
Abstract
Background:
Effects of lifestyle change on blood glucose levels can be monitored by self-monitoring of blood glucose (SMBG) in type 2 diabetes mellitus (T2DM) patients. We analyzed whether the SMBG-structured lifestyle intervention program ROSSO-in-praxi-international can improve glucometabolic control in the short and the long term.
Subjects and Methods:
One hundred twenty-four SMBG-naive ambulatory non–insulin-treated T2DM patients were randomly assigned to an SMBG group (n=63) and a control group (n=61). Both groups received a 12-week structured lifestyle guidance manual. The SMBG group additionally got a blood glucose meter with 150 test strips and was instructed to measure blood glucose regularly as well as event-driven. Glucometabolic parameters were assessed at baseline, after 12 weeks, and after 1.5 years.
Results:
During the 12 weeks of intervention the SMBG group significantly improved glycated hemoglobin (HbA1c) levels (from 7.4±1.6% to 6.9±1.1% [P<0.001]) and weight (−0.9±1.9 kg [P<0.05]), whereas HbA1c reduction (from 7.5±1.0% to 7.3±1.0%) and weight loss (−0.6±2.4 kg) were not significant in the control group. Of the 124 patients, 122 completed the 1.5-year follow-up. In the control group HbA1c increased again, reaching baseline values (7.5±0.7%). In the SMBG group HbA1c remained stable (6.9±0.9% [P=0.0003 for trend]), and weight (−1.6±3.0 kg vs. baseline [P=0.0003 for trend]) improved further. Eighty-seven percent of participants in the SMBG group continued to perform SMBG. Those who measured their blood glucose more than three times per week (n=24) demonstrated an overall reduction in HbA1c of 1.0% (P=0.006 vs. three times or fewer per week) after 1.5 years.
Conclusions:
Integration of SMBG into basic therapy of T2DM for monitoring the effect of lifestyle changes improves glucometabolic control and has long-term effects.
Introduction
Recently, we developed a short-term, highly motivational, but low-cost program—the SMBG-structured 12-week lifestyle guidance ROSSO-in-praxi 7 —and could demonstrate a significant reduction in HbA1c and other cardiometabolic risk factors, even long term, combined with a significant improvement in the quality of life. 8 (The studies ROSSO-in-praxi 7,8 and ROSSO-in-praxi international have been developed on the basis of the findings from the ROSSO trial [Retrolective Study Self-Monitoring of Blood Glucose and Outcome in Patients with Type 2 Diabetes], 9 which demonstrated that fatal and nonfatal cardiometabolic events were lower in T2DM patients who performed SMBG. Both studies investigate the effects of SMBG in a prospective setting: ROSSO-in-praxi 7,8 is an uncontrolled proof-of-principle study with non–insulin-treated T2DM patients from Germany, and ROSSO-in-praxi international is a randomized controlled trial with non–insulin-treated T2DM patients from Bulgaria.) As in this pilot program a control group was lacking, the aim of ROSSO-in-praxi-international was to apply the manual-based lifestyle guidance on SMBG-naive, non–insulin-treated patients with T2DM in a randomized controlled trial and to analyze the effects of SMBG on HbA1c and other cardiometabolic factors in the long term.
Subjects and Methods
Study population
The study was designed as a prospective, randomized, parallel-group comparison between non–insulin-treated T2DM patients included in manual-based lifestyle guidance with an SMBG group and a control group. The study duration was 12 weeks. Subjects were recruited from the inpatient and outpatient database in a Bulgarian clinic. Patients who had been diagnosed with T2DM by the treating physician within the last 5 years, were ≤75 years old, with a body mass index (BMI) of ≥27 kg/m2, had not been treated with insulin or oral antidiabetes medication (with the exception of metformin), and had no experience with SMBG were eligible for the study. The participants were randomly assigned to an SMBG group or a control group. The first subject was enrolled on December 4, 2008; the last subject completed the 12 weeks of intervention on May 28, 2009, and the follow-up on September 8, 2010.
