglycemia. However, as shown by Monnier et al. 38 in patients with type 2 diabetes, the relative contributions of each depend on the level of A1C. When A1C is between 6.5% and 8%, for example, larger proportions of the contributing high glucose concentrations (as measured by calculating the incremental area under the daytime plasma glucose curve from 8:00 a.m. to 5:00 p.m.) were observed during the postprandial phase. 38 This finding is compelling given demonstrated causal relationships between postprandial hyperglycemia and markers of cardiovascular diseases (e.g., oxidative stress, carotid atherosclerosis, and endothelial dysfunction). 12,39 –43 In a recent update of its 2007 Guideline for the Management of PostMeal Glucose, the International Diabetes Federation endorsed targeting both postprandial and fasting glucose for achieving optimal glycemic control. 12 SMBG is cited as the most practical method for monitoring postprandial glycemia provided that actionable advice is associated with its use.
Although not yet widely available, an alternative or corroborative measurement that some clinicians find useful is 1,5-anhydroglucitol (1,5-AG [GlycoMark™]), a naturally occurring dietary polyol reflecting transient elevations of glucose over the previous 2 weeks. 44 In patients with moderately controlled glycemia (A1C<8.0%), this emerging assay may be used for detecting postprandial hyperglycemia and/or within-patient trends in glycemic variability, keeping in mind that correlations to acute or long-term complications, if any, are not yet known. As with A1C, caution must be exercised when using 1,5-AG because of individual differences in the renal threshold for glucose, variations across race and gender, and susceptibility to interferences, such as renal failure. 1,5-AG is not affected by red blood cell life span, perturbations of hemoglobin, uric acid, bilirubin, ascorbic acid, creatinine, or maltose.
Taken together, the aforementioned issues underscore limitations of using A1C alone for diabetes management decisions. Although corroborating measures, such as fructosamine or 1,5-AG, can be clarifying when A1C and SMBG data conflict, SMBG remains the mainstay for assessing diabetes control and the risk for short- and long-term complications in individual patients. Furthermore, it must be remembered that all approaches to assessing glycemia are subject to numerous interrelated and sometimes unpredictable factors. These include the analytical performance of blood glucose monitors under changing conditions (or, in the case of CGM, time delays between interstitial fluid and capillary blood glucose measurement), whether or how patients have been taught to take action on results, and the physiological, behavioral, social, and medical setting in which monitoring occurs. 45
Mobilizing the Human Factor
There have been numerous attempts to identify a robust and practical measure of short-term glucose variation. The most noteworthy measures to date for clinical utility are arguably SD, mean amplitude of glycemic excursions (MAGE), Low Blood Glucose Index (LBGI), and coefficient of variation (mean/SD). 26,46 The relative strengths and weaknesses of these methods are presented in Table 4. SD is preferable for the typical patient using SMBG as his or her primary monitoring method because it entails a relatively simple formula based on five to 10 random readings over a 2–4-week period: twice the SD should be less than the average blood glucose (SD×2<average). 47 Downloadable therapy management software programs designed for use with specific blood glucose meters graphically display SDs in different formats at different times of the day. However, this technology, ideally used by patients in collaboration with their healthcare providers, is underutilized largely because optimizing electronic meter memory functions requires knowledge, skill, and volition by both patients and clinicians. 48 Furthermore, downloading data from a wide variety of glucose meters can be cumbersome in the office setting. Expanding built-in data management features that offer immediate feedback to patients through their meters and developing more standardized platforms for data downloading are feasible near-term solutions for overcoming such user–interface hurdles.
Adapted from Weber and Schnell. 46
CGM, continuous glucose monitoring; LBGI, Low Blood Glucose Index; MAGE, mean amplitude of glucose excursions; SMBG, self-monitoring of blood glucose.
Volitional obstacles pose separate but related challenges to the full realization of our glucose-measuring tools. 49 Patients' attitudes toward SMBG self-care behaviors are shaped mainly by whether or not they know what to do and how, their perception of drawbacks versus value at any given time, and their confidence in carrying out the necessary tasks. Clinician ambivalence may stem from concerns about lack of time to address the needs of patients, fear of adverse events (particularly in patients taking insulin), and skepticism about patient commitment to diabetes self-management practices in general. 50 These mutually reinforcing doubts can be “re-set” by using technology to focus conversation and translate the long-term benefits of day-to-day SMBG (e.g., avoiding complications) into concrete short-term rewards (e.g., less hypoglycemia). 48 Furthermore, healthcare providers' willingness to provide information and engage patients in participatory decision-making has been positively associated with patients' ratings of self-confidence and desire to take autonomous action regarding diabetes management, with corresponding improvement in glycemic control. 51 Healthcare policies that support collaborative patient–provider relationships (e.g., in the United States, billing codes for non–face-to-face interactions) should be actively explored, especially at the level of primary care where attitudes toward diabetes are often instilled.
