
Abstract
Background:
This study was designed to evaluate two pen needles (PNs) with the same diameter but different lengths (4 mm and 6 mm) and different needle tip shapes (straight and tapered) to compare their effects on glycemic control, perceived pain, safety, patients' ease of use and preferences, and visual impression.
Subjects and Methods:
In this prospective, open-label, controlled crossover study, 41 insulin-treated patients with type 1 or type 2 diabetes were randomized into either Group 1 (the 32-gauge×4-mm PN was used during Study Period 1, then the 32-gauge×6-mm PN was used during Study Period 2) or Group 2 (the order for using the PNs was reversed).
Results:
The 32-gauge×4-mm PN provided an equivalent glycemic control in diabetes patients as the 32-gauge×6-mm PN, with an equivalent occurrence rate of adverse events. The 32-gauge×4-mm PN was perceived as significantly less painful and rated as significantly more favorable than the 32-gauge×6-mm PN according to the survey results on patients' ease of use and preferences and on their visual impressions.
Conclusions:
The 32-gauge×4-mm PN was not only as safe and efficacious as the 32-gauge×6-mm PN, but also was perceived as less painful, easier to use, and more favorable to Japanese adult patients with diabetes.
Introduction
Currently, 5- or 6-mm-long PNs are most commonly used in Japan, and recently we have been able to use 4-mm-long 32-gauge (32G) needles for insulin injection. Then, we conducted this study to evaluate and compare the effects of the newly used 32G×4-mm PN and the existing 32G×6-mm PN on glycemic control, perceived pain, safety, patients' ease of use and preference, and visual impression in Japanese adult diabetes patients.
Subjects and Methods
This research was a prospective, randomized, open-label, controlled home-use crossover study in type 1 or 2 diabetes patients who were 20 years or older, who had been using an insulin pen device for at least 1 year, and who were current users of Novo Fine® 32G tip×6-mm tapered needles (Novo Nordisk Pharma Ltd., Tokyo, Japan) (hereafter referred to as 32G×6 mm). Additional inclusion criteria included insulin injection of two or more times per day, a glycated hemoglobin level in the range of 5.9–8.9% (according to the National Glycohemoglobin Standardization Program), and a body mass index of less than 35 kg/m2. Exclusion criteria were any physical conditions that may hinder adherence to study procedures, any neurological diseases, nephrotic syndrome, pregnancy, or lactation.
Each subject visited our institute three times during the study. At Visit 1, all the screened subjects received a verbal explanation of the study procedures, and written informed consent was obtained. Subjects were then randomized into either Group 1 or Group 2. Subjects in Group 1 were instructed to use the 32G×4-mm needle (Micro-Fine® Plus 32G×4-mm thin wall; Nippon Becton Dickinson Company, Ltd., Tokyo) during the first month of the study period (Study Period 1) and then to use the 32G×6-mm needle during the second month (Study Period 2). Subjects in Group 2 were asked to use the 32G×6-mm needle in Study Period 1 and then the 32G×4-mm needle in Study Period 2. Each subject was instructed to use only one type of the allocated PN during each study period and to fill in the given document (Injection Events) for each injection, including adverse events such as bending or breakage of needles.
At Visit 2, after Study Period 1, the study coordinator checked the completeness of the documents written by the subjects and clarified any ambiguity. Finally, at Visit 3, after Study Period 2, the study coordinator checked the documents written by the subjects and clarified any ambiguity. Thereafter, the subjects were asked to complete a questionnaire on their visual impression or preferences for these PNs.
Assessments
The primary end point was to determine any differences in glycated albumin (GA) levels at the ends of the two study periods. Serum GA reflects the average blood glucose concentration during the past 1–2 weeks. 14 The clinical significance of GA is similar to that of glycated hemoglobin, but GA is regarded as a better indicator for glycemic excursion in diabetes patients. 15 The secondary end points were adverse events during injection in the two study periods, perceived pain, subject's preference, and visual impression. Adverse events during injection were recorded by the subjects. Perceived pain, subject's preference, and visual impression were assessed using questionnaires for the subjects (Table 1).
Needle A was a 32-gauge×4-mm needle, and Needle B was a 32-gauge×6-mm needle.
VAS, visual analog scale.