One hundred twenty-four SMBG-naive, ambulatory, non–insulin-treated T2DM patients were randomly assigned to an SMBG group (n=63) and a control group (n=61). Participants visited the study center at baseline, after 12 weeks, and for a follow-up after a mean of 1.5 years. Two patients were lost to follow-up and did not attend the clinic after 1.5 years. Thus 122 participants (98%) completed both the 12-week lifestyle guidance and the 1.5-year follow-up. The study was approved by the local ethics committee and performed according to the rules of the Declaration of Helsinki. All participants gave their informed written consent.
SMBG-structured 12-week lifestyle guidance
At the baseline visit the participants in the SMBG group received a blood glucose meter, 150 test strips (Accu-Chek® Performa; Roche Diagnostics, Mannheim, Germany), needle pricks, and a short manual. They got detailed information about self-monitoring, and they were educated and trained by the study nurse how to use the glucose meter and how to perform SMBG. The manual included templates to record the blood glucose values. Participants were advised to perform four seven-point blood glucose diurnal profiles at baseline and after 4, 8, and 12 weeks, as well as event-driven SMBG (e.g., 1.5–2 h after chocolate consumption or at fasting state in the morning, when exercise had been done the evening before). The patients were motivated to draw their own conclusion from the SMBG results after such lifestyle events and to modify their daily habits. The manual offered motivation to change lifestyle, guidance, how to change eating habits, how to react on hyperglycemia with physical activity, and how to prevent hypoglycemia. On the basis of their blood glucose values patients should understand the interference of their eating and physical activity behavior on the resulting blood glucose values, and this should result in the sequence SMBG, eating, SMBG, acting. Profiles had not been reviewed during the trial but were transferred to the attending physician at visit 2 after 12 weeks. Recommendations on metformin dose were made on the basis of the trend of all blood glucose profiles. Three reminder calls from the treating physician (each a few days before the day that the profile should be measured) were included to maintain participants' motivation and adherence to the study. The participants were instructed not to change their antidiabetes medication themselves but only after advice from their treating physician. Participants in the control group had no access to SMBG but got a similar manual including basic information about calorie-restricted diet, physical activity, and weight loss, although instructions on SMBG and templates for blood glucose diurnal profiles were not included. The study physician took care of the patients during the 12-week period; thereafter patients were transferred to general practitioners for usual care. The participants from both groups were invited to attend the clinic 1.5 years after the study's end.
Determination of glucometabolic parameters
At baseline, at the end of the study (12 weeks), and at 1.5 years after the study's end, actual body weight, waist circumference, and blood pressure were measured, and blood was drawn in both groups by a diabetes nurse or the treating physician. HbA1c, as the main outcome parameter, was measured by an immunoturbidimetric method; levels of triglycerides, total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol were determined by enzymatic colorimetric methods (Cobas Integra 400; Roche Diagnostics GmbH).
Statistical analysis
The Friedman test plus Dunn's multiple comparison test was used to compare values at “baseline,” “end of study,” and “follow-up” within both groups. The Mann–Whitney test was used for between-group comparisons, and within-group differences were analyzed using the Wilcoxon signed rank test. Spearman's correlation was used for determination of associations and logistic regression analysis for identification of parameters that contributed to the observed HbA1c reduction. Level of significance was 0.05. For data analysis GraphPad Prism version 4.0 (GraphPad Software, San Diego, CA) and SAS statistical package version 9.1 TS2MO (SAS Institute, Cary, NC) were used.
Results
Addition of SMBG to a 12-week lifestyle guidance significantly improved glucometabolic control and cardiovascular risk factors
One hundred twenty-four T2DM patients were included in the study. One hundred twenty-two participants (98%) completed both the 12-week lifestyle guidance and the 1.5-year follow-up. The groups are comparable, although participants in the SMBG group (n=63) had a shorter duration of T2DM than those in the control group (n=61) (Table 1). The primary end point of the analysis was reduction of HbA1c. During the 12 weeks of lifestyle guidance patients in the SMBG group in comparison with the control group were able to significantly reduce their HbA1c level from 7.4±1.6% to 6.9±1.1% (−0.5±0.9% [P<0.001] vs. −0.2±0.6% [P=0.38] in the control group), body weight from 90.2±17.8 to 89.2±17.6 kg (−0.9±1.9 kg [P<0.05] vs. −0.6±2.4 kg [P=0.38]), BMI from 30.8±4.7 to 30.5±4.7 kg/m2 (−0.3±0.7 kg/m2 [P<0.05] vs.−0.2±0.8 kg/m2 [P=0.36]), and waist circumference from 105±12 to 104±12 cm (−1.0±2.8 cm [P<0.05] vs. −0.6±2.9 cm [P=0.34]). Blood pressure, triglycerides, and total and high-density lipoprotein cholesterol improved in addition, although no statistical significance was reached. During the 12 weeks of study no statistically significant improvements were observed in the control group. No adverse or side effects were reported during the study.