Personalizing Diabetes Monitoring: An Effective Means of Improving Glycemia
Reviewing SMBG readings systematically with patients affords the opportunity to use patients' own data as a teaching tool and focal point for fruitful conversation. 47 In non–insulin-requiring type 2 diabetes—contrary to several studies showing that SMBG can increase stress and anxiety without improving control (at least as reflected by A1C)—periodic glucose profiles obtained at different times of day have been found to help patients see the relevance of SMBG data, create individualized monitoring schedules, and prospectively appreciate that insulin therapy is an inevitable function of progressive disease rather than a sign of personal failure. 52 –54 A staggered regimen of pre- and postmeal blood glucose monitoring can provide instant feedback on the effects of certain foods or medications affecting postprandial hyperglycemia. This information could in turn flag the need for therapy escalation between clinic visits or, conversely, reveal the inefficiency or redundancy of current therapy. Candidates for insulin therapy might further benefit by the application of patient-oriented insulin titration regimens. 16,50 In the multinational AT.LANTUS trial, for example, patients with longstanding type 2 diabetes who initiated basal insulin using patient-driven versus clinician-directed titration protocols achieved significantly improved glycemic control with low incidence of hypoglycemia (<1%). 55
Another noteworthy benefit of strategically timed SMBG is the potential to augment patient safety by uncovering individual variations in blood glucose that might otherwise remain unnoticed. Indeed, a recent U.S. study of nearly 100,000 emergency hospitalizations for adverse drug events in adults ≥65 years of age found that hypoglycemia resulting from antihyperglycemic therapy accounted for nearly a third of emergency department visits, prompting the observation that “current guideline and performance measures may not reflect diabetes management for all patients.” 56 The rapidly growing worldwide prevalence of older people with diabetes—especially those with type 1 diabetes in long-term care facilities who may require more intensive diabetes treatment and be prone to costlier acute metabolic complications than their counterparts with type 2 diabetes—represents another looming crisis warranting more considered approaches to glycemic measurement. 57
Bridging the Education Gap
The paramount role of self-management education in helping patients master techniques of SMBG, check blood glucose at meaningful times, and respond appropriately to results seems self-evident, yet only one-third to one-half of people with diabetes in the United States receive any formal instruction. 58 Barriers to formal diabetes education include lack of referrals by physicians, insufficient reimbursement, a limited number of effective programs, and other logistical and financial factors. 59 A recent evaluation of payer-derived claims for Diabetes Self-Management Training (DSMT) demonstrated that even a single session with a Certified Diabetes Educator yielded benefits with respect to costs, alignment with accepted care guidelines, and outcomes (recognizing that patients who are willing to attend one or multiple sessions may be more likely to achieve these benefits). 60 Although the benefit was found to increase with the number of encounters, only 6% of commercially insured patients attended at least one accredited DSMT program. Of patients enrolled in Medicare, only 3% attended one DSMT program, whereas less than 1% attended multiple sessions. This obvious underutilization presents a formidable obstacle to developing comprehensive individualized care plans.
An alternative practical approach may be found in tapping the potential of diabetes management software to help patients and clinicians gather needed data, discern blood glucose patterns, evaluate influencing factors, and target different metabolic defects. 45 By offering a “big picture” perspective, downloaded meter data, used in conjunction with written logbooks, can readily answer the following questions: Is fasting glucose in range? Are postprandial glucoses in range? Is the patient at risk for hypoglycemia? Is the patient troubleshooting high and low blood glucoses appropriately? Are there any trends occurring over time or on certain occasions? Does mean glucose correlate with A1C? Once out-of-range glucose levels and problematic patterns are identified, comparing downloaded data with manual records of SMBG data can provide useful cues to their root cause, help connect problems to solutions, and enlist patients in making timely adjustments between appointments. The following case shows how SMBG, CGM, and companion diabetes management software systems might be used together to identify problem areas and target treatment accordingly.