Assessment of perceived pain
Comparative perceived pain in the use of the two types of PNs was assessed using a validated 150-mm visual analog scale (VAS). 16,17 Two weeks after the start of Study Period 2, each subject marked the VAS with a vertical dash by comparing the difference in the degree of pain that they perceived during their use of these two types of PNs. We calculated the degrees of perceived pain when using the two PNs by measuring the gap in the VAS. A calculated value of 0 means no difference in pain. Positive values indicate that the PN used in Study Period 2 was more painful, and negative values mean that it was less painful.
Subjects' ease of use and preference
Along with the pain assessment, 2 weeks after the start of Study Period 2, each subject was asked to complete a questionnaire for rating the two PNs with regard to the ease of use and subject's preference. The questionnaire was designed by the investigators in reference to the previous studies of Hirsch et al. 9 and Iwanaga and Kamoi, 18 and the subjects answered each question on a scale of 1–5.
Visual impression
At Visit 3, subjects were shown two unshielded and unlabeled PNs identified as “Needle A” and “Needle B.” Needle A was a 32G×4-mm needle, and Needle B was a 32G×6-mm needle. After examining the two PNs, the subjects completed the questionnaires that compare visual impression, which may affect the psychology of patients who require a routine subcutaneous injection.
Statistical analysis
The sample size was based on a two-tailed t test with a significance level of 0.05 and a power level of 0.90. With the anticipated effect size the average difference in the mean GA level is within 20%, with the 95% confidence interval (CI), so that the level of glycemic control with the two devices can be considered equivalent. The required sample size was 20 in each group, 40 in total. Analysis of variance was performed to determine if the needle type or the order of needle usage was associated with the GA level.
For the secondary end point, the frequency of adverse events during injection was calculated per needle type using Fisher's exact test. The mean pain VAS scores were analyzed using one-sample t test with the threshold of median 0, at an α=0.05 significance level. The ease of use, subject's preference, and visual impressions were analyzed using Wilcoxon's signed-rank test. A value of P<0.05 was considered to indicate a statistically significant difference.
Results
Among the 41 subjects who were randomized into the two study groups (Fig. 1), three were excluded from the end-point analyses because of protocol deviations (two from Group 1 and one from Group 2). The mean body mass index of all the randomized subjects was 23.2 kg/m2, 36 (88%) had type 2 diabetes, 28 (68%) were male, and the mean age was 64 years old (Table 2).

Study flow diagram. 32G, 32-gauge.
BMI, body mass index.
The mean absolute change in the GA levels at the ends of Study Periods 1 and 2 was 5.63% (95% CI, 3.67–7.59%) (n=38, P<0.0001) (Fig. 2). Because this is well within the acceptance criteria of ≤20%, the abilities of the two PNs to control glycemic levels are considered equivalent. The frequencies of injection events are listed in Table 3. The 32G×4-mm needle had a trend toward more leakage and bleeding than the 32G×6-mm needle, although the difference was not significant. The average VAS score for comparative pain was −16.6 mm (−26.0 mm, −7.3 mm) (P=0.0009), indicating that the 32G×4-mm needle was rated as less painful than the 32G×6-mm needle. The survey results on the subjects' ease of use and preferences for the PNs are shown in Figure 3. None of them gave an “Absolutely” rating for the 32G×6-mm needle. Except for the similar ratings for needle stability in the skin, the subjects significantly preferred the 32G×4-mm needle in all the other question categories. The survey results on the subjects' visual impression for the two unlabeled PNs (32G×4 mm and 32G×6 mm) are shown in Figure 4. The 32G×4-mm needle was selected significantly more frequently for all the question categories.

Variation in glycated albumin levels during the study periods. The needle type and the order of needle usage were not significantly associated with the glycated albumin level (P=0.8096). 32G, 32-gauge; CI, confidence interval.