Data are mean±SD values.
The Mann–Whitney test was used for comparison of baseline values between the self-monitoring of blood glucose (SMBG) and the control group: a P<0.01.
The Friedman test plus Dunn's multiple comparison test was used to compare values at baseline, end of study, and follow-up within both groups: b P<0.05, c P<0.001.
BMI, body mass index; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Improvements in HbA1c, weight, BMI, and waist circumference could be maintained during 1.5 years of follow-up
Patients were followed up for a mean of 1.5 years. One hundred twenty-two participants (98%) completed the follow-up (Table 1). During the follow-up period participants in the SMBG group were able to maintain the achieved reduction of HbA1c (−0.5±1.4% vs. baseline [P<0.05]), body weight (−1.6±3.0 kg [P<0.001]), BMI (−0.5±1.0 kg/m2 [P<0.001]), and waist circumference (−1.7±3.5 cm [P<0.001]) (Fig. 1). Low-density lipoprotein cholesterol levels were also significantly lower during follow-up compared with baseline (−0.3±1.2 mg/dL [P<0.05]). In the control group HbA1c increased significantly (P<0.05) during follow-up compared with the end of the study, reaching baseline levels again.
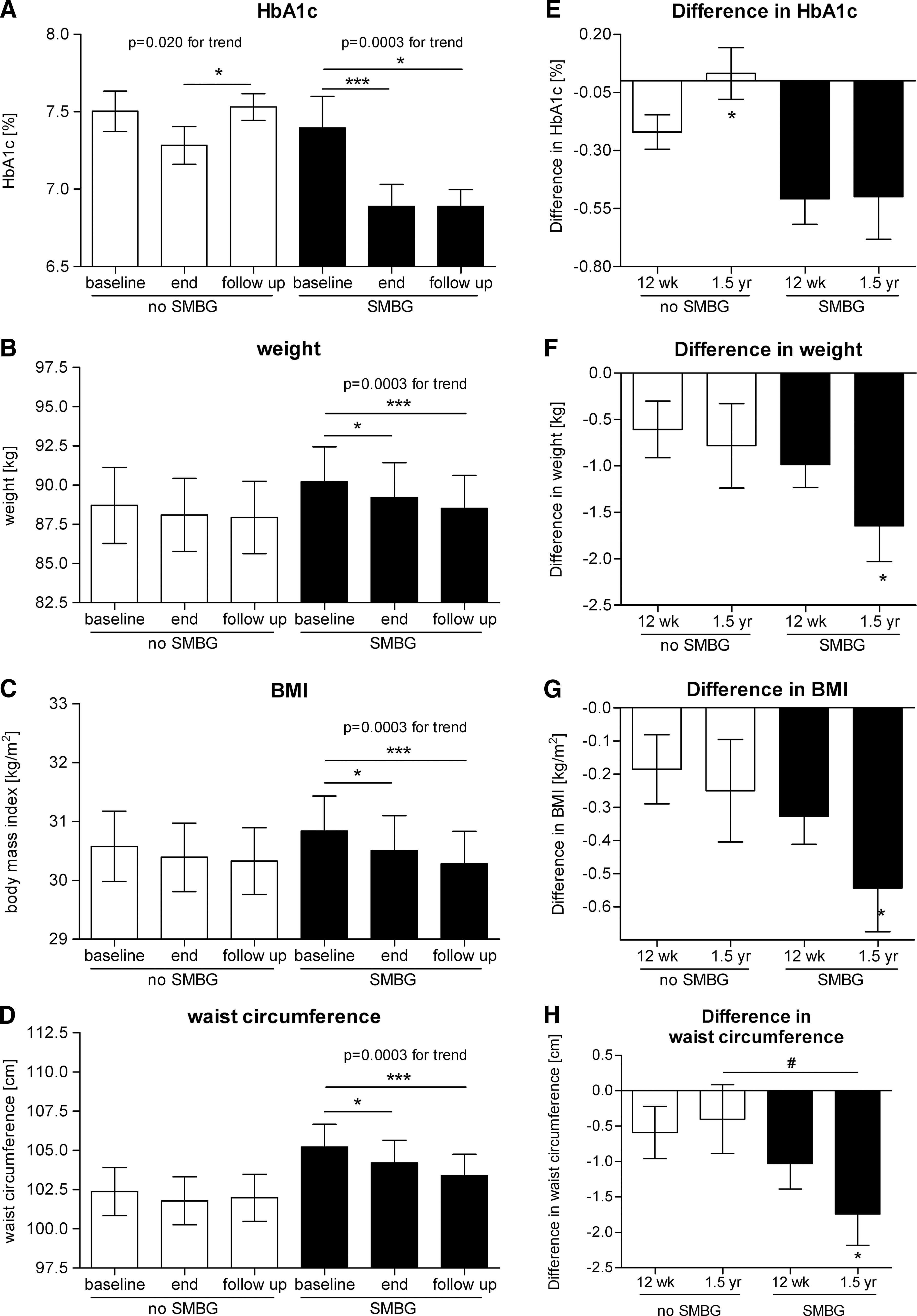
Improvements in
Metformin medication increased during the study and follow-up period
Patients in the control group were treated with a mean of 2,455±679 mg/day metformin at baseline, 2,494±743 mg/day at the end of the study (39±367 mg/day), and 2,773±405 mg/day (total increase of 318±474 mg/day [P<0.01]) after 1.5 years of follow-up (P<0.0001 for trend). Metformin dose in the SMBG group increased as well, from 2,172±892 mg/day at baseline to 2,348±796 mg/day at the end of the study (an increase of 177±532 mg/day) and to 2,620±499 mg/day (total increase of 448±710 mg/day [P<0.001]) at the time of follow-up. Although there was a significant increase within both groups over time, medication was not significantly different between groups at any time. In order to estimate whether HbA1c reduction in the SMBG group could be due to the increased metformin dose, we correlated