
Abstract
Background:
Acute lymphoblastic leukemia (ALL) maintenance therapy (MT) has been occasionally associated with symptomatic hypoglycemia (SH), attributed to purine analog (mercaptopurine [6-MP]). This hypoglycemia has been hypothesized to affect substrate utilization of gluconeogenic precursor alanine in the liver.
Case Report:
An overweight 5-year-old boy with ALL was evaluated for SH (lethargy and vomiting) that occurred 8–10 h after fasting while receiving daily 6-MP. Hypoglycemic episodes (>20 episodes per month) occurred predominantly around midmorning but not during the 5-day dexamethasone pulse. The adrenocorticotropic hormone test yielded a normal cortisol response, which ruled out pituitary adrenal suppression. A 12-h overnight fasting glucose was 49 mg/dL, with suppressed insulin response <2 IU/mL, low C-peptide of 0.5 ng/mL, high insulin-like growth factor-binding protein >160 ng/mL, high free fatty acid of 2.64 mmol/L, and negative glucagon stimulation test (change in blood glucose [BG] <5 mg/dL). These results ruled out hyperinsulinism. The patient was placed on cornstarch therapy 5 h prior to dosing with 6-MP. This treatment reduced the SH events to fewer than two episodes per month. To study the efficacy of cornstarch, the patient was fitted with the iPro™ professional continuous glucose monitoring system (CGMS) (Medtronic MiniMed, Northridge, CA) with a preset low alarm at 70 mg/dL, which was worn for a period of 5 days while the patient was on cornstarch. With 1,000 sensor reading the BG range was 65–158 mg/dL, and the percentage mean absolute difference between sensor and finger-stick BG readings (the parent monitored his BG four times a day) was 9.4%. There were no hypoglycemic episodes detected by the CGMS while the patient was on cornstarch. After the cessation of chemotherapy, a 15-h fasting study was performed, and the CGMS was placed. Results showed resolution of hypoglycemia.
Conclusions:
The CGMS helped us devise an effective management plan for our patient. CGMS proved useful as an adjunct to characterize the pattern of hypoglycemia and to validate the benefit of cornstarch in hypoglycemia associated with 6-MP treatment of ALL.
Background
The backbone of maintenance chemotherapy for childhood ALL is oral daily 6-mercaptopurine (6-MP) and weekly metrotrexate. Ziino et al. 3 found an incidence of 7% of hypoglycemia in children with ALL who were receiving purine analog. This hypoglycemia may be an underreported adverse effect of ALL maintenance chemotherapy. 3 –6 The mechanism of purine analog (MP)-induced hypoglycemia remains unclear. Halonen et al. 4,7 did fasting studies on children with ALL and found that plasma levels of the gluconeogenic amino acids alanine and glutamine were significantly lower in children who developed hypoglycemia. 7 In this subgroup of children, liver enzymes were elevated, suggesting that the tendency toward hypoglycemia was associated with concomitant liver dysfunction. 4 It is known that purine analogs cause liver toxicity by inhibiting de novo purine synthesis. 6 Therefore, it is hypothesized that impaired hepatic gluconeogenesis associated with liver dysfunction is causing hypoglycemia. 7 The continuous glucose monitoring system (CGMS) is an innovative technological tool that could be used to monitor hypoglycemia in ALL patients.
Childhood hypoglycemia is generally defined as a blood glucose (BG) level lower than 60 mg/dL (3.3 mmol/L), during which there are symptoms due to compensatory sympathetic stimulation and symptoms of neuroglycopenia. 8 Hypoglycemia causes cognitive impairment in children, 9,10 and it is important to recognize that hypoglycemia of any cause can impact memory and attention skills.