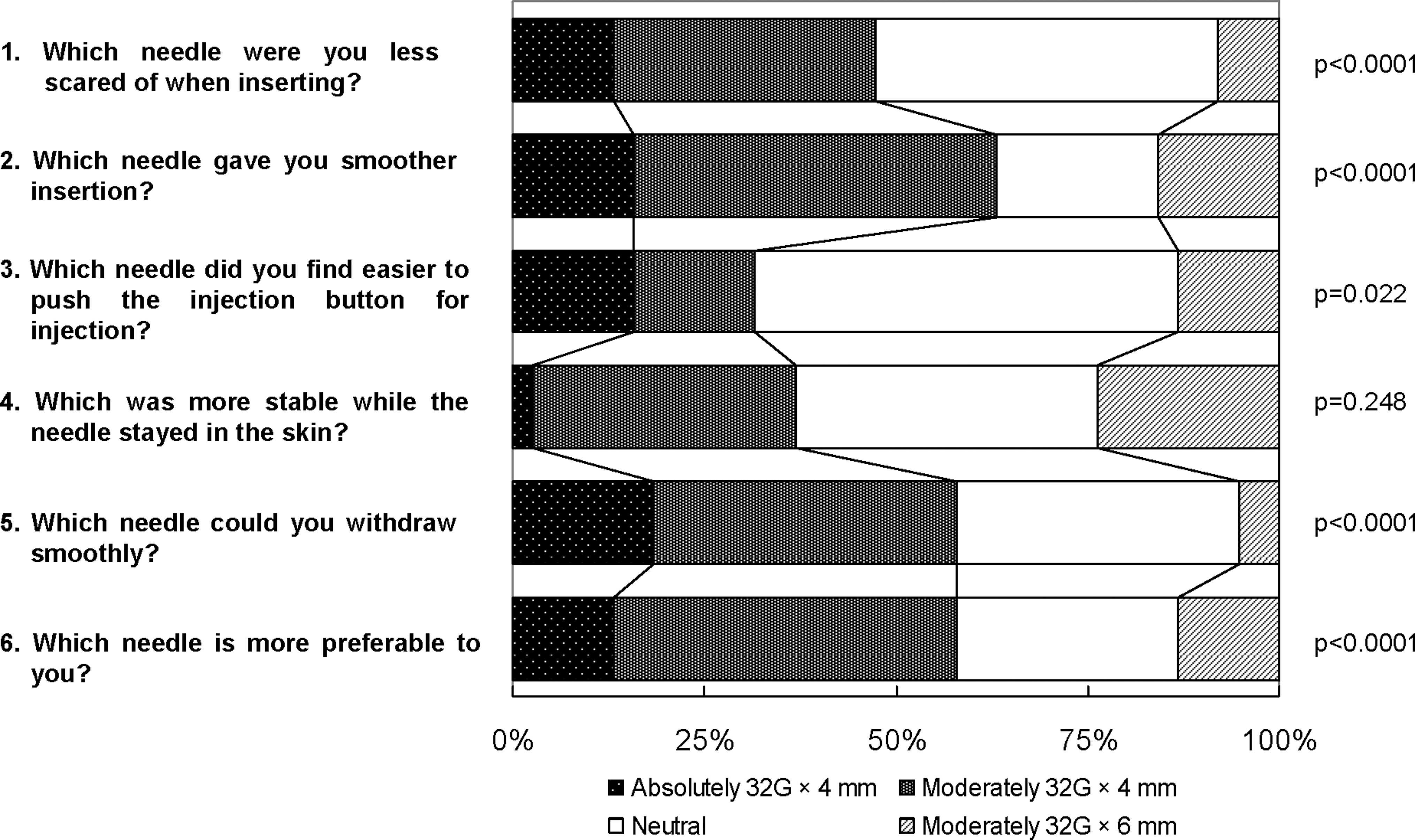
Results from the subject preference questionnaire. The percentages of subjects who chose between the two pen needles (32-gauge [32G]×4-mm or 32G×6-mm) by grading them as “absolutely” or “moderately” or choosing “neutral” when they could not find a difference are indicated.

Visual impressions of unlabeled pen needles. The subjects were asked to complete a questionnaire on visual impression for the two unlabeled pen needles. The 32-gauge (32G)×4-mm needle was selected significantly more frequently for all the question categories. This indicates that the 32G×4-mm needle appeared to be less painful, less scary to inject, and more likely to make the subjects without experience in insulin therapy using pen needles feel more confident and at ease in starting therapy.
Adverse events
There were no unexpected or serious adverse events during the trials.
Discussion
In the present prospective and controlled crossover comparison study, we have demonstrated that the 32G×4-mm PN provided a level of glycemic control and a occurrence rate of adverse events equivalent to those of the existing 32G×6-mm PN. Furthermore, a significantly high number of patients rated the 32G×4-mm PN as less painful according to VAS, less scary to use, and easier to insert, and they preferred this type of PN over the 32G×6-mm PN on the whole.