HbA1c levels at time of follow-up with metformin dose, but no significant correlation was observed for the SMBG group (Fig. 2). However, a weak correlation was established in the control group (r=0.261; P=0.044). In contrast, HbA1c was strongly correlated with SMBG (i.e., the number of blood glucose measurements per day) (r=−0.484; P<0.0001).

Correlation of glycated hemoglobin (HbA1c) levels versus medication and versus self-monitoring of blood glucose (SMBG). Associations between HbA1c levels and
Participants who continued SMBG further improved their HbA1c level during 1.5 years of follow-up
During the follow-up participants of the SMBG group were asked how often they had performed SMBG after the end of the study. Eighty-seven percent reported having continued SMBG and to have performed a mean of 3.4±3.0 blood glucose measurements per week, despite not having been provided with test strips. Sixty-two percent of the participants continued to measure their blood glucose three or fewer times per week (with a mean of 1.4±1.1 measurements), whereas 38% measured more than three times per week (with a mean of 6.8±1.9 measurements per week). According to those two categories of SMBG performance, a stratified analysis was performed. HbA1c values of both groups were not significantly different at baseline. Compared with the baseline values, participants who measured their blood glucose more than three times per week demonstrated HbA1c reduction of 0.52±0.74% at the end of the study (from 7.3±1.8% to 6.8±1.4%) and an even greater reduction of 1.02±1.47% (P=0.014) at the time of follow-up ending up (Fig. 3) with a final HbA1c of 6.3±0.5% (P<0.01 vs. baseline). In contrast, those participants who measured three or fewer times per week also showed an improvement in HbA1c of 0.49±0.95% (from 7.4±1.5% to 6.9±1.0%) by the end of the study. However, their HbA1c level significantly increased again up to 7.2±0.9% (P<0.05) after 1.5 years, resulting in a significantly lower HbA1c reduction of only 0.19±1.35% (P=0.006) compared with the group performing more than three blood glucose measurements per week.