CGMS devices are medical devices that measure interstitial fluid glucose utilizing a subcutaneous glucose sensor probe. A CGMS can be worn for several days and provide measurements of glucose every 5 min (up to 288 measurements per day). 11 In 2007, the Food and Drug Administration approved a pediatric model of a CGMS for use with an insulin pump or as a stand-alone device for the management of diabetes in children 7–17 years old. Studies have reported the accuracy of the CGMS with a large number of paired data points. 12 The CGMS is safe and well tolerated and provides readings that are in close agreement with glucose meter values, 13 although there is a time lag of about 20 min. In 2011, The Endocrine Society formulated practice guidelines for the use of CGMS. The Society makes no recommendation for or against the use of CGMS by children with type 1 diabetes mellitus who are younger than 8 years of age and by children without diabetes (as a device to monitor glucose levels in hypoglycemic evaluations) as the data are limited. 14 There have been nonrandomized studies indicating that CGMS can be used successfully in patients less than 8 years of age. 13,15
We report a case of hypoglycemia in a child with ALL, in remission, being treated with 6-MP. Significant symptomatic hypoglycemia was managed with oral cornstarch. The CGMS was used off-label to study the BG profile during cornstarch therapy. The device helped verify the resolution of hypoglycemia after the discontinuation of the therapy.
Case Report
Our patient is a 5-year-old overweight boy (weight, 76th percentile; height, 23rd percentile; body mass index, 95th percentile) with ALL diagnosed at the age of 2 years. He was treated with maintenance chemotherapy including oral administration of dexamethasone (3 mg/m2 per dose twice a day for 5 days every 4 weeks), 6-MP (75 mg/m2 per dose per day), and weekly methotrexate (20 mg/m2 per dose per week), as per the Children's Oncology Group COG AALL0331 protocol. The patient was tested for the thiopurine S-methyltransferase (TPMT) genotype in order to identify whether he is at risk for toxicity from thiopurine medication, including 6-MP. The result was negative for poor metabolizer alleles (genotype TPMP*1/TPMT*1). Two months after starting his first maintenance phase (Day 62), the child was found to be unresponsive, and his glucose level was recorded as 22 mg/dL. The child experienced diaphoresis, nausea, and vomiting (more than 20 episodes per month), for which there was no obvious identifiable cause. He had multiple repeated episodes of hypoglycemia (range, 43–59 mg/dL) detected by home glucose monitoring, which usually occurred 9–13 h after an overnight fast. The child had not experienced any identifiable episodes of hypoglycemia during the preceding months as he underwent the consolidation and delayed intensification phases of chemotherapy, although hypoglycemia has been reported even in these phases by other investigators. 3
The child was admitted to the Intensive Care Unit during the second maintenance phase for an overnight formal fasting protocol. After he had fasted for 12 h, his glucose level decreased to 49 mg/dL, critical labs (results are shown in Table 1) were collected, and 1 mg of glucagon was administered subcutaneously. The change (rise) in glucose level 30 min after glucagon was given was less than 5 mg/dL. Hyperinsulinemia was excluded because of the negative glucagon stimulation test, low insulin level, low C-peptide, and presence of high free fatty acid. Urine organic acid testing showed an elevated 3-hydroxybutyric acid level, which indicated ketosis. The adrenocorticotropic hormone (250 μg) stimulation test was performed on a separate day, and the cortisol level rose to 25.9 μg/dL at 60 min after test, ruling out adrenal insufficiency (Table 1). The liver function test showed a more than two times elevation of liver enzymes (Table 1). The working diagnosis was ketotic hypoglycemia secondary to 6-MP.
IGF, insulin-like growth factor; IGFBP, insulin-like growth factor binding protein; NA, not available; QNS, quantity not sufficient.
Therefore 6-MP dose timing was switched to 5 a.m. in the morning instead of the evening in order to prevent the hypoglycemia that usually occurred between 9 and 11 a.m. The patient was placed on 2 tablespoons (15 g of carbohydrate) of cornstarch in soy infant formula (Enfamil® Prosobee; Mead Johnson Nutritionals, Evansville, IN) 5 h prior to each dose of 6-MP 1 week after the fasting study was conducted.