A common medical belief regarding injection therapy is that obese patients “need” longer needles to administer insulin effectively. However, several studies from 1999 have shown opposite results. Each of these studies compared successively shorter and thinner PNs with previously used larger types and demonstrated an equivalent level of glycemic control, less pain, and nearly always greater preference for the shorter PNs by the patients. These previous studies have compared 31-gauge×8-mm with 29-gauge×12.7-mm PNs, 13 31-gauge×6-mm with 29-gauge×12.7-mm PNs in obese patients, 8 and 31-gauge×5-mm with 31-gauge×8-mm PNs in obese patients. 12
Hirsch et al. 9 reported that three types of needles differing in diameter and length (31-gauge×5 mm, 31-gauge×8 mm, and 32G×4 mm) provided equivalent levels of glycemic control, but the shortest needle (32G×4 mm) achieved reduced pain and greater preference than the two other needles. However, it was uncertain whether we could apply their results to Japanese patients, considering the differences in their study population in which the mean body mass index was 31 kg/m2.
Our results indicated improvement in the quality of life of the patients with the use of the shorter needle, which maintains an equivalent level of glycemic control as the longer needle in Japanese diabetes patients whose obesity level is lower than that of Europeans and Americans. To this end, our findings have important implications that the use of a shorter needle, independently of the presence of obesity, maintains the blood glucose control at an equal level as a long needle and improves patients' quality of life.
Before the conduct of this study, we were aware of the possibility that the frequency of adverse events such as bending of needle and leakage of insulin may increase when using a shorter needle. However, reports of bent needles were infrequent, and insulin leakage was also rare in our study. Wittmann et al. 19 reported that the needle length did not have a marked effect on the amount of insulin leakage. Their conclusions were based on an experimental model using pork rinds, and our results support their findings in humans. Hirsch et al. 9 also reported that there was no significant difference in the leakage occurrence rate among three needle types (31-gauge×5 mm, 31-gauge×8 mm, and 32G×4 mm). Although there was no significant difference in adverse events in this study, considering the sample size, we hope that this will stimulate further studies.
In addition, it is expected that the use of a shorter needle in lean subjects would reduce the risk of intramuscular injections, which increase the variation in the insulin absorption rate. Birkebaek et al. 20 designed a small study to compare the use of a 4-mm needle with a 6-mm needle in lean patients with diabetes, including children, and demonstrated that the use of the 4-mm needle achieved a significant reduction in the risk of intramuscular injections without increasing backflow from the skin.
Iwanaga and Kamoi 18 previously reported what kinds of needle design contribute to perceived pain of insulin injection in which they compared 32G×6-mm (with taper) and 31-gauge×5-mm (without taper) needles. They reported that needle diameter and shape more strongly influenced the reduction of injection pain and needle anxiety than needle length. They also indicated that the difference in needle shapes (mainly the presence or absence of the taper) is a critical factor for diabetic patients in administering self-injection of insulin. However, in our study, the needles had the same diameter, but differed in terms of the presence of the taper and the length of the needle. As a significantly larger number of patients preferred the 32G×4-mm PN (no taper), we considered that it is not the presence of the taper but the length of the needle that was the contributing factor for reducing the injection pain and needle anxiety of self-injection in diabetes patients.
Conclusions
The new 32G×4-mm needle provides an equivalent level of safety and efficacy as the conventional 32G×6-mm needle and is not likely to cause any specific disadvantages during clinical use. More important is that this study showed that the 32G×4-mm needle may provide more benefits to insulin-dependent diabetes patients who need insulin therapy and improve their quality of life as they are more likely to perceive the 32G×4-mm needle as less painful and easier to use. The 32G×4-mm needle may be useful for patients starting insulin therapy because of its more favorable visual impression.
Limitations
The limitations of this study include the lack of a widely validated quality of life measure and the small sample size. Our future studies will include a larger number of samples and will involve the use of a widely validated quality of life evaluation method to address these limitations.
Footnotes
Acknowledgments
We are indebted to Dr. Atsuko Kimura, Ph.D., and Associate Professor Edward F. Barroga, Ph.D., of the Department of International Medical Communications at Tokyo Medical University for their editorial review of the English manuscript. We are also indebted to Dr. J. Kuri, S. Tozaka, and H. Tateno (Nippon Becton Dickinson Company Ltd.) and Dr. L. Hirsch (Becton Dickinson Company) whose suggestions made enormous contribution to our work. The materials used in this study were provided by Nippon Becton Dickinson Company Ltd.
Author Disclosure Statement
No competing conflicts of interest exist.