Glycated hemoglobin (HbA1c) level improvements due to the frequency of self-monitoring of blood glucose (SMBG) performance. Data are mean±SEM values.
Performance of SMBG and a high baseline HbA1c level are the only parameters that could explain maintenance of HbA1c reduction during follow-up
We performed logistic regression analysis in order to find out if the HbA1c reduction could be explained by confounders (Table 2). We found that performance of SMBG with an odds ratio (OR) of 3.62 (95% confidence interval [CI] 1.42–9.23) significantly contributed to the observed HbA1c level reduction. The effect remained stable (OR 4.48 [95% CI 1.16–12.86]) after adjustment for baseline parameters. In the fully adjusted model, when HbA1c level reduction during the study period and alteration of metformin dose were included, the effect even increased, indicating that the chance for HbA1c level reduction had an OR of 4.99 (95% CI 1.61–15.45) if SMBG was performed. The only other parameter with significant contribution to successful HbA1c level reduction was high baseline HbA1c level (OR 5.18 [95% CI 2.30–11.68]).
Logistic regression was used to identify those baseline parameters that could explain glycated hemoglobin (HbA1c) reduction. Shown are odds ratios (ORs) and confidence intervals (CIs).
Adjustment to self-monitoring of blood glucose (SMBG), age, diabetes duration, and baseline HbA1c.
Adjustment to SMBG, age, diabetes duration, baseline values of HbA1c, weight, triglycerides, systolic blood pressure, diastolic blood pressure, total cholesterol, low-density lipoprotein (LDL) cholesterol, and high-density lipoprotein (HDL) cholesterol.
Adjustment to SMBG, age, diabetes duration, baseline values of HbA1c, weight, triglycerides, systolic blood pressure, diastolic blood pressure, total cholesterol, LDL cholesterol, HDL cholesterol, HbA1c level reduction during study period, and adjustment of metformin dose.
Parameters having a significant contribution.
Discussion
In our study non–insulin-treated T2DM patients in the SMBG group significantly reduced their HbA1c, body weight, BMI, and waist circumference, and those improvements could be maintained for 1.5 years of follow-up. No significant improvements were observed in the control group. Metformin dose was increased in both groups, although there was no association between metformin daily dose and final HbA1c levels. Indeed, HbA1c was strongly associated with the number of blood glucose measurements, and participants who performed more than three SMBG measurements per week could reduce their HbA1c levels by more than 1% after 1.5 years of follow-up. The only explanatory factors for successful maintenance of HbA1c level reduction during follow-up were performance of SMBG and higher baseline HbA1c level. Therefore, the ROSSO-in-praxi-international trial explicitly demonstrates that SMBG not only supports the improvement of glucometabolic parameters in non–insulin-treated T2DM patients when added to a lifestyle intervention, but by continuous performance it could maintain glucometabolic control in the long term.
In recent years there has been a vigorous discussion about the benefit of SMBG. Published randomized controlled trials concerning SMBG in T2DM patients have not reached a consistent conclusion, especially in non–insulin-treated patients. As a consequence, there is worldwide variability in the use of glucose test strips and policies on reimbursement. 10 SMBG per se is a diagnostic procedure and not an intervention. 11 The real intervention is the lifestyle change, but clinical trials often compare different types of intervention versus outcome with different strategies for SMBG-guided disease management, leading to biased conclusions about the effect of SMBG. In many of the published studies patients also have not been advised how to use their SMBG measurements to support their lifestyle change. In this context, the analysis by Schwedes et al. 12 clearly demonstrated that SMBG in combination with a defined counseling algorithm is successful in reducing the HbA1c level. Our study design compared the effect of SMBG added to a manual-based lifestyle intervention. Therefore, it could be excluded that a different intervention design could have an impact on the results. Moreover, our results are supported by a comprehensive systematic review and meta-analysis. 13 On the basis of 12 trials, including a total of 2,943 patients, the authors demonstrated a benefit on HbA1c (weighted mean difference of −0.31% [−0.44; 0.17]) for those T2DM patients who performed SMBG compared with those who did not measure their blood glucose. Detailed analyses further revealed that self-management instruction and the treatment algorithm have had a significant impact on HbA1c level reduction, with the effects on HbA1c being greater the longer the follow-up period.