This management reduced the symptomatic hypoglycemia events to fewer than two episodes per month. To further study the efficacy of cornstarch, the iPro™ Professional CGMS (Medtronic MiniMed, Northridge, CA) was used for a period of 5 days while the patient was on cornstarch. The CGMS record was preset with a low alarm at 70 mg/dL. With 1,000 sensor readings the BG level ranged from 65 to 158 mg/dL with a percentage mean absolute difference between sensor and finger-stick BG readings of 9.4%. There were no hypoglycemic episodes detected in the CGMS while the patient was on cornstarch as shown in Figure 1.
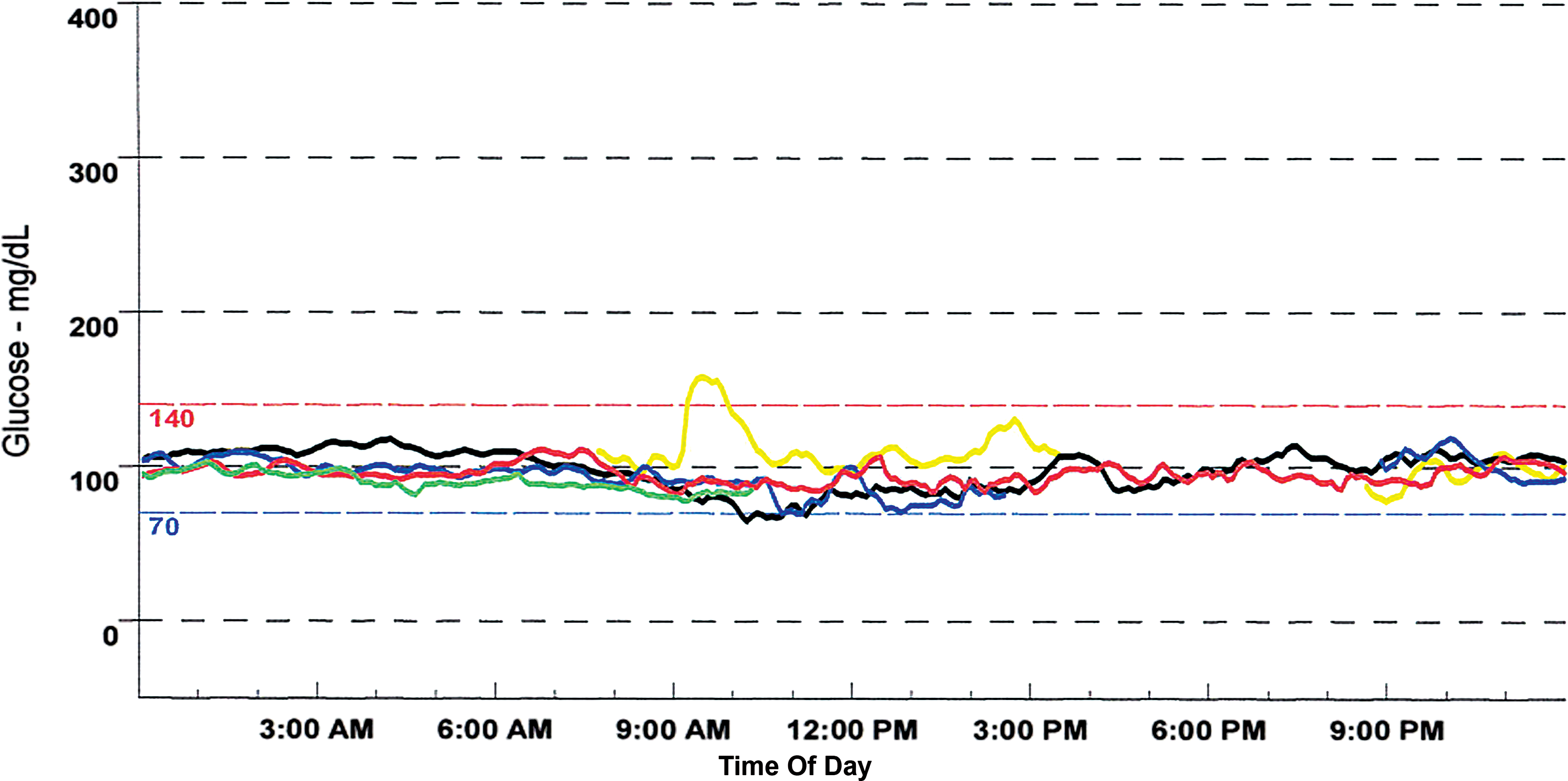
Continuous glucose monitoring system readings during five consecutive days. To convert blood glucose units from conventional units (in mg/dL) to SI units (mmol/L), multiply by 0.0555. Color images available online at
Three months after the cessation of chemotherapy, a 15-h fasting study was conducted. The CGMS was placed 4 days prior to and during the fasting study. The patient had a glucose level of 79 mg/dL at the end of the fasting study. After these results were obtained, self-monitoring of BG (SMBG) was discontinued.