Case example
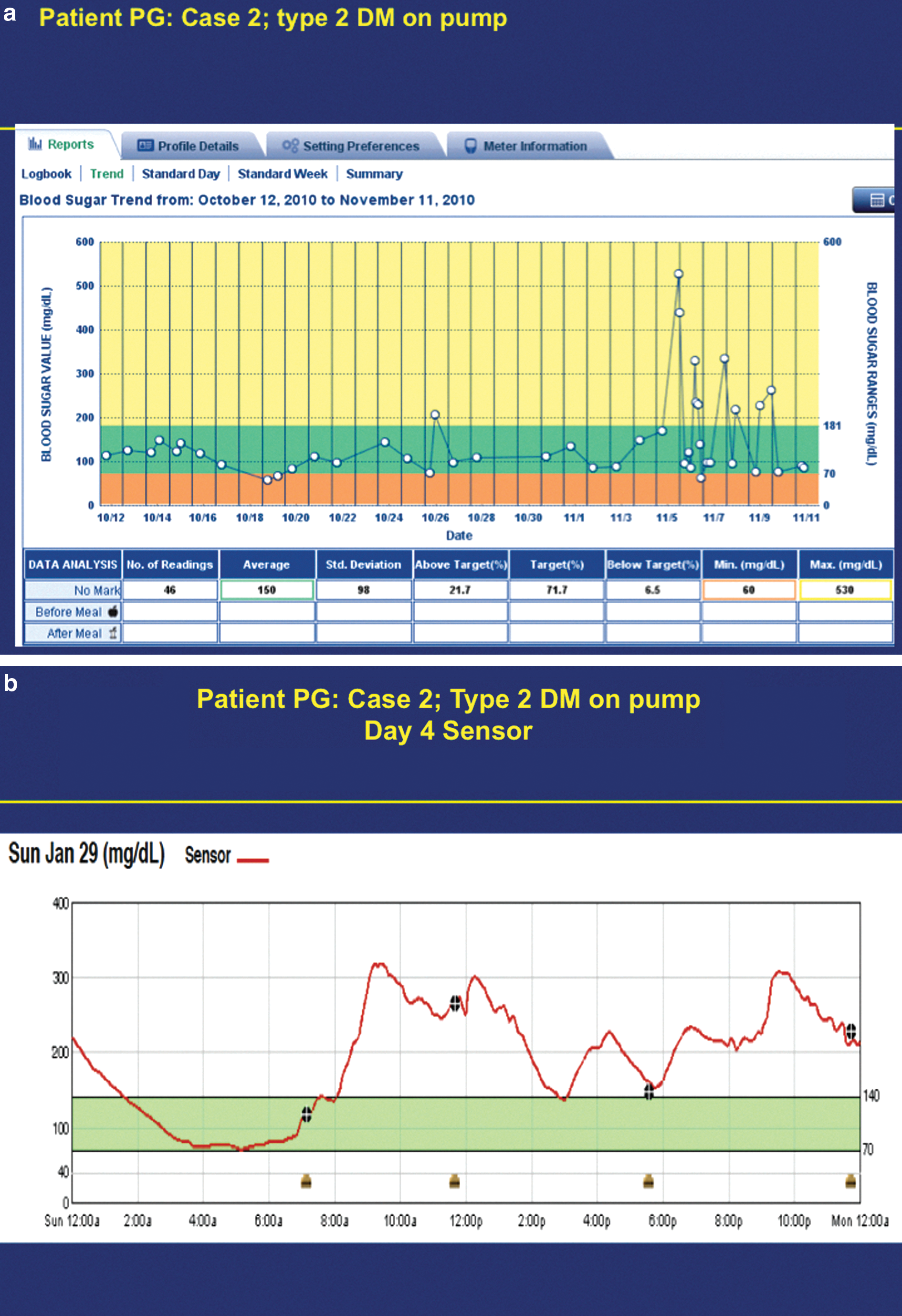
The 64-year-old patient had been diagnosed with type 2 diabetes at 37 years of age. She has been using an insulin pump for over a decade and underwent gastric bypass surgery 6 years ago (current body mass index, 29 kg/m2). Her total daily insulin dose of 20 units/day consists of 69% basal insulin. She tests her blood glucose an average of one to two times per day. Her A1C is 7.9%, and her mean blood glucose over the course of 1 month is 150 mg/dL, with a SD of 98. The high SD is reflected in the Trend Report, which had been downloaded from the patient's blood glucose meter after she expressed concerns about her pump's mechanical function (Fig. 1a). Not finding anything amiss with the pump and noting marked glycemic excursions beginning around midday, the physician followed up with a professional CGM study. (Professional CGM, also known as “masked” or “retrospective” CGM, provides short-term continuous data not seen by the patient in real-time but that can be downloaded at the office visit for retrospective review.) The patient was encouraged to use the meal-marking feature on her blood glucose meter to track pre- and postmeal glucose while wearing the CGM device (which requires four fingerstick tests per day). As shown in Figure 1b, the continuous data revealed that inadequate bolusing in response to certain foods accounted for the patient's high SD. The patient was surprised that, after so many years of diabetes management, she had not simply “felt” that something was wrong. Based on this visual feedback, she agreed to continue monitoring four times per day, including before and after her largest meal, meet with a diabetes educator/pump trainer to better understand her pump's bolus calculator feature, and, until the next visit, follow a simple but flexible algorithm of 4 units of insulin per meal, with increases as needed to keep her next blood glucose reading <120 mg/dL or postmeal <180 mg/dL. The physician wrote this algorithm directly on the patient's logbook at the conclusion of the visit, gave her a written prescription for exercise, which she had asked about, and commended her for considering new approaches to staying healthy.
Summary and Conclusions
On a population basis, A1C remains our most viable and important index of glycemic control and the one with most evidence to show that it predicts diabetes complications. Yet, given that it explained only 11% of the variation in retinopathy risk for the entire DCCT cohort, the question of how critical aspects of glycemia not reflected by A1C should be identified and treated in individuals weighs heavily. The answer will shape expectations for patients, clinicians, healthcare systems, businesses, and governments confronting the monumental public health challenge of diabetes. Selecting wisely from the full array of our current glucose measuring tools, and applying their respective strengths to address the diverse needs of these interdependent stakeholders, holds potential for rapidly optimizing glycemia even as criteria for allocating precious healthcare resources in diabetes evolve.
Footnotes
Acknowledgments
This activity is supported by an unrestricted educational grant from Bayer HealthCare, Diabetes Care.
CME Test Questions