Normally, glucometabolic control worsens during the years after diabetes diagnosis. The United Kingdom Prospective Diabetes Study demonstrated for a period of 15 years after diagnosis that patients with T2DM show an increase in HbA1c level 14 with a lower increase with intensive pharmacological treatment than with conventional therapy. After a period of 2 years with conventional treatment there was an increase in HbA1c level of about 0.1%, which seems to be comparable with the increase of 0.2% in HbA1c level (nearly back to baseline levels) that we observed in the control group during follow-up in the ROSSO-in-praxi-international trial. In contrast, in the SMBG group an HbA1c level reduction of 0.5% could be maintained during the follow-up period of 1.5 years. This difference might be explained by the fact that during the study the participants learned how to use SMBG to control their dietary pattern and physical activity and how to change their lifestyle in order to reach good blood glucose values. We have proven the efficacy of this manual-based intervention on lifestyle change before in a group of 327 non–insulin-treated T2DM patients in Germany. 7 During the 12 weeks of intervention they significantly reduced their body weight and HbA1c level. Participants who continued to perform SMBG daily maintained the achieved reduction of 0.3% in HbA1c level during the follow-up period of 2 years. 8 Indeed, in the present study the SMBG group demonstrated an overall HbA1c reduction of 0.5%, whereas those who had continued to measure their blood glucose more than three times per week had an overall improvement of 1.0%. Therefore, our results clearly demonstrate (1) that the increase observed in the control group fits to the normal development of the disease (as shown by the United Kingdom Prospective Diabetes Study), (2) that participants in the SMBG group could maintain the achieved HbA1c level reduction over time, and (3) that those who continued to perform more than three blood glucose measurements per week reached a final HbA1c level improvement of 1.0%. These results imply that those individuals who are able to identify the relationship between their nutrition/physical activity and their blood glucose levels and to use this knowledge to improve their lifestyle benefit from SMBG in the long term. Moreover, the high percentage of those who actually continued to perform SMBG (87%) confirms that SMBG and SMBG-structured lifestyle changes can easily become integrated into general diabetes care. On the other hand, these results clearly demonstrate that a continuous usage of SMBG is necessary, as otherwise unfavorable lifestyle behaviors might creep in.
So far, it has not been clear whether lifestyle guidance has an effect on long-term outcomes. The ROSSO study provided some indirect evidence and demonstrated a significant correlation between use of SMBG and lower risk for fatal or nonfatal end points. 9 In this retrospective epidemiological cohort analysis no specific SMBG-based education program was used, and the only inclusion criterion for the SMBG group was performance of SMBG for at least 1 year. It is interesting that the ROSSO study could not identify any other independent factor than SMBG to explain the strong effect on the clinical outcomes, and therefore SMBG-induced lifestyle changes are presumed to be responsible for this effect. 15 Our results strengthen this hypothesis as we observed a significant decrease of HbA1c level in the SMBG group. For further studies, it would be interesting to learn more about what the patients changed during the intervention and follow-up. Food and activity records, food frequency questionnaires, and questionnaires about decision-making may help to further refine the intervention to focus on the key aspects of what most affects different patients.
In the present study SMBG was used as an additional tool in manual-based lifestyle guidance. Our results demonstrate that this short-term, highly motivational, and low-cost guidance can easily be implemented into general diabetes care and strengthen patient empowerment in order to change lifestyle and to improve glucometabolic control.
Footnotes
Acknowledgments
We thank Roche Diagnostics for providing blood glucose meters, test strips, and needle pricks used in the study.
Author Disclosure Statement
K.K. and S.M. have received fees for lectures and consultancy from Roche Diagnostics. T.T. has received fees for lectures from Roche Diabetes Care.