Discussion
Our patient had symptomatic hypoglycemia associated with 6-MP maintenance therapy for ALL, similar to that found by other investigators. 3 –6 Our investigation adds to the knowledge that hypoglycemia secondary to ALL maintenance chemotherapy is more likely to occur in children who have liver dysfunction. 4 TPMT activity exhibits genetic polymorphism and plays an important role in the metabolism of thiopurine medication, including 6-MP. 16 Patients who inherit low levels of TPMT activity are at high risk for developing serious side effects in response to thiopurine medication. 5,16 However, our patient had normal TPMT based on a genetic study; thus we do not believe TPMT deficiency played a role in his hypoglycemia.
One of the treatment options for hypoglycemia is use of complex carbohydrates. We successfully used cornstarch at midnight to offset the fasting hypoglycemia. We used cornstarch because it has been used effectively in the management of hypoglycemia in type I glycogen storage disease. 17 In our patient, cornstarch therapy eliminated long-standing intermittent hypoglycemia. Additionally, the change in the timing of the 6-MP dose also may have helped to prevent the hypoglycemia. The hypoglycemia resolved when maintenance chemotherapy was completed, as shown by our patient's response to a 15-hour fast.
The CGMS proved useful as an adjunct to capillary BG monitoring to characterize of the timing of hypoglycemia. CGMS has an advantage over intermittent SMBG in that it has potential to detect hypoglycemic events that may occur between the time points of SMBG, especially for nocturnal hypoglycemia. 14 Neither CGMS nor SMBG perfectly reflects plasma glucose levels, but they are clinically useful correlates. The CGMS shows the glucose concentration in the subcutaneous interstitial fluid, which has been shown to reflect the concentrations and dynamics of glucose in the brain. 18 Treatment of hypoglycemia is important as we know that untreated protracted hypoglycemia can have deleterious neurocognitive effects. CGMS technology helped us devise an effective management plan for and helped validate the benefit of cornstarch therapy for our patient. We demonstrated the utility of CGMS in documenting the effectiveness of cornstarch to prevent 6-MP-induced hypoglycemia. Therefore, we suggest that CGMS can be used as a tool to study the pattern of hypoglycemia and to also guide treatment of hypoglycemia.
We would like to highlight several points from our case. Hundreds of children undergo chemotherapy with 6-MP every year, yet little is known about the prevalence of 6-MP-induced hypoglycemia. When hypoglycemia is discovered (by either history or biochemical testing) during treatment, a rigorous fasting protocol should be undertaken to better delineate the etiology of the hypoglycemia. Cornstarch proved useful in treating 6-MP-associated hypoglycemia, and this may be considered a treatment option. The iPro CGMS holds promise as a tool to elucidate glucose fluxes in challenging cases of hypoglycemia to help identify the pattern of hypoglycemia.
Footnotes
Acknowledgments
The authors acknowledge Medtronic USA, who provided the iPro Professional Continuous Glucose Monitor for the evaluation of our patient in this study.
Author Disclosure Statement
No competing financial interests